Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
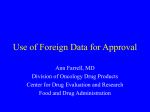
Bridging Studies Global Development W. Joe Shih Biostatistics Dept UMDNJ-School of Public Health Sept. 29, 2006 FDA/Industry Conference, Washington D.C. Clarification • Bridging studies: in the context of “ICH E5”. • ICH E5 includes drugs and biologics. • Not the ‘vaccine immunogenicity bridging trials’ (which are conducted when manufacturing processes or storage conditions are changed after vaccine licensure for improving production yields and vaccine stability or shelf life). New Trend • Moving from “Bridging study” toward “Global trial” • More fruitful to discuss issues with “Global trial” design and analysis My presentation: ½ “Bridging” ½ “Global” Purpose of ICH E-5 • "To facilitate the registration of medicines among ICH regions – US/EU/Japan…” (now expanded to other countries) • “To provide guidance on regulatory and development strategies …" Extrapolate foreign clinical data and evaluate influence of ethnic factors Minimize duplication of clinical studies Supply medicine expeditiously to patients Difficulties • “Ethnicity” is a not a simple nor precise concept • Political and cultural sensitivities (involving international trade of pharmaceuticals - WTO) • Lack of consensus even regarding need for such a guidance A compromise concept in E5: "Bridging data package" = ‘Selected information from the complete clinical data package (CCDP) that is relevant to the population of the new region’ + (if needed) ‘Bridging study(ies) in the new region.’ Difficulties • No gold standards of “bridging studies” • Heterogeneity among regulatory agency, industry, and academia in the interpretation of the ICH guideline; e.g. what is “extrapolation” of foreign data? how to evaluate the “bridging evidence”? Practical Issues • What type of bridging studies are required? – Clinical studies? – PK/PD studies? • Sample size of a bridging study? Not all regions/countries act the same way Market size seems matter very much (unfortunately) Japanese Experience Japanese Drug Organization (‘Kiko’, or OPSR): “All the examples of bridging studies raised by the DO are phase II/III studies which would have to be performed exclusively in Japan.” (In addition to PK/PD.) Naito, C. ‘Acceptance of foreign clinical data and bridging studies.’ Proceedings of the 19th conference on Japanese Society of Clinical Pharmacology and Therapeutics. Rinsho Yakuri, Jpn J. Clin Pharmacol Ther 30:505-506, 1999. Other Asia-Pacific Experience • Much relaxed/friendly environment; this region’s regulatory agencies have provided: Criteria for bridging evaluation Check for “need a bridging study?” Long list of products that require no verification of ethnic insensitivity • Example: Taiwan, Korea, Singapore, Thailand Considerations for Assessing the Necessity of a Bridging Study ( 1of 4 ) Submit relevant documents Does the drug meet DOH requirements for waiving YES according to DOH a bridging study and also the criteria for exempting requirements and request submission of information for ethnic consideration?(1) for waiving bridging studies NO Does the submitted preclinical and clinical data package meet the regulatory requirements (ICH E5 and DOH guidance on clinical trials)?(2) NO Amendment YES NO Does the package include clinical data of Asian populations?(3) Is the medicine insensitive to both intrinsic and extrinsic factors? efficacy and safety insignificant? (See ICH E5 guidelines) YES YES NO Considerations for Assessing the Necessity of a Bridging Study ( 2 of 4 ) Does the package include clinical data of Asian populations?(3) NO YES YES Have any early phase trials or global clinical trials that meet the YES DOH requirements of bridging studies been conducted in Taiwan? NO Is it reasonable to extrapolate from foreign clinical data that the medicine is insensitive to both intrinsic and extrinsic factors in Asians(3) and that its clinical differences in efficacy and safety are acceptable?