Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
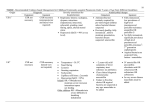
Indiaclen Short course of Amoxicillin in treatment of Pneumonia (ISCAP) 3 versus 5 days amoxicillin for treatment of non-severe pneumonia in young children: a double blind, placebo controlled multi-centric randomized trial Funding Agency USAID through IndiaClen/INCLEN Study Location - Mumbai - Lucknow - Nagpur - New Delhi - Chandigarh - Trivandrum - Vellore C N.D L N M T V C=Chandigarh N.D= N. Delhi, L=Lucknow, N=Nagpur, M=Mumbai, T=Trivendrum, V=Vellore BACKGROUND • ARI is the biggest killer of under 5 children in developing countries including India. • ARI Control Programme in India recommends cotrimoxazole as first line drug for non-severe pneumonia. • Reports of significant in vivo and in vitro resistance to cotrimoxazole. • Clinical studies showing high treatment failure with cotrimoxazole. Objectives Primary To compare the proportions of children recovering on 3-day versus 5-day treatment with oral amoxicillin in children aged 2-59 months presenting with non-severe pneumonia, with or without wheeze Objectives Secondary To compare Proportion who relapse within the next 6-14 days of observation Proportion who had resistant strains of S.pneumoniae and H.influenzae in nasopharyngeal cultures at the time of enrollment and at 12-14 days follow-up Direct medical cost of treatment of clinical failures and relapses in both groups (Data not shown) Outcome Measures Clinical Cure- on day 6 Clinical failure- Till day 6 Clinical relapse days 7-14 DEFINITIONS Clinical cure: Return of respiratory rate to age specific WHO cut off. Clinical Failure: Development of chest indrawing with danger signs or persistence of fast breathing at day 3 or later leading to therapy change. Relapse: Development of signs of pneumonia between day 6 -14. Inclusion Criteria Children aged 2 - 59 months with non-severe pneumonia (WHO defined) Written informed consent Exclusion criteria severe pneumonia or very severe disease (WHO defined) severe malnutrition other infectious conditions requiring antibiotics therapy clinically recognized congenital heart disease known or clinically recognized chronic systemic disorder history of repeated wheezing including physicians diagnosed asthma hospitalization in past 2 weeks use of antibiotics in previous 2 days measles within the last month known history of penicillin allergy prior enrollment in the study Sample Size Calculated to test equivalence hypothesis to detect difference of 4.5% using one sided t- test and 90% power, assuming 12% failure rate with amoxycillin Required number of patients was 950 in each group Intervention Scored amoxicillin dispersible tablet (125 mg/tablet) for the first three days 4-6 kg ½ tablet per dose 7-10 kg 1 tablet per dose 11-15 kg 1 ½ tablets per dose 16-20 kg 2 tablets per dose Effective dose per kg body weight – 31 to 54 mg/day For the next two days they received either amoxicillin or placebo FINAL OUTCOME 3 days = 1095 5 days = 1093 1st follow-up Failure = 68 Resolved = 1027 Failure =73 Resolved = 1020 Resolved = 983 2nd follow-up Failure= 47 Resolved = 980 Failure= 37 Relapse=32 Cured = 948 Relapse= 29 3rd follow-up Cured = 954 Results Table 1: Loss to follow-up 3 day AMX N % 5 day Total AMX N % N % Absolute difference, C.I LTF Day 4 37 3.4 43 3.9 80 3.7 0.5 (-1, 2.0) LTF Day 6 62 5.7 67 6.1 129 5.9 0.4 (-1.5, 2.4) LTF Day 12-14 96 9.8 94 8.6 190 8.7 0.2 (-2.2, 2.5) Results Table 2: Adherence to treatment types 3-day AMX n % 5-day AMX n % Total n% p-value Adherence at 3 day 1031 94.2 1026 93.9 2057 94 0.78 Adherence at 5 day 937 85.6 928 84.9 1865 85.2 0.66 Results Table 3: Outcome Measures (Per Protocol) N 3-day AMX % N 5-day AMX % Absolute Difference 95% C.I Total recruited 1033 1026 Cure on day 6 980 94.9 983 95.8 0.9 (-0.9, 2.8) Relapse 32 3.3 29 3.0 0.3 (-1.2, 1.85) Results Table 5: Risk factors associated with failures by logistic analysis Variable Adjusted OR C.I Unadjusted OR C.I Excess Respiratory Rate more than 10 bmp 2.82 2.8 (1.8, 4.45) (1.5, 5.2) Non-Adherence at 5 days 11.57 (7.4, 18.0) - RSV positivity 1.95 (1.0, 3.8) 13.1 (8.5, 20.2) 2.1 (.9, 4.9) SP resistant Time 0 SP resistant Time 2 3 day AMX HI resistant Time 0 5 day AMX 62.2 57.4 61.2 54.4 78.2 66.7 66.1 100 80 60 40 20 0 66.6 Resistance pattern of isolates in two treatment types HI resistant Time 2 CONCLUSIONS 1. Oral amoxicillin for 3 days is as effective clinically as 5 days in the treatment of children 2-59 months old suffering from non severe pneumonia. 2. In S. pneumoniae on day 12 – 14 an increased in-vitro resistance to cotrimoxazole with 5 day treatment seen. RECOMMENDATIONS For the treatment of non-severe pneumonia in children 2 to 59 months of age the National ARI Control Programmes already using amoxicillin as first line drug should consider 3 day antibiotic therapy