Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
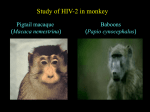
Epidemiology of HIV-2 infection in the U.S, 1996-2006 Lata Kumar MS, MPH Richard Selik MD Division of HIV/AIDS Prevention National Center for HIV/AIDS, Viral Hepatitis, STD and TB Prevention Centers for Disease Control and Prevention 2007 HIV Diagnostics Conference, Dec 5-7, 2007 The findings and conclusions in this presentation are those of the authors and do not necessarily represent the views of the Centers for Disease Control and Prevention. Outline • Background • Methods – Diagnostic criteria • Results • Discussion • Conclusion • Recommendation Background Background – HIV-2 first isolated 1986 – West Africa – HIV-1 and HIV-2 - 60-70% homologous HIV Groups and Subtypes HIV HIV-1 Group O Group N HIV-2 Group M * Subtypes A - K Subtypes A-G *HIV-1, subtype B most common in U.S. HIV-2 Prevalence Highest in West Africa Ivory Coast Guinea Bissau The Gambia Guinea Senegal Other Countries Reporting HIV-2 Infections < 1% HIV-2 HIV-2 – Transmission Same modes of transmission as HIV-1 * ‘ Male-to-male sexual contact (MSM) Injection drug use (IDU) Both MSM and IDU (MSM/IDU) High-risk heterosexual contact* (HRH) Other ' Heterosexual contact with a person known to have or to be at high risk for HIV infection Includes persons that acquired HIV due to hemophilia or a blood transfusion and person whose risk factor was not reported or identified HIV-2 – Clinical Aspects - Less transmissible - Progresses more slowly to AIDS - Lower mortality Source Marlink R., “Lessons learned from the second AIDS Virus, HIV-2”, AIDS 10: 689-699. 1996 HIV-2 – Risk Factors • Native of West Africa • Sexual contact or needle sharing with - a person from this endemic region - a person with known HIV-2 infection • Children of women with or at-risk for HIV-2 Methods HIV-2 – Surveillance Methods Laboratory component: Identify and confirm infections Interview component: Determine exposures, risk factors, and country of origin Data Source CDC maintains supplemental database for reports on HIV-2 infection to ensure completeness of reporting Diagnostic Criteria Figure 1. Centers for Disease Control/Food and Drug Administration testing algorithm for use with combination HIV-1/HIV-2* enzyme immunoassays(EIAs) HIV-1/HIV-2 EIA HIV-1 Western Blot Positive @ Indeterminate Negative Report as HIV positive ^ HIV-2 EIA Repeatedly Reactive HIV-2 Supplemental Test ( e.g., Western blot) Positive Negative Indeterminate * HIV- human immunodeficiency virus @ An Immunofluoresence assay (IFA) for HIV-1 antibodies has recently been licensed by the Food and Drug Administration and can be used instead of Western blot. Positive and negative IFA results should be interpreted in the same manner as similar results from Western blot tests. An indeterminate IFA should first be tested by Western blot and then as indicated by the Western blot results. ^ Perform HIV-2 EIA only if there is an identified risk factor for HIV-2 infection HIV-2 – Laboratory Diagnosis 1. Screening HIV-1/2 ( EIA) 2. Perform HIV-1 Western Blot - Rule out HIV-1 first * 3. Bio-Rad HIV-1/ HIV-2 Multispot 4. Detect/Confirm HIV-2 antibodies - HIV-2 Western blot - PCR for unique sequences * HIV-2 not FDA licensed antibodies can react with bands on HIV-1 Results Distribution of HIV-2 cases in the U.S by Country of Birth, 1996-2006 (N=68) Other Countries 2% India India 12% 12% Other Africa 7% East EastAfrica Africa 11%11% West Africa West Africa 66% 66% Distribution of HIV-2 cases among the different regions in the U.S, 1996-2006 US region Number of cases Midwest 26 (38%) South 12 (18%) Northeast 12 (18%) West 8 (12%) Total 68 Disease category of HIV-2 cases at diagnosis, United States, 1996-2006 Among the 68 reported – 19 cases had AIDS – 29 cases did not have AIDS – 20 cases did not have sufficient information to know status Distribution of HIV-2 cases by Race/Ethnicity, United States, 1996-2006 Race/Ethnicity Number of cases Blacks 53 (77%) Asian /Pacific Islanders Other/unknown 8 (12%) 7 ( 10%) Total 68 Discussion Discussion • HIV-2 infection continues to be of low prevalence in the U.S • Majority of the cases reported are from persons of West African origin • Diagnosis of HIV-2 continues to be a challenge – absence of FDA approved confirmatory test Limitation • Incomplete reporting since not all states have reported HIV-2 consistently to CDC? • The total cases here may be an under estimation of the true cases Conclusion • Although HIV-2 continues to be of low prevalence in the US, monitoring the type of HIV infection needs to continue in the U.S – Since antiretroviral treatment (ARV) is different for HIV-2 infection – Misdiagnosis of HIV-2 to be HIV-1 due to crossreactivity Recommendation When HIV-2 is suspected, the following steps should be followed : • Send specimens to CDC laboratory for confirmation • Contact CDC coordinator for “Cases of Public Health Importance” (COPHI) Questions ? Lata Kumar [email protected] Tel: 404-639-3893