Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
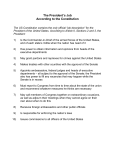
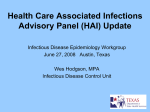
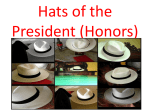
Senate Health and Human Services Committee Interim Charge #1 August 23, 2006 The Mental Health of Texans is Everyone’s Responsibility • DSHS’s Mental Health and Substance Abuse Services – Community-based services • 39 Local Mental Health Authorities • Dallas Area NorthSTAR Authority • 180 Substance Abuse contracts – 10 State Hospitals • Public Mental Health System – DSHS mental health services are only part of the public mental health system in Texas – Law enforcement, education, Medicaid, CHIP, the criminal justice system, hospitals and other entities all play major roles in treating Texans with mental illnesses Senate Health and Human Services Committee DSHS Presentation August 23, 2006 2 Number of Adults and Children (and Total) Served at DSHS Community Mental Health Centers from FY2003 to FY2006 Year-to-Date Children Adults Total 150,000 135,743 110,491 131,344 129,744 107,558 105,131 129,400 103,659 100,000 50,000 25,622 22,499 26,213 25,741 0 FY2003 FY2004 FY2005 FY2006 Year-to-Date (September-June) Source: FY2003 = CARE Report HC028488, TDMHMR MH Priority Population Counts by Month for 09-01-02 through 08-31-03, prepared on 09/20/03, total is unduplicated; FY2004 = CARE Report HC028488, TDMHMR MH Priority Population Counts by Month for 09-01-03 through 08-31-04, prepared on 09/18/04, total is unduplicated; FY2005 = DSHS Mental Retardation and Behavioral Health Outpatient Warehouse, Business Objects Corporate Report, LBB RDM Served for FY2005, 08/01/06, used for LBB reporting for number of adults and children receiving community mental health services per year (i.e., number who received a full RDM service package); FY2006 Year-to-Date = DSHS Mental Retardation and Behavioral Health Outpatient Warehouse, Business Objects Corporate Report, LBB RDM Served for FY2006 September-June, 08/03/06, used for LBB reporting for number of adults and children receiving community mental health services per year (i.e., number who received a full RDM service package). Senate Health and Human Services Committee DSHS Presentation August 23, 2006 3 Number of Texans who Participated in Substance Abuse Prevention and Intervention Services in FY2005 119,920 46,186 331,016 989,569 Youth Prevention Youth Intervention Adult Prevention Adult Intervention Senate Health and Human Services Committee DSHS Presentation August 23, 2006 4 53,420 Texans Accessed Substance Abuse Treatment in FY2005 7,360 8,887 23,144 32,800 Youth Male Female Priority Female Estimated number in need of treatment is 1.6 million Texans Senate Health and Human Services Committee DSHS Presentation August 23, 2006 5 Resiliency and Disease Management (RDM) • Evidence-based • Intended to better match services to Mental Health consumers’ needs, and to use limited resources most effectively by providing the right service to the right person in the right amount to have the best outcomes. • Includes medication management, case management, skills training, family training, supports and partners, psychosocial rehabilitation, individual and group counseling, supported employment, supported housing, and Assertive Community Treatment (ACT) Senate Health and Human Services Committee DSHS Presentation August 23, 2006 6 RDM Key Components • Uniform Assessment • Standard Service Packages • Utilization Management • Data Analysis and Performance Evaluation • Jail Diversion Senate Health and Human Services Committee DSHS Presentation August 23, 2006 7 Percent of Adults and Children Served with RDM Receiving the Minimum Number of Recommended Monthly Service Hours 100% 85% 75% 80% 60% 71% 38% 40% 20% 83% 48% 60% 50% 29% Target = 85% 66% 57% 37% Adults Children 0% FY2005 FY2005 FY2005 FY2005 FY2006 FY2006 Quarter Quarter Quarter Quarter Quarter Quarter 1 2 3 4 1 2 Source: DSHS, Mental Retardation and Behavioral Health Outpatient Warehouse (MBOW), PM Service Package Minimum Hours. For methodology, see Fiscal Year 2006 Performance Contract with Local Mental Health Authorities, Information Item C. Senate Health and Human Services Committee DSHS Presentation August 23, 2006 8 RDM Outcomes • Outcomes for Adults in FY 2005: 78% with improved or stabilized functioning 88% with improved or stabilized risk of harm 82% with improved or stabilized