Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
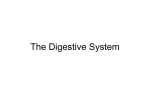
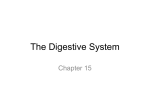
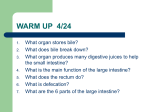
Hepatitis Prevention in Travellers Dr. Pierre J. Plourde Medical Officer of Health Medical Director, Travel Health and Tropical Medicine Winnipeg Regional Health Authority Associate Professor, Departments of Medical Microbiology and Community Health Sciences, University of Manitoba Chair, Committee to Advise on Tropical Medicine and Travel Public Health Agency of Canada What You Don’t Know Can Hurt You Dr. Pierre J. Plourde Medical Officer of Health Medical Director, Travel Health and Tropical Medicine Winnipeg Regional Health Authority Associate Professor, Departments of Medical Microbiology and Community Health Sciences, University of Manitoba Chair, Committee to Advise on Tropical Medicine and Travel Public Health Agency of Canada Hepatitis Prevention in Travellers DISCLOSURE • Honoraria from GSK for presentations on travel health and tropical medicine (Twinrix®) • Honoraria from sanofi pasteur for presentations on travel health and tropical medicine Objectives Prevalence (risk of disease?) Prevention in general (PPM) HBV Exposure Risk Factors Prevention with vaccines Risks of Vaccine-Preventable Diseases • Hepatitis A (1:1000/month) • Hepatitis B (1:2000/month) • Yellow fever (1:4000/week endemic; 1:300/week epidemic) • JE (1:5000/month) • Typhoid (1:30,000/month) • Cholera (1:300,000/month) Immunization Categories • Routine – Childhood/adult immunizations • Recommended – According to specific risks • Required – To cross international borders Algorithm for Travel Immunizations • Childhood immunizations UTD? (Routine) – If no; administer Td, aP, Polio(?), MMR, HBV • Food/water risk? (Recommended) – If yes; HAV, Typhoid, ETEC vaccine(?) • Long-term stay? (Recommended) – If yes; HBV, rabies • Border crossing? (Required) – If yes; Yellow fever, meningococcal Hepatitis Prevention Summary • HAV – Food and water precautions, especially raw shellfish – Vaccine • HBV – Safer sex; avoid skin piercing activities – Vaccine • HCV – Avoid skin piercing activities; ?safer sex • HDV (rare) – Avoid skin piercing activities – HBV vaccine • HEV (relatively rare) – Food and water precautions Hepatitis A Endemicity Geographic Distribution of HAV Infection Hepatitis B Endemicity Geographic Distribution of Chronic HBV Infection HBsAg Prevalence 8% - High 2-7% - Intermediate <2% - Low Hepatitis A Mortality Age-specific Mortality Due to Hepatitis A Age group (years) <5 5-14 15-29 30-49 >49 Total Case-Fatality (per 1000) 3.0 1.6 1.6 3.8 17.5 4.1 Source: Viral Hepatitis Surveillance Program, 1983-1989 Hepatitis B Mortality Hepatitis B – Clinical Features • Incubation period: Average 60-90 days Range 45-180 days • Clinical illness (jaundice): <5 yrs, <10% >5 yrs, 30%-50% • Acute case-fatality rate: 0.5%-1% • Chronic infection: <5 yrs, 30%-90% >5 yrs, 2%-10% • Premature mortality from chronic liver disease: 15%-25% Risk Factors Associated with Reported Hepatitis B, 1990-2000, United States Other* Injection drug use 14% 15% Sexual contact with hepatitis B patient 13% Household contact of hepatitis B patient 2% Men who have sex with men 6% Unknown 32% Blood transfusion 0% Medical Employee 1% Multiple sex partners Hemodialysis 0% 17% *Other: Surgery, dental surgery, acupuncture, tattoo, other percutaneous injury Source: NNDSS/VHSP Hepatitis B • Exposure risks – sex contacts – unexpected/planned health care (blood products, nonsterile equipment, acupuncture) – personal services (tattoo, body piercing, manicures, hair cut/shave) Hepatitis B Exposure Risks* High travel risk** Europeans Americans 95% CI 8.3% (2000) 8% (2004/5) 18-40 yrs 1.9 0.8-4.9 Male 3.4 1.7-7.0 Single 2.4 1.2-5.0 Travel alone 2.0 1.0-4.2 >20 d duration 4.6 1.7-12.6 * Zuckerman JN, et al. J Travel Med 2000;7:170-174; Connor BA, et al. J Travel Med 2006;13:273-280) ** invasive medical intervention, dental, tattoo, body piercing, acupuncture, sex contact Sexual Risk Behaviour of Travellers* • Of ~2000 travellers, 5% reported casual sexual contact with a new partner from the destination country • 52% did not expect this to happen (75% in women) • 31% did not always use condoms • 41% were not protected against hepatitis B * Croughs M, et al. J Travel Med 2008;15:6-12 Fig 2 Number of injections per person and per year and proportion of these administered with injection equipment reused in the absence of sterilisation, by region, 2000 Hutin, Y. J F et al. BMJ 2003;327:1075-1080 Hepatitis B • Exposure risks – sex contacts – unexpected/planned health care (blood products, nonsterile equipment, acupuncture) – personal services (tattoo, body piercing, manicures, hair cut/shave) • Potential benefits – vaccine efficacy >95% after 3 doses – vaccine adverse events minimal – “catch up” universal immunization Hepatitis Vaccine Schedules Hepatitis A Twinrix® Hepatitis B 1440 E.U. 50 Units 160 Ag Units 720 E.U. 20 mcg 10-20 mcg 0, 6-12 mo 0, 1, 6 mo 0, 1, 6 mo 1 mo seroconversion >95% 94% (HAV) 30% (HBV) 30% 80% (0,7,21d) 6 mo seroconversion >95% >95% >95% >20 yrs >20 yrs (HAV) >15 yrs (HBV) >15 yrs Dose Schedule Duration Hepatitis Vaccine Costs • Hepatitis A vaccine – $110 for vaccine – $65 for visit fees • HAV/HBV vaccine (Twinrix®) – $180 for vaccine – $85 for visit fees • Incremental cost of ~$90 Hepatitis Prevention in Travellers Conclusions • Pre-travel risk assessment for HAV and HBV in all travellers • Food and water precautions, safer sex, avoidance of skin piercing activities • All non-immune travellers should receive HAV and HBV vaccines – Vaccines are very efficacious and safe • Immune globulin (Ig) rarely indicated • Stay tuned for CATMAT Statement Hepatitis Prevention in Travellers MERCI THANK YOU