Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
EMS “Street Drug” Review and
Management of Overdose
S I LV E R C R O S S E M S S Y S T E M
JA N UA RY 2 0 1 4
Objectives
Review of the commonly used “street drugs”
How to identify a patient that is possibly on these drugs
Common side effects of these drugs
EMS management of safety considerations
Overdose situations: management and clinical assessment decision-making
SMO: overdose review
Medication review: Narcan
Skill review: insertion of the oropharyngeal and nasopharyngeal airways
Methamphetamine
Common
“Street Drugs”
that EMS is
increasingly
facing
Common Club Drugs:
◦ MDMA (Methylenedioxymethamphetamine)
◦ GHB (Gamma-hydroxybutyric acid)
Heroin
Methamphetamine
Other names for
methamphetamine:
◦ Ice
◦ Meth
◦ Tina
◦ Geep
◦ Chalk Dust
◦ Ice Cream
◦ LA Glass
Methamphetamine
Methamphetamine is a highly addictive
stimulant.
Generally lasting 12 hours, this high is 250 times
more stimulating to the dopamine receptors in
the brain than the high from endorphins from
exercise, eating, and even sex.
These receptors wear out after a period of time,
becoming damaged. The person has no way to
feel good from eating, sex, or anything
pleasurable and seeks out more of the drug.
These people may go into a deep sleep for two
to four days, appearing to be deceased.
This puts them at risk for rhabdomyolosis, a
break down of muscle tissue. The proteins
floating in the bloodstream from this
breakdown clog the kidneys and cause kidney
failure. Depending on the extent of the
damage, the patient could end up on
permanent dialysis.
Swallowing
-20-30 Minutes to feel the effects
How is Meth
ingested?
-This method has the least risks due to the vomiting
mechanism when toxins are ingested
-Meth can be put in water, juice, and commonly is
placed in gel caps and taken orally.
-“Parachuting” is wrapping the meth in toilet paper
and swallowing it. This delays the onset, and makes
the high come on more slowly and evenly. This can
also be done with a baggie and a small puncture.
Considered a “harm reduction technique.”
Crystal Meth Recovery Services,
Meth Memo 2013
Smoking
7-10 Seconds to feel the effects
How is Meth
Ingested?
Crystal Meth Recovery Services,
Meth Memo 2013
Entered through the lungs which may lead to
breathing difficulties
Usually crystal meth is smoked in glass pipes, similar
to how crack cocaine is used.
Shooting Up
15-30 seconds to feel the effects
How is Meth
Ingested?
Injected into the veins, or “the works.”
This is where abscesses and skin infections begin to
develop.
Injection bypasses the filtering mechanism by the body:
the vomiting mechanism is bypassed and this directly
circulates in the bloodstream.
The sharing of needles spreads diseases such as
Hepatitis, HIV, and many antibiotic-resistant bacteria.
Crystal Meth Recovery Services,
Meth Memo 2013
Improperly drawn-up meth can create an air bubble in
the syringe and subsequently cause an air embolus
resulting in cardiac arrest.
“Bumping” or snorting
Onset of 3-5 minutes
How is Meth
Ingested?
Crystal Meth Recovery Services,
Meth Memo 2013
Most common ingestion method
Can cause nose bleeds, respiratory problems,
and abscesses can form on the nose and face.
“Booty Bump”
How is meth
ingested?
Onset of 10-15 seconds
Needleless syringe is used to administer liquid meth into the
rectum.
The drug is absorbed by the blood vessels in the lining of the
rectum.
Sometimes used in conjunction with prostitution, this can
cause injury and disease when used as a “professional
adjunct” for these patients for alternate routes of intercourse.
Often used in patients who have septum issues from snorting
or loss of veins from injecting.
Crystal Meth Recovery Services,
Meth Memo 2013
“Hot Rail”
Onset of 7-10 seconds.
How is Meth
Ingested?
