Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
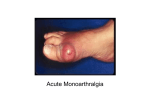
Septic and crystal arthritis Jaya Ravindran Rheumatologist Case 1 • 82 year old • Admitted 2.6.08 acute on chronic knee pain 3-4 days • Recent excision of shin BCC with skin graft complicated by cellulitis • Ex Not unwell afebrile MEWS O • Warm, slightly tender knee effusion, tolerating 90 flexion • ? Wound infection started on antibiotics • CRP 187 Case 1 • Radiological abnormality? • Differential diagnosis? • Further investigations? • Management? Case 1 • • • • No organisms, scanty WBC Pyrophosphate crystals Low dose colchicine CRP 42 Case 2 • DS 42 year old lady • PMH Crohns • Admitted 12.5.08 with onset of feeling hot and cold, D & V, headache 10 days ago • 3 days ago developed painful swelling left wrist, right knee and left ankle • SH Roadie, smoker – 10 roll-ups/day, lives with husband and son Case 2 • Ex unwell,T38.5, p117/min, BP 116/64, RR20/min, satn 91% air, urine nad • Tender swollen and red wrist, knee and ankle • CXR ‘clear’ • IMP septic • Plan BC, analgesia, iv antibiotics, IVI • Systolic dropped to 90 systolic • Na 122 CRP 285, Blood gas P02 7, PCO2 7 PH 7.4 • Transferred to WGH Case 2 • Seen by rheumatologist joints aspirated • 13.5 blood cultures group A Strep, aspirate no growth, WBC • 15.5 vasculitic rash, low complement ?post Strep • 16.5 ECHO normal, CRP and joints settling • 17.5 Right pleuritic chest pain with rub Case 2 • P02 8 treat for PE as well • 21.5 CTPA cavitating consolidation right lower lobe, hilar nodes, no PE • Still spiking ?empyema – nil aspirated,, no AFB in sputum, HIV negative, awaiting WBC scan Case 3 • DB 45 year old man • PMH RA on sulphasalazine • 4 day history painful hot swollen red right big toe • Differential? • Investigations? Case 4 • • • • 82 year old man PMH LVF,AF, TIA, BPH DH Aspirin, bumetanide, ramipril, digoxin, statin Referred with acute on chronic wrist pain needing MST • Pain was so severe that he asked next door’s dog to stop barking! • WBC 13, CRP 155, Cr 143, XR OA changes Case 4 • • • • • • Ex Well afebrile MEWS 0 Tender warm swollen right wrist Dry tap Imp ? Crystal Oral prednisolone Good response but then confused, t 37.5, p116/min, 3+ blood & 1+ prot urine dip, increasing painful swelling in left wrist and toe • Diagnosis and plan? Case 4 • WBC 20, Cr 261 • MSU, BC and joint aspirated • IVI and antibiotics, MST and ramipril stopped • Uric acid crystals, no growth in aspirate • Wrists injected once presumed UTI treated • Wrists better, CRP 3, Cr 124 What are other differentials for monoarticular pain? Monoarthritis - differential • Monoarticular sero-ve spondyloarthritis eg psoriatic and reactive arthritis • Monoarticular RA Monoarthritis - differential • Haemarthroses (warfarin, bleeding disorders) • Trauma – fracture, internal derangement, haemarthroses Others to think about • Osteonecrosis/AVN (steroids/alcohol/SLE) • Prosthetic joint loosening, # or infection Others to think about • Periarticular pathology • Cellulitis Septic arthritis • 15-30 per 100,000 population • Fatal in 11% of cases in UK • Delayed or inadequate treatment leads to irreversible joint damage How do you get septic arthritis? Pathogenesis Who gets septic arthritis ? Who gets septic arthritis? • pre-existing joint disease • prosthetic joints • low SE status, IV drug abuse, alcoholism • diabetes, steroids, immunosuppression • Skin lesions e.g. ulcers, particularly in context RA often source of infection • Which organisms cause septic arthritis? Which organisms? • common organisms Staphylococci or Streptococcus • Elderly & immunocompromised gram -ve organisms Which organisms? • • • Anaerobes more common with penetrating trauma Pseudomonas - IV drug abusers young adults - significant incidence gonococcal arthritis Who gets septic arthritis? • poor prognostic features: older pre-existing joint disease & presence of synthetic material within joint What are the signs and symptoms of septic arthritis? Symptoms & signs of septic arthritis • Symptoms usually present for < 2/52 • Typically hot, swollen, red tender joint with reduced range of movement, difficulty weight bearing • Night and rest pain • Large joints more commonly affected than small • majority of joint sepsis in hip or knee • Systemic upset (MEWS) Symptoms & signs of septic arthritis • In pre-existing inflammatory joint disease symptoms in affected joint(s), out of proportion to disease activity in other joints. • 10% of cases > one joint • presence of fever not reliable indicator • Features of gonococcal arthritis ? Gonococcal arthritis • • • • Women>men Menses, pregnancy 1-3% arthritis 1day- weeks after sexual encounter • Migratory (70%), Tenosynovitis (70%), monoarthritis (32%), polyarthritis (10%) • Fever, Dermatitis (pustules, vesicular, haemorrhagic bullae, mac.papular) What investigations are useful in septic arthritis? Investigations • Synovial fluid aspiration – gram stain/m,c,s – Absence of organism does not exclude septic arthritis – polarised light microscopy (crystals) – NB suspected prosthetic joint sepsis should ALWAYS be referred to orthopaedics