Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Food choice wikipedia , lookup
Low-carbohydrate diet wikipedia , lookup
Epidemiology of metabolic syndrome wikipedia , lookup
Overeaters Anonymous wikipedia , lookup
Thrifty gene hypothesis wikipedia , lookup
Gastric bypass surgery wikipedia , lookup
Cigarette smoking for weight loss wikipedia , lookup
Abdominal obesity wikipedia , lookup
Obesity and the environment wikipedia , lookup
Childhood obesity wikipedia , lookup
Obesity in the Middle East and North Africa wikipedia , lookup
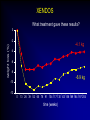
Cumulative incidence of Diabetes after 50 years based on average BMI aged 20-50 years Johns Hopkins precursors study - n=916 males Cumulative incidence (%) 15 >25 24-24.9 22-23.9 <22 12 9 6 3 0 50 55 60 65 70 75 age (years) Arch Intern Med 1999;159:957-63 TV watching and activity as risk factors for DM in 37519 health professionals Arch Intern Med 2001;161:1542-8 What can we do about obesity ? Julian H Barth Obesity Clinic, Leeds, UK. What is obesity ? The disease process of obesity is weight gain not the absolute value of overweight The average man gains 1 gm per day A toxic or obesogenic environment Obesity as a normal response to an abnormal environment • side-effect of technological advances • reflects natural human preferences (eg easy, convenient, fast, low effort, value for money) • key vectors – energy-saving machines, passive recreation – energy-dense foods & drinks, large portion sizes Natural history of obesity Obese Overweight Normal Years of management or intermittent monitoring How do we treat obese patients? • identify ideal weight • prescribe 800-1000 kCal diet • castigate the patient as a failure • await the development of co-morbidities Treatments for obesity • Diet / eating patterns • Physical activity • Psychological / behaviour modification therapy • Pharmacotherapy • Surgery • Prevention Evaluation of the obese patient • Examine the patient for co-morbidities • Examine the patient for a “medical” cause of obesity • Ask why the patient wants to lose weight • Ask how much weight loss is desired What are the causes of obesity? Nutritional ignorance Sedentary lifestyle Drug therapy for other diseases Dysfunctional eating Social/emotional turmoil Chronic failure of life-long dieting Successful obesity management • patient accepts the benefit of weight loss • patient accepts modality of therapy • competent, sympathetic health-carer available to review progress regularly • realistic claims for weight loss • indefinite after-weight-loss service BNF 1999 Eating & obesity • • • • • • • • Eating patterns Nutritional knowledge Missed meals Social eating Binge eating Emotional eating Alcohol ex-sports-(wo)men Dietary therapy • Low calorie diets – – – – – LCD (800-1500kCal/day) (3.4-6.3MJ) High fibre diets calorie counting energy prescribed low CBH diets • VLCD (<800kCal/day) (<3.4MJ) • Milk diet • Alternative diets XENDOS What treatment gave these results? 0 weight loss (%) -2 -4.1 kg -4 -6 -8 -6.9 kg -10 -12 0 13 26 39 52 65 78 91 104 117 130 143 156 169 184 197 204 time (weeks) Physical activity and obesity • 4th risk factor for IHD – as important as cholesterol and bp • PA improves cardiovascular fitness, plasma lipids & blood pressure • physically active subjects live longer • exercise results in more weight loss than diet • Doctors do NOT advise their patients to be active Before starting drug therapy… • Previous therapies – dietary approaches – Physical activity – Behavioural modification • Motivation • Effective • Safe • lifestyle changes have the potential for longterm weight loss Drugs that promote weight gain • steroids • beta-blockers • anti-diabetic agents • anti-histamines • anti-psychotic agents • anti-depressants • anti-convulsants • anti-migraine agents • breast cancer therapies Medical therapy for diabetes Sulphonylurea + Insulin Insulin Diet alone UKPDS 57 Diabetes Care 2002;25:330-6 Indications for drug therapy • Obesity of severity to shorten life span • Obesity related disorders that might be improved by weight loss – eg hypertension, NIDDM, hyperlipidaemia & sleep apnoea • Need to reduce weight for other medical therapy eg surgery Timing of drug therapy • Good motivation – weight loss already achieved with diet &/or physical activity – newly diagnosed obese subject with diabetes or bp • Poor motivation • Weight loss usually occurs within the first 4-6 months of programme • Realistic expectations of therapy Pharmacotherapy for obesity (2001) • • • • • Phentermine Mazindol Diethylproprion Fenfluramine Dexfenfluramine all have been withdrawn • Orlistat • Sibutramine • Rimonabant ‘Xenical’ ‘Reductil’ ‘Accomplia’ Aims of obesity therapy • Weight loss • Weight maintenance Orlistat: mean weight changes 0 –2 Change –4 in body weight –6 (%) Placebo (n=249) –6.1% *p<0.001 –8 Orlistat 120 mg (n=271) –10 –10.2% –12 -4 0 10 20 30 40 52 Time (weeks) Sjostrom L et al. Lancet 1998;352:167 XENDOS • 4 years therapy with orlistat • Weight loss – Active Rx – Placebo 6.9 kg loss 4.1 kg loss • Cumulative incidence of type 2 Diabetes – Active Rx – Placebo 6.2% 9.0% Weight maintenance: sibutramine Weight loss Weight maintenance Bodyweight (kg) 104 102 100 Control 98 96 94 Sibutramine 92 90 88 0 2 4 6 8 10 12 14 16 18 20 22 24 Month STORM Study. Lancet 2000;356:2119-25 Combination of lifestyle modification & sibutramine on weight loss Sibutramine alone Sibutramine + Lifestyle Combined Treatment 20 18 16 14 12 10 8 6 4 2 0 2 4 6 Time (months) 12 Arch Intern Med 2001;161:218-227 Rimonabant Van Gaal LF et al. Lancet 2005;365:1389-1397. Counterweight • 7 UK centres • Weight management advisors at each centre • Obesity audit of disease burden • Prospective obesity management programme through practise education Weight loss 0 start 3 months 6 months 12 months -1 -2 kg -3 * -4 * * -5 -6 * p<0.001(n=446) Completers Non-completers Int J Obes 2004;28 (suppl 1):S29 Slimming on Referral • Collaborative project between Derby HA & Slimming World • Pilot study • 107 subjects 70 60 50 40 12w 24w 30 • 58% competed 12w 20 • 27% completed 24w 10 0 <5% 5-10% >10% Obesity surgery • 1-2% morbidly obese ~ 8-16,000 people in Leeds • Considerable weight loss maintained over 8-10 years • Considerable reduction in comorbidities – – – – Diabetes Musculoskeletal disorders Sleep apnoea Improved quality of life • Only about 200 operations p.a. in England & Wales …so what are the indications for surgery? NEJM 2004;351:2683-93 What do we need ? Slimming clubs Support groups Occupational health Primary care team GP, nurse, dietitian, psychologist Secondary care team Dietitian, physician, surgeon Obesity research unit Sports & leisure facilities Disinterested Primary care team HEALTHY ENVIRONMENT