Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
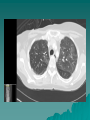
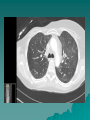
HPI 49 year old woman with metastatic breast cancer seen in the hospital for fever and SOB Right breast cancer (infiltrating ductal ca) diagnosed in 2001 at age 38 – Treatment included mastectomy (negative lymph nodes), doxarubicin and cytoxan (4 courses) HPI Patient did well until March 2010 when erythema over right chest noted – Biopsy + adenoca c/w breast Breast ca: “triple negative” – Estrogen receptors – Progesterone receptors – Her2 Staging PET scan demonstrated multiple positive lymph nodes: mediastinum, supraclavicular and bone mets Treatment Course Radiation June to chest wall 2010 – Received Paclitaxel and Bevacizumab – Also given Zometa for bone mets – Stopped in Dec 2010 due to toxicity April 2011 – Started Gemcitabine/Carboplatin and Iniparib (experimental protocol) Treatment Course October 2011 – Brain mets noted and patient started stereotactic brain radiation, also given dexamethasone Dexamethasone mid-December December stopped in 27, 2011 – Admitted with fever and SOB PMH/FH/SH/Meds Prothrombin mutation noted on initial heme eval - prophylactically started on warfarin in 2010 Family history of breast CA Non-smoker, Meds: no unusual exposures omeprazole, metoprolol, warfarin Physical Exam/Lab VS – Current temp 37 (prior to 37.9) – Pulse 110 – On 02 3 LPM Chest: Bilateral crackles, most prominent at bases No other physical findings H/H 11.8/33.9 WBC 5.1 Plt 64 INR 1.58 ESR >100 CRP 213 CT Chest - Radiology Diffuse groundglass opacities and scattered centrilobular nodules. Differential includes cardiogenic or noncardiogenic pulmonary edema, infection and drug reaction. Clinical Course Started on antibiotics (Zosyn, Levaquin) Negative: cocci serology, PCR of nasal swab for influenza and mycoplasma antibodies Bronchoscopy on 12/29 with BAL done BAL Fluid slightly hemorrhagic, did not clear with repeated lavage Smears/cultures negative Negative aspergillus antibody in BAL Negative PCR for PCP and legionella Clinical Course Patient continued to have low-grade fever –Oxygen requirements increased BAL cultures remained negative VATS lung biopsy done on 1/5/12 –? infection –? drug toxicity Pathology Report Fibrinous acute lung injury with increased alveolar macrophages, scattered multinucleated giant cells and increased extravascular tissue eosinophils. The overall histopathology favors drug toxicity over other possibilities. Clinical Course Patient started on corticosteroid therapy All cultures remained negative Was discharged on 1/7/12 on prednisone 60 mg/day F/U in pulmonary clinic on 2/8/12 – Clinically improved Clinical Diagnosis: Drug-induced Lung Injury – Likely due to Gemcitabine Patient most recently receiving gemcitabine/carboplatin/iniparib Onset of respiratory symptoms was delayed several months after last dose – delay due to dexamethasone treatment for brain mets? Gemcitabine Lung Toxicity Acute dyspnea with infusion in 10% 3 types of acute pneumonitis: – Capillary leak syndrome – Diffuse alveolar damage – Alveolar hemorrhage Frequency is low: 0.27% Gemcitabine Lung Toxicity Reduction in DLco within 2 months of treatment reported in 24%, often self-limited (more frequent in women, older age, low baseline DLco) Some cases of pulmonary fibrosis reported, but rare Ann Onc 2004 Gemcitabine Lung Toxicity Factors increasing risk of lung injury include other chemotherapy (including paclitaxel), chest radiation Mortality rate with acute pneumonitis up to 20%, but rapid response to steroid therapy is reported Iniparib Poly(adenosine diphoshate-ribose) polymerase inhibitor (PARP) Recent phase 2 trial (NEJM, 2011;364:205) in metastatic “triple negative” breast cancer 123 patients given iniparib with or without gemcitabine/carboplatin Iniparib improved survival: 7.7 months vs 12.3 months Dyspnea reported, but no severe pulmonary complications from Iniparib in this study.


































![Your Lung Cancer Team [DRAFT 6]](http://s1.studyres.com/store/data/017182233_1-481dd7d8dceba4fe88e23a5f72206659-150x150.png)