Investigations • Blood cultures • Significant proportion blood cultures + ve in absence of + ve synovial fluid cultures • FBC ESR & CRP • Absence of raised WBC, ESR or CRP does not exclude diagnosis of sepsis Other investigations • CRP useful for monitoring response to treatment • Urate may be normal in acute gout • U+E & LFT – prognosis and influence antibiotic regime Other tests? • • • Gonococcal - skin pustule - skin swab, urethral/cervical /rectal/throat swab, blood culture, joint aspirate genitourinary or respiratory tract infection then culture sputum and CXR & MSU If periarticular sepsis – appropriate swabs and cultures • Radiology ? Imaging • Plain X rays no benefit in diagnosis but form baseline for any future joint damage. May show chondrocalcinosis (pyrophosphate arthritis). • MRI sensitive for osteomyelitis and spinal involvement Imaging • Ultrasound useful in guiding needle aspiration eg hip • White cell scanning helpful in diagnosing prosthetic sepsis • What are the radiological features of infected prosthesis? Prosthetic infection Spinal infection • Discitis – with destruction end plates • Management? • MEWS score? • Shock? • Multi-organ failure? • RESUSCITATION Antibiotic treatment of septic arthritis • Local and national guidelines • Liaise with micro. guided by gram stain • Conventionally given iv for 2 weeks or until signs improve, then orally for around 4 weeks Joint drainage & surgical options • medical aspiration, surgical aspiration via arthroscopy or open arthrotomy • Suspected hip sepsis – early orthopaedic referral – may need urgent open debridement Recommendations specific to 1o care & emergency department • commonest hot joint to present in 1o care is 1st MTP gout • diagnosed on clinical grounds without needle aspiration or referral to hospital. (Make referral if inadequate recovery) • Some GPs aspirate & inject joints for inflammatory arthritis or osteoarthritis. If withdraw pus/unexpected cloudy fluid should send sample with patient to local emergency department Recommendations specific to 1o care & emergency department • GPs & doctors in EAU should refer patients with suspected septic arthritis to specialist with expertise to aspirate joint. • May be orthopaedic surgeon or rheumatologist • Admit if sepsis is suspected or confirmed. Summary • with a short history of a hot, swollen, tender joint (or joints) plus restriction of movement; septic arthritis until proven otherwise • If clinical suspicion high investigate & treat as septic arthritis even in absence of fever – always joint aspiration and blood cultures GOUT • Definition and metabolism? Gout • An inflammatory arthritis caused by hyperuricaemia • Uric acid is formed from the breakdown of purines (DNA) • Excreted in the urine • Characterised by the deposition of urate crystals in the joints and soft tissues Gout Epidemiology • Prevalence 1-2% • Most common cause of inflammatory arthritis in men 3-5:1 and postmenopausal women • Usually presents between 40-60 years • Diagnosis of gout ? Polarized microscopy - negatively birefringent needle shaped crystals Clinical - usually self-limiting monoarthritis • Usually resolves 7-10 days Diagnostic criteria for gout – ACR criteria • • • • • • • • • • • • • > 1 attack of acute arthritis Maximum inflammation within 1 day Attack of monoarthritis Redness over joints Painful or swollen 1st MTP Unilateral attack 1st MTP Unilateral attack tarsal joint Tophus Hyperuricaemia Asymmetric swelling within joint on x-ray Subcortical cysts without erosions on x-ray Joint fluid culture –ve for organisms 6 or more criteria Chronic gout • Up to 10 years to develop • Less painful • Older age • Tophi – hands, feet, elbows, ears • Erosions • Poly/oligoarticular Erosive gout • Causes of gout ? Classification of Gout 1. Primary Gout: Majority • Causes either over-production (10%) or underexcretion of uric acid (90%). 2. Secondary Gout: • increased formation of uric acid • reduced excretion of uric acid • drugs / toxins • miscellaneous Increased Production of Uric Acid High alcohol esp beer or dietary intake esp high seafood and meat Increased Production of Uric Acid Increased purine turnover: • Lympho/myeloproliferative disorders • Tumours • Muscle necrosis • Chronic Haemolysis • Severe psoriasis Reduced Excretion of Uric Acid • • • • • Chronic renal disease Hypertension Hypothyroidism Hyperparathyroidism Drugs Drug induced hyperuricaemia • • • • • Diuretics esp.thiazides Low dose aspirin Cytotoxics Cyclosporin Ethambutol and pyrazinamide • Associated diseases and triggers gout? Associations • • • • Hypertension Obesity Hypercholesterolaemia Diabetes Triggers of gout • • • • • • • Minor trauma Operations Unaccustomed exercise Dietary excess Alcohol Dehydration Starting diuretics Useful investigations • U+E, glu, BP, urate at 4 weeks • Pyrophosphate arthritis features ? Clinical • Acute monoarthritis in elderly esp in hospital • Chronic polyarthritis with hypertrophic OA changes Chondrocalcinosis • Polarized microscopy features? • Metabolic Causes? • Triggers? Pyrophosphate Crystals Metabolic Causes of pyrophosphate arthritis • • • • Haemochromatosis