Crystal Meth Recovery Services,
Meth Memo 2013
A glass stem is heated until the tip is red hot, then
placed over a bump (a small pile of the drug) and
the vapor is inhaled through the nose.
Immediate Effects
Elation
Effects of Meth…
High energy and feeling of acuity, insomnia
GI distress (vomiting/ diarrhea)
Sweating
Anorexia
Agitation, irritability, talkativeness, panic, compulsive
fascination with repetitive tasks, violence, confusion
Increased sex drive, making this a popular club drug
Hypertension, hyperthermia, tachycardia, glucose level
instability, bronchodilation
Vasoconstriction
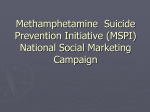
“Faces of Meth”
Faces of Meth is an internet finding with
hundreds of results.
Meth causes muscle wasting and anorexia,
and in combination with the toxins it is “cut”
with, causes a severe result in the aging
process and is often the cause of sores on the
face and skin. Tooth loss is also a common
side effect of meth use…
Here are some “before and after” photos.
Most of these photos are taken within a sixmonth to two-year period:
“Faces of Meth”
http://photos.oregonlive.com/oregoni
an/2011/05/faces_of_meth_7.html
“Faces of Meth”
http://photos.oregonlive.com/oregoni
an/2011/05/faces_of_meth_7.html
“Faces of Meth”
http://photos.oregonlive.com/oregoni
an/2011/05/faces_of_meth_7.html
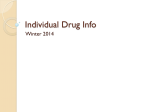
Meth and the
teeth…
Meth affects the
top teeth first, and
subsequent damage
spreads to the gum
tissue, dissolving
the roots.
Treating the patient experiencing
agitation and insomnia…
EMS and Meth…
Be aware the lack of sleep causes the brain to work incorrectly.
When combined with the toxins of meth, this patient can
become very agitated.
Use caution and protect yourself from exposure to bodily fluids
from an agitated patient and paraphernalia in the pockets.
EMS and meth
Ask for police assistance when dealing with a violent patient,
however, make an attempt at calming these patients. The
tachycardia and hypertension in combination with further
agitation can cause cardiac arrest.
Use restraint techniques safely. Use of soft restraints is
preferred over police handcuffs to reduce injury and
professional liability.
Call ahead for medical control direction for the agitated patient
if necessary.
Obtain IV access if possible.
EMS and meth
Maintain airway control, being aware of loose teeth,
piercings, and vomit that potentially could enter the
airway.
If patient is seizing, follow Code 35 for the ALS/BLS
SMO’s for Seizures. ALS providers can administer
Versed if applicable.
Monitor patient for hypertension, hyperthermia,
and cardiac arrhythmias. Be sure to monitor
patient’s glucose level
Myocardial infarction
Meth Overdose
“The approach to the patient with
methamphetamine-induced cardiac ischemia should
be no different than standard of care ACS
treatment. Nitrates, beta-blockers, aspirin, heparin,
and morphine should be administered if indicated.
Based on the latest American College of Cardiology
Foundation/American Heart Association guidelines,
methamphetamine- and cocaine-using patients with
chest pain and suspected ACS should also receive
sublingual nitroglycerin.”
Methamphetamine Toxicity Treatment
& Management (2013). John R
Richards, MD, FAAEM; Chief
Editor: Asim Tarabar, MD.
MDMA
9 million users worldwide
Most common club drug
Often seen at raves and industry parties
MDMA
STREET NAMES
ECSTASY
Elephants
Adam
Eve
Scooby snacks
Cadillac
Hug
Snowball
Beans
Hug Drug
X
California Sunrise
Love Drug
XE
Clarity
Love pill
XTC
E
Lover’s speed
Essence
Molly
Roll
“Ecstasy
MDMA
was originally developed by Merck
pharmaceutical company in 1912. In its original
form, it was known as “MDMA.” It was used in
1953 by the US Army in psychological warfare
tests, and then resurfaced in the 1960s as a
psychotherapy medication to “lower
inhibitions.” It wasn’t until the 1970s that
MDMA started being used as a party drug.
