Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
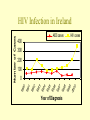
Treatment of HIV DR Sara Woods GUIDE Registrar St James’s Hospital Number of people living with HIV/AIDS Total 33.6 Million Adults 32.4 Million Women 14.8 Million Children < 15 years 1.2 Million AIDS Deaths in 1999 Total 2.6 Million Adults 2.1 Million Women 1.1 Million Children < 15 years 470,000 AIDS cases HIV cases 400 300 200 100 0 19 90 19 91 19 92 19 93 19 94 19 95 19 96 19 97 19 98 19 99 20 00 Number of Cases HIV Infection in Ireland Year of Diagnosis Goal of Antiretroviral Therapy To the length/quality of life by • Reducing the Viral Load (VL) • Preventing infection of new cells • Preventing further damage to the immune system ( CD4) AIM:VL<50 copies/ml and CD4>>200 BHIVA Guidelines When to start therapy? • VL >30,000 & CD4 350-500 • CD4 <350 • Symptomatic Starting Tx early • Drug toxicities • Drug resistance/limit future drug options Delayed Treatment • Limit capacity for immune restoration Antiretroviral Agents (HAART) Divided into 4 groups • Nucleoside reverse transcriptase inhibitors (NRTIs) • Protease Inhibitors (PIs) • Non- nucleoside reverse transcriptase inhibitors (NNRTIs) • Fusion Inhibitors Life Cycle of HIV Inhibited by: Saquinavir, Ritonavir, Indinavir, Nelfinavir, Amprenavir,Lopinavir, BINDING PROTEASE viral proteins TRANSLATION UNCOATING genomic RNA double stranded DNA viral mRNA genomic RNA INTEGRATION REVERSE TRANSCRIPTION Inhibited by: ZDV, ddI, ddC, 3TC, d4T Abacavir, Nevirapine , Delavirdine, Efavirenz TRANSCRIPTION cell nucleus cell membrane ASSEMBLY proviral RNA Antiretroviral Therapy Nucleoside Analogue (NRTI) Non Nucleoside (NNRTI) Protease Inhibitors (PI) Zidovudine(AZT) Nevirapine (NVP) Rtonavir (RTV) Stavudine (d4T) Efavirenz (EFV) Indinavir (IND) Didanosine (ddI) Delaviridine Nelfinavir (NFV) Lamivudine (3TC) Amprenavir (AMP) Zalcitabine (ddC) Saquinavir (SQV) Abacavir (ABC) Lopinavir/Rtn (Kal) Tenofovir (NtRTI) Tipranavir (Tip) Atazanavir (Ataz) NRTIs • 1st drugs licensed • Backbone of HAART • Similar in structure to nuclesides present in HIV RNA • During viral replication – become incorporated into the genome, competing with cellular nucleosides • Bring about chain termination & incomplete replication Zidovudine (AZT) Lamivudine (3TC) • Dose: 300mg -1000mg daily • Metabolism – hepatic and renal • Reduces risk of vertical transmission of HIV • Good CNS penetration • Dose 150mg BD • 90% renal excretion • Hepatitis B Side Effects • Bone Marrow Suppression • Nausea • Headache • Insomnia • Myalgia Side Effects • Pancreatitis • Abnormal LFTs • Peripheral neuropathy • Headache Emtricitabine (FTC) Tenofovir (TEN) • Dose 200mg OD • Take with/without food. • CrCl <50ml/min – dose adjustment • Hepatitis B Side Effects • Headaches, diarrhoea, nausea • CK – muscle pain & weakness • Tg, blood sugar, WCC & RBC • Disturbance of liver, kidney & pancreas • Dose 245mg OD • Take with food • Hepatitis B Side Effects • Hypophosphatemia • Diarrhoea, nausea, vomiting • Pancreatitis • Renal failure, acute renal failure, proximal tubulopathy Protease Inhibitors Act on the HIV Protease Enzyme – prevent production of essential proteins. Benefits: • Dramatic decline in clinical progression of HIV disease/related deaths followed PI introduction in 1996 Drawback: • Pill Burden • Long term metabolic complications Cholesterol/Lipodystrophy Syndrome/Diabetes • Food/fluid restrictions • DRUG INTERACTIONS Ritonavir (RTN) • Dose Escalation 600mg bd • 50% discontinuation rate Side Effects • N/V/D • Perioral/Peripheral Neuropathy • Malaise • Fever Atazanavir Azapeptide PI Superior lipid profile to other PIs Dose: 400mg OD Or 300mg OD Ataz/100mg OD Ritonavir Boosted if coprescribed with Ten or EFV or previous PI exposure With food Side effects Diarrhoea, nausea, vomiting (taken with RTN) Tipranavir • Novel nonpeptidic PI • Active against HIV 1 strains which demonstrate resistance to other PIs • Dose: 500mg Bd Tip/200mg Bd Ritonavir Side Effects • Diarrhoea, nausea, vomiting (taken with RTN) Atazanavir • Azapeptide PI • Superior lipid profile to other PIs • Dose: 400mg OD Or 300mg OD Ataz/100mg OD Ritonavir • Boosted if coprescribed with Ten or EFV