housing 86% with improved or stabilized employment 91% with improved or stabilized criminal justice involvement 97% of adults who received the full benefits indicated avoided spending time in crisis (i.e., avoided being placed in 23-hour observation in a hospital setting, crisis counseling, etc.). Senate Health and Human Services Committee DSHS Presentation August 23, 2006 9 RDM Outcomes • Outcomes for Children in FY 2005: 80% with improved or stabilized functioning 92% with improved or stabilized risk of harm 92% with improved or stabilized school behavior 84% with improved or stabilized severe aggressive behavior 89% who avoided re-arrest 98% of children who received the full benefits indicated avoided spending time in crisis (i.e., avoided being placed in 23-hour observation in a hospital setting, crisis counseling, etc.). Senate Health and Human Services Committee DSHS Presentation August 23, 2006 10 FY2005 Texas Monthly Hospital Emergency Room (ER) Costs 31 Percent Lower for Medicaid Clients with Mental Illness or Substance Abuse Receiving DSHS Behavioral Health Treatment $115 ER Costs per Medicaid Client per Month Untreated $115 ER COST OFFSET - $36 Average per Client per Month 31% REDUCTION Treated $79 $0 Source: Prepared by Research Team, Strategic Decision Support, HHSC, 3/23/2006. Average of ER costs per month for Medicaid clients not receiving needed DSHS Mental Health and Substance Abuse services (Untreated) vs. average of ER costs per month for Medicaid clients receiving needed DSHS Mental Health and Substance Abuse services (Treated). Senate Health and Human Services Committee DSHS Presentation August 23, 2006 11 Crisis Services Redesign • February 2006, DSHS established the Crisis Services Redesign Committee to develop recommendations for a comprehensive array of crisis services. • Members of the committee include medical experts, citizen stakeholder groups, law enforcement representatives, county probate court judge representation, and county representatives, as well as individuals from professional organizations and provider groups. • A redesign of crisis services will build on, and is a part of, the service improvements made by the evidence-based Resiliency and Disease Management program. • A thorough review of the current crisis system was conducted, including holding public hearings around the state, reviewing current research and consultation with experts. Senate Health and Human Services Committee DSHS Presentation August 23, 2006 12 Crisis Services Redesign • The committee is considering a range of effective community-based interventions designed to intervene in and avoid crisis and the need for hospitalization, including: – 24-hour hotline – Mobile outreach – 23 to 48-hour hold capacity – On-call psychiatric services – Crisis residential services – Respite – In-home crisis resolution • Special Issues – Children’s issues – Forensic issues – Transportation Senate Health and Human Services Committee DSHS Presentation August 23, 2006 13 Behavioral Health Issues Impact Other Systems • 75% of children placed in foster care have parents with behavioral health problems • 75% of kids in the juvenile justice system have behavioral health problems • 30% of kids in the juvenile justice system will end up in the adult justice system • 46% of all ER visits have behavioral health issues as a basic or contributing factor • 30% of all truancy is related to behavioral health problems Senate Health and Human Services Committee DSHS Presentation August 23, 2006 14 Mental Health Transformation • Overarching goal is to improve the mental health of all Texans and support the development of state infrastructure for implementing the President’s New Freedom Commission goals. • New Freedom Commission Goals are shared by the 14 state agencies, client and family member representatives, and legislators participating on the Transformation Working Group, including: – The Governor’s Office; Dept of State Health Services; Texas Health and Human Services Commission; Dept of Family and Protective Services; Dept of Criminal Justice; Texas Juvenile Probation Commission; Texas Youth Commission; Consumers; Family Members; Texas Education Agency; Dept of Aging and Disability Services; Dept of Assistive and Rehabilitative Services; Workforce Commission; Veteran’s Administration; Housing and Community Affairs. Senate Health and Human Services Committee DSHS