(See ICH E5 guidelines) NO Is the medicine insensitive to both intrinsic and extrinsic factors? Are the clinical differences in efficacy and safety insignificant? (See ICH E5 guidelines) No bridging study required(4) NO Based on the result of evaluation, an appropriately designed protocol of a bridging study should be submitted to DOH for approval(5) YES No bridging study required(4) Considerations for Assessing the Necessity of a Bridging Study ( 3 of 4 ) Is it reasonable to extrapolate from foreign clinical data that the medicine is insensitive to both intrinsic and extrinsic factors in Asians(3) and that its clinical differences in efficacy and safety are acceptable?(See ICH E5 guidelines) YES No bridging study required(4) NO Is it reasonable to extrapolate from foreign clinical data that the concentration (dose)-response relationship is similar between foreign and Asian populations(3)? NO Is PK and/or PD data of Asian populations(3) available for estimating dosage or predicting efficacy? YES NO YES Based on the result of evaluation, an appropriately designed protocol of a bridging study should be submitted to DOH for approval.(5) Considerations for Assessing the Necessity of a Bridging Study ( 4 of 4 ) Is PK and/or PD data of Asian populations(3) available for estimating dosage or predicting efficacy? YES NO Based on the result of evaluation, an appropriately designed protocol of a bridging study should be submitted to DOH for approval.(5) Using available data for dose determination (1) Apply for waiving bridging studies with reference to DOH announcements of waiving clinical trials. If the drug falls within the category that “requires submission of information proving no existence of ethnic differences”, it should be evaluated following this flowchart after the one year phase-in period. (2) Under circumstances when evidence indicating potential intrinsic/extrinsic differences between Chinese and other Asian populations, a bridging study in Chinese population is a must. (3) A bridging study will be required when there exists any safety concern. 1(4) Under circumstances when evidence indicating potential intrinsic/extrinsic differences between Chinese and other Asian populations, a bridging study in Chinese population is a must. (5) A bridging study can be a PK and/or PD study or any clinical study that can demonstrate the efficacy and safety of the medicine. Products Requiring No Verification of Ethnic Insensitivity • • • • • • • Drugs for treatment of AIDS Drug for organ transplantation Topical agents Nutrition supplements Cathartics prior to surgery Radiolabeled diagnostic pharmaceuticals The drug is the only choice of treatment for a given severe disease • Drugs for life-threatening disease have demonstrated a breakthrough efficacy • Lacking adequate trial subjects for any drug used for rare disease Products Requiring No Verification of Ethnic Insensitivity • • • • • • • • Anticancer drugs Drugs with breakthrough efficacy Drugs of single use Drugs with different salt of the same composition and the same administered route have been approved internal Drugs for chronic psychologic or immunological diseases and conducting clinical trails internal difficulty Each compounds of new combination drug have been proved internal, and the efficacy is the same as the single compound Drugs with the mechanism, administered route, efficacy and adverse effect, similar to the approved drugs New combination composed of single compound of approved combination or compounds of approved combination has the same efficacy as approved combination US FDA’s Experience O’Neill (2003). The ICH E5 Guidance: An Update on Experiences with its Implementation • Majority of NDA’s contain foreign clinical trial data, often used as primary evidence of efficacy and safety – rarely, does the entire data base on efficacy consist of foreign clinical data • Until recently, discussion have rarely been held with sponsors during IND/NDA development stages that specifically consider bridging strategies when relying on foreign clinical data US FDA’s Expereince • Some, but not all review divisions, during the process of evaluation of the clinical efficacy data examine regional differences in efficacy and safety • Most multi-national trials have included patients from Western Europe, U.S., Canada, New