By the early 1980s, MDMA was being promoted
as “the hottest thing in the continuing search
for happiness through chemistry,” and the “in
drug” for many weekend parties. Still legal in
1984, MDMA was being sold under the brand
name “Ecstasy,” but by 1985, the drug had been
banned due to safety concerns.”
Drugfreeworld.com (2013)
Onset form pill ingestion is roughly 20 minutes to
one hour.
Duration is anywhere from 3 to 6 hours.
MDMA
Patient has feeling of well-being, extreme euphoria,
significantly enhanced sense of touch and other
senses such as sound perception, along with a
boost in energy. Some individuals even experience
mild hallucinogenic effects while on the drug. The
enhanced tactile experiences individuals
experience while on the drug has earned it the
nickname "the love drug".
Some Ecstasy users feel ill and experience stiff
joints and muscles, a stiff jaw, extreme thirst, sleep
disturbances, depression and paranoia.
www.ecstasy.ws/e-overdose.htm
(2014)
Actual overdose is rare, and what EMS needs to
consider is the effects of the drug
MDMA and EMS
Hyperthermia and low sodium levels (hyponatremia)
are the biggest problems EMS faces. Monitoring
patient’s temperature and glucose levels are
mandatory. Establishing an IV of NS will help restore
sodium and prevent further dehydration.
Take caution when touching patients, as they have
increased tactile sensations.
Actual overdose is treated following SMO protocol
for overdose, maintaining airway and following ACLS
guidelines for cardiac arrhythmias.
Rohypnol
GHB
It has been a concern for the last few years because
of its abuse as a "date rape" drug.
People may unknowingly be given the drug that,
when mixed with alcohol, can incapacitate victims
and prevent them from resisting sexual assault.
Also, Rohypnol can be lethal when mixed with
alcohol and/or other depressants.
https://www.kstate.edu/media/webzine/Didyouhearyes/GHBfacts.html
This drug is a sedative-hypnotic, causing amnesia.
It can cause respiratory depression in large
amounts.
GHB is usually taken orally.
GHB
It is sold as a light-colored powder that easily
dissolves in liquids or as a pure liquid packaged in
vials or small bottles.
In liquid form, it is clear, odorless, tasteless, and
almost undetectable when mixed in a drink. GHB is
typically consumed by the capful or teaspoonful at a
cost of $5 to $10 per dose.
https://www.kstate.edu/media/webzine/Didyouhearyes/GHBfacts.html
The average dose is 1 to 5 grams and takes effect in
15 to 30 minutes, depending on the dosage and
purity of the drug. Its effects last from three to six
hours.
The most likely situation with this drug arises in an
unintentional ingestion.
GHB and EMS
Be careful to preserve evidence if patient feels they
were sexually assaulted.
Take caution with patient’s emotions, as they may
be fragile due to amnesia and experience severe
anxiety.
Treatment of the side effects is necessary, and due
to “cocktail mixes” Narcan may be given to
counteract other drugs mixed with GHB.
Side effects of mild to severe overdose:
Nausea
Vomiting
Delusions
Depression
GHB Overdose
Vertigo
Hallucinations
Seizures
Respiratory distress
Loss of consciousness
Slowed heart rate
Lowered blood pressure
Amnesia
Coma
GHB can become addictive with sustained use.
Heroin
Heroin use is on the rise!
Has a “city drug” stigma, however many suburban
departments are seeing huge increases of the drug in
higher socioeconomic areas
30 Deaths are accounted to heroin in Will County in 2011
Chicago and the metro surrounding areas have the highest
rate of ER visits due to heroin abuse
While many EMS providers are familiar with
overdoses and the heroin patient, important
reminders of care can make for a better patient
outcome and safer situations for EMS
Heroin and EMS
Many reports of EMS providers having a problem
with a patient requesting a refusal after Narcan is
administered. Call medical control for direction!
Symptoms
Airways and lungs
Heroin Overdose
◦ Apneic
◦ Shallow