Presentation August 23, 2006 15 Mental Health Transformation • The 2 primary areas of focus: – Developing and supporting local behavioral health collaboratives – Using cutting edge technology to change work processes across agencies • Improvement of the system will be targeted to the following principles: – Apply evidence to health care delivery – Use information technology – Encourage continuous improvement – Prepare the workforce Senate Health and Human Services Committee DSHS Presentation August 23, 2006 16 Behavioral Health Integrated Provider System (BHIPS) • First statewide development of an electronic health record in the United States. • BHIPS is an Internet-based, non-proprietary computer system for behavioral health providers that supports a comprehensive service delivery system. • BHIPS offers tools for clinicians to ensure provision of consistent, quality services. • Using BHIPS, providers can easily meet state and federal requirements for reporting, including capturing required client and billing data. • Provider focus groups were used to gather input for the design of BHIPS to ensure that the system works in a clinical setting. • Security and privacy of information ensured by allowing a provider access only to data that they enter or have been allowed to access through the consent of the client. • BHIPS is the basis for other states’ use of Electronic Health Records. Senate Health and Human Services Committee DSHS Presentation August 23, 2006 17 Drug Demand Reduction Advisory Committee (DDRAC) • The 77th Texas Legislature passed Senate Bill 558, establishing the Drug Demand Reduction Advisory Committee (DDRAC) with a mandate to develop and coordinate a statewide strategy to reduce drug demand in Texas. • The DDRAC, with input from the public and private sectors, is to: – Serve as a single source of information for the Governor, the Legislature and the public about issues relating to reducing drug demand, including available prevention programs and services; – Develop a statewide strategy to reduce drug demand; – Identify lead or contributing agencies or offices to implement the strategy; and, – Coordinate the implementation of the strategy by those agencies or offices. Senate Health and Human Services Committee DSHS Presentation August 23, 2006 18 Drug Demand Reduction Advisory Committee (DDRAC) • Agencies participating in the effort include: – Office of the Governor, Criminal Justice Division (CJD); Department of /Public Safety (DPS); Health and Human Services Commission (HHSC); Texas Alcoholic Beverage Commission (TABC); Texas Department of State Health Services (DSHS); Texas Correctional Office on Offenders with Medical and Mental Impairments (TCOOMMI); Texas Department of Criminal Justice (TDCJ); Texas Department of Aging and Disability Services (DADS); Texas Department of Family and Protective Services (DFPS); Texas Education Agency (TEA); Texas Juvenile Probation Commission (TJPC); Texas Youth Commission (TYC); Texas Department of Transportation (TxDOT) Senate Health and Human Services Committee DSHS Presentation August 23, 2006 19 Drug Demand Reduction Advisory Committee (DDRAC) • Enabling legislation requires DDRAC to make recommendations to the Legislature. This year DDRAC recommendations will address issues including: – Reducing the risks of underage drinking – Reducing the risks associated with driving under the influence – Uniform Accident and Sickness Policy Provision Law (UPPL)/prevention of insurance exclusion for patients under the influence – Using SBIRT model in healthcare and social service settings • Collaborative concepts and action plans for DDRAC include: – Motivational interviewing training across agencies – Development of joint DSHS/Criminal Justice screening, assessment and placement protocols for adults and children Senate Health and Human Services Committee DSHS Presentation August 23, 2006 20 Integration of Behavioral Health and Primary Care: Project InSight Project InSight provides screening, brief intervention, and referral to treatment (SBIRT) as part of routine medical care in the Harris County Hospital District. • Findings: – One in five patients screen positive for substance abuse issues – Total cost savings after one year has been more than $4 million due to reduced utilization of emergency and inpatient services Senate Health and Human Services Committee DSHS Presentation August 23, 2006 21