Zealand and Australia – Minimal but increasing experience with Latin America and Eastern Europe • Few examples of formal bridging studies done in the U.S. that were performed subsequent to development of a complete clinical data package, and that were carried out in response to an FDA request US FDA’s Expereince • Generally, when FDA asks for more data/studies, it is because the clinical trial evidence in the NDA is not convincing and other formal phase 3 studies conducted in the U.S. are needed • As trials come from new regions, it may become critical to agree in advance on the sources of data • There has not often been a prospective evaluation during the IND of differential PK, PD or clinical endpoints to treatment response Evaluating “Bridging Evidence” Major Statistical Methods • Shih (2001, CCT) – “Consistency” • Liu, Hsueh and Chen (2002, BJ) – “Equivalence” • Chow, Shao, Hu (2002, JBS) – “Reprodicibility/Generalizability” • Hsiao, Xu, Liu (2003, JBS) – “Group sequential” • Wang/Hung (FDA) (Stat in Med, 2003) “Non-inferiority” • Ware (Harvard) – “Hierarchical model” • Purpose of “Bridging” is not to get an ‘overall’ estimate of treatment effect () by adding another study Consistency Shih (2001). Controlled Clinical Trials, 22, 357-366. • Results of K reference studies (per investigator) from the CCDP are available: W w ,....., w 1 • New (small) local study result from the new region : K v • First, construct the predictive probability function pv W , which provides a measure of the plausibility of v given the results W Consistency • Then compare pv W with the plausibility of each of the actually observed wi , i.e., Pwi W • The result v is considered consistent with the previous results W if and only if Pv W min Pwi W , i 1,..., K (or, a low, say, 5%tile) v falls within the Consistency previous experience of W Bayesian most plausible prediction Reproducibility/Generalizability Chow, S.C., Shao, J., and Hu, O.Y.P. (2002). Journal of Biopharmaceutical Statistics, 12, 385-400. • Statistical Criteria – Reproducibility – Generalizability • Sensitivity Index – A measure, which is derived based on the difference in two patient populations, to determine the chance of reproducibility and generalizability based on the observed clinical data Similarity, Equivalence/Non-inferiority Hung et al. (2003). Statistics in Medicine, 22, 213225. • Let be the therapeutic effect Original region 1 New region 2 • Data (from the original region) available for 1 1 >0 has been established • Want to test hypotheses of 2 Similarity, Equivalence/Non-inferiority • Non-inferiority margin r1 • Hypotheses H 0 : 2 r1 vs. H a : 2 r1 Hung: “Sample size for new trial will usually be demanding”. Global trial: M-national M-center (M-n/M-c) trials • When a ‘m-national m-center’ trial is conducted, likely it is the only study (i.e., no duplication) • US FDA’s practice: When only one “m-center trial” is available for establishing ‘substantial evidence’ of efficacy and safety, the results need to be very persuasive: Overall Rx effect: Highly significant (e.g., p-value <= 0.001) No single site dominates the favorable effect Internally consistent – across centers, endpoints, other subgroups – But …. Leave open how to assess ‘internal consistency’ M-n/M-c trials FDA’s practice • Charles Anello (FDA) ASA FDA-Industry Workshop, Bethesda 2003 Results for individual studies should be presented; Extreme or opposite results need to be discussed; Special attention is given to age, gender and ethnicity (or region) That is, FDA does not seem to differentiate ‘M-n/M-c’ trials from the usual Multi-center trials My View: M-n/M-c vs. M-c trials • In m-center trials, ni in each center is not fixed (although anticipated) and randomization is done within each center • Centers compete with a total N (designed) • When the total N is reached, recruitment stops • Centers with small n are usually combined • Definition of ‘center’ somewhat arbitrary • In a M-n/M-c trial, ‘nation’ is not arbitrary and the sample size given for a nation has to be minimally specified (same as in ‘bridging’) M-n/M-c vs. M-c trials • M-center trials (ICH E-9): Test treatment