Hyperparathyroidism Hypophosphatasia Hypomagnasaemia Triggers of pyrophosphate arthritis • Management of gout? Management of acute gout • Affected joints should be rested (C) and analgesic, anti-inflammatory drug therapy commenced immediately, and continued for 1–2 weeks (A). • Fast-acting oral NSAIDs at maximum doses are the drugs of choice when there are no contraindications (A). • In patients with increased risk of peptic ulcers, bleeds or perforations, co-prescription of gastro-protective agents should follow standard guidelines for the use of NSAIDs and Coxibs (A). • Colchicine can be an effective alternative but is slower to work than NSAIDs (A). In order to diminish the risks of adverse effects (especially diarrhoea) it should be used in doses of 500 µg bd–qds (C). Management of acute gout • Allopurinol should not be commenced during an acute attack (B) but in patients already established on allopurinol, it should be continued and the acute attack should be treated conventionally (A). • Opiate analgesics can be used as adjuncts (C). • Intra-articular corticosteroids are highly effective in acute gouty monoarthritis (B) and i.a, oral, i.m or i.v corticosteroids can be effective in patients unable to tolerate NSAIDs, and in patients refractory to other treatments (A). • If diuretic drugs are being used to treat hypertension, an alternative antihypertensive agent should be considered, but in patients with heart failure, diuretic therapy should not be discontinued (C). Recommendations for diet, lifestyle modification and non-pharmacological modalities of therapy • In overweight patients dietary modification to achieve ideal body weight should be attempted (B), but ‘crash dieting’ (B) and high protein/low carbohydrate (Atkins-type) diets (C) should be avoided. • Inclusion of skimmed milk and/or low fat yoghurt, soy beans and vegetable sources of protein and cherries, in the diet should be encouraged (B). • Intake of high purine foods and red meat should be restricted (B). Liver, kidneys, shellfish and yeast extracts should be avoided (B), and overall protein intake should be restricted (C). • Patients with gout and a history of urolithiasis should be encouraged to drink >2 l of water daily (B) and avoid dehydration (C). Alkalinization of the urine with potassium citrate (60 mEq/day) should be considered in recurrent stone formers (B). Recommendations for diet, lifestyle modification and non-pharmacological modalities of therapy • Alcohol consumption should be restricted to <21 units/week (men) and 14 units/week (women) (B), and patients should be encouraged to have at least 3 alcohol-free days per week (C). Beer, stout, port and similar fortified wines are best avoided (C). • Affected joints should be elevated and exposed in a cool environment (C). ‘Bed cages’ (C) and ice packs (B) can be effective adjuncts to therapy. • Trauma to joints (B) and intense physical exercise (B) should be avoided but moderate physical exercise encouraged (B). Management of recurrent, intercritical and chronic gout • The plasma urate should be maintained below, 300 µmol/l (C). • In uncomplicated gout uric acid lowering drug therapy should be started if a second attack, or further attacks occur within 1 yr (B). • Uric acid lowering drug therapy should also be offered to patients with tophi (C), patients with renal insufficiency (B) patients with uric acid stones and gout (B) and to patients who need to continue treatment with diuretics (B). • Commencement of uric acid-lowering drug therapy should be delayed until 1–2 weeks after inflammation has settled (C). • Initial long-term treatment of recurrent uncomplicated gout normally should be with allopurinol starting in a dose of 50–100 mg/day and increasing by 50–100 mg increments every few weeks, adjusted if necessary for renal function, until the therapeutic target (SUA <300 µmol/l) is reached (maximum dose 900 mg) (B). • NB renal impairment, elderly, azathioprine Management of recurrent, intercritical and chronic gout • Uricosuric agents can be used as second-line drugs in patients who are under-excretors of uric acid and in those resistant to, or intolerant of, allopurinol (B). The preferred drugs are sulphinpyrazone (200–800 mg/day) in patients with normal renal function or benzbromarone (50–200 mg/day) in patients with mild/moderate renal insufficiency (B). • Colchicine 0.5 mg bd should be co-prescribed following initiation of treatment with allopurinol or uricosuric drugs, and continued for up to 6 months (A). In patients who cannot tolerate colchicine, an NSAID or Coxib can be substituted provided that there are no contraindications, but the duration of NSAID or Coxib cover should be limited to 6 weeks (C). • Aspirin in low doses (75–150 mg/day) has insignificant effects on the plasma urate, and should be used as required for cardiovascular prophylaxis (B). However, aspirin in analgesic doses (600–2400 mg/day) interferes with uric acid excretion and should be avoided (B). Other drugs and diseases • consider losartan and fibrate if hypertensive and hyperlipidaemia (uricosuric) • Screen for and treat metabolic syndrome THANK-YOU