or previous PI exposure • With food Side effects • Diarrhoea, nausea, vomiting (taken with RTN) Drug Interactions - PIs • PIs metabolised by CYP 450 isoenzyme system • Coadministration of enzyme inducers may levels of PIs – risk of resistance (eg Rifampicin) • Coadministration of enzyme inhibitors may levels of Pis – risk of toxicity • PIs inhibit CYP3A4 – levels of other drugs RTN>>IND=NFV=AMP>>SQV (eg/Pethidine/Antiepileptics) • Some PIs induce isoenzymes levels of other drugs (eg Methadone/O.C.) NNRTIs • Act on reverse transcriptase enzyme – preventing HIV RNA from being processed • Simplier to take than PIs/no food restrictions • Resistance develops quickly – interclass resistance • ?delayed toxicities Nevirapine (NVP) Efavirenz (EFV) • Dose: 200mg OD x 14/7, then 200mg BD • Metabolised by and inducer of CYP 450 • Dose 600mg OD • Induces and inhibits CYP 450 • Teratogen Side Effects • Rash • Fever • Nausea • Hepatotoxicity Side Effects • Dizziness/Headache • Insomnia • Increased Dreaming • Irritability • Decreased Concentration Drug Interactions NNRTIs • NNRTIs metabolised by CYP 450 isoenzyme system • Coadministration of enzyme inducers may levels of NNRTIs - risk of resistance • Coadministration of enzyme inhibitors may levels of NNRTIs – risk of toxicity • NNRTIs induce isoenzymes levels of other drugs Patient Monitoring • Baseline – VL/CD4/FBC/LFTs • 1 Month – VL/CD4/FBC/LFTs • Then every 3 Months – VL/CD4/FBC/LFTs Virologic Failure • VL > 50copies/ml on 2 occasions more than one month apart Reasons • ? Patient Adherence(<95%)/Intolerance • ? Pharmacological Issues • ? Poor Pharmacokinetics Perform Resistance Test and change therapy accordingly HIV Resistance Reduced Susceptibility of Virus to ART • Virus replicates in the presence of drugs – can result in development of mutations • Results in changes in structure/function of protease & RT enzymes –less susceptible to drugs HIV Resistance Testing • Two types -both require VL > 1000copies/ml Phenotypic Assay: • Measures ability of a HIV isolate from patient to grow in presence of specific drugs • Time consuming & expensive Genotypic Assay: • RT/Protease genes from patients virus sequenced to determine mutations within these genes • Insensitive to presence of minor variants Genital Wart Therapies Clearance Rate Recurrence Rate Podophyllin 38-79% 21-65% Surgical Excision 89-93% 19-22% Electrodesiccation 94% 25% CO2 Laser 72-97% 6-49% Cryotherapy 70-96% 25-39% Interferons 36-53% 21-25% Beutner K, Am J Med, 1997. Patient Applied Therapies Clearance Recurrence rate rate Imiquimod 40-77% Podophyllotoxin 68-88% 5-FU* 68-97% 13% 16-34% 0-8% * No longer recommended Beutner K, Am J Med, 1997. Trichomonas vaginalis • Treatment – • Rx; Metronidazole 2g stat dose • Rx; Metronidazole 400mg bd x 5/7 • Contraindicated in first trimester • Treat Partner Bacterial Vaginosis • Treatment – 120 100 Metronidazole 400mg BD x 5d 80 BV lactobacilli Gardnerella anaerobes 60 40 20 • Avoid alcohol as possibilty of a disulfiramlike reaction normal 0 increasing pH increasing symptoms Treatment of chlamydia • Azithromycin 1g po stat. • Doxycycline 100mg bd x 7/7 • In pregnancy / breastfeeding: 500mg bd x 14/7 Erythromycin • Contact tracing concordance rate 65% of F contacts [80% if epididymitis], 53% M contacts • Test of cure NSU • Treatment – Azithromycin 1g stat dose or Doxycycline 100mgs BD x 7d Alternative regimens Erythromycin 500mgs QDS x 7 days or 250mgs QDS x 14d or Olfloxacin 300mgs BD x 7d Gonorrhoea • IM Ceftriaxone 250mg stat • Screening for other STD • Contact tracing • Pregnancy / Breastfeeding - Ceftriaxone 250mg im stat. • Contact tracing concordance rates: 78% F contacts, 86% M • Test of cure Herpes simplex genitalis • HSV-1 and 2 • Symptomatic primary infection in adult life, as likely to be HSV-1 as HSV-2 • Antivirals Valcyclovir 500mg bd x 5/7- acute attack Valcyclovir 500mg od x 1 year –suppression Acyclovir 200mg five times day - pregnancy • Saline baths/Analgesia/Local anaesthetic/Counselling • May require admission and suprapubic catheterisation • Treatment of syphillis Benzathine penicillin 2.4MU once/week x 3 weeks If allergic - doxycycline 200mg od x 14d or erythromycin 500mg QDS x 14d