main effect first; if significant … • Test TxC interaction as an exploratory analysis (no specific method or -level) • When there are a large number of centers, it is less important to consider interaction (since TxC is expected? ) • M-c Focus: the ‘overall’ (main) Rx effect • M-n/M-c focus: nation-specific effect, not the overall Rx effect Overall Rx effect vs. Country specific effect • You never (I bet) saw a drug allowed to be marketed in every state in the U.S. except for California (or vice versa) • But some drugs are approved in the US, but not in Japan; some are approved elsewhere but not in the US • FDA Hung’s “similarity/non-inferiority” for evaluating new region’s 2 is ‘countryspecific’ too) Global drug development: M-n/M-c trials Statistical approach: Hierarchical (multilevel) models • Nations can ‘combine’ their data to improve estimation for each nation/region while allowing for heterogeneity • (Empirical) Bayes methods/REML for multi-level models provide approach to estimation Efron (1996 JASA): Hierarchical (E-) Bayes Model = U Hierarchical (E-) Bayes Model g ( ) is the direct data for 0 (of interest) X is the other countries/centers’ data for U Marginal sampling density: d ( x ) g (u ) f ( x )du Conditional density of given X: h( | x ) h( )d ( x) Induced Prior density for 0: g x ( 0 ) h( | x) g ( 0 )d X0 u Posterior density of 0 based on all the data (X0,X): p x ( 0 | x0 ) g x ( 0 ) f ( x0 ) g x ( 0 ) L0 ( 0 ) 0 Construct hierarchical Bayes interval for 0 Hierarchical (E-) Bayes Model (Morris 1983) E-Bayes tactic: Replace the induced prior with the MLE prior ( ̂ from d ( x ) ) the MLE posterior: pˆ ( 0 | x0 ) gˆ ( 0 ) L0 ( 0 ) The hyper-prior density h(.) is no longer needed Other improvements (e.g., bias correction) also considered in Efron (1996) “Relevance” of X to 0 is a crucial issue May consider ‘mixture/weighted’ prior for g (.) Hierarchical generalized linear models (Lee & Nelder, 1996 JRSS-B) are also worth studying. Simple Model Example Standardized Rx effect: xi ~ N(i , 1); Prior i ~ N(, 2); i = 0, 1, …, K Marginal: xi ~ N(, 2 +1) MLE: ̂ x , ˆ 2 s 2 (only use xi, i =1,...,K) MLE posterior for 0 ~ N( (1 B) x0 Bx , 1-B); K B E-Bayes -level interval for 0 ( K 1) s 2 ((1 B) x0 Bx ) z / 2 (1 B)1/ 2 Efron (1996): Not as good as Stein estimator, which uses x0 in MLE (improvement can be done) Sample size (interval width) depends only on the K other data, 1-B = 12 ( K 1) s Desirable to have large K and small variability in the data X H- (E)-Bayes or H-GLM models are applicable to the bridging study scenario as well … But the the simultaneous multi-level modeling makes more sense when all data (X0, X) are from the same (M-n/M-c) trial. An Example: Summary of Results From a Global Drug Development for Treatment of BPH – 14 national centers Xi ¶Mean (Xi-X)2 and standard deviation of the change in Total Symptom Score in the control (1) and test (2) treatment groups respectively. Hierarchical E-Bayes 95%-level intervals Nation/Center-Specific Rx Effect (Simple Model Example: BPH Data) 5 4 3 2 1 0 1 -1 -2 2 3 4 5 6 7 8 9 10 11 12 13 14 Global Trial: Final remarks As one global trial, all nations’ data are used to improve estimation for each nation while allowing for heterogeneity. There won’t be a ‘global registration’; hence, nation/region-specific Rx effects (assuming properly estimated now) are more of interest than the ‘overall’ Rx effect. Nation/region-specific treatment effects can be contrasted with others, but not in the spirit of showing ‘similarity’ or ‘non-inferiority’. Excess heterogeneity, if happens, still needs to be explained carefully. Summary Scenario (A): When a large US/EU company seeks a drug approval in a small AP nation, use predictive ‘consistency’ to assess fit of the small trial to the larger set of prior experience. Scenario (B): When studies are done elsewhere and submitted for NDA in the US, the FDA will likely ask for repetition studies in the US and assess some kind of ‘similarity’/’non-inferiority’ (not in the ‘active control’ sense). Scenario (C): For global drug trials, simultaneous multi-level models helps to better estimate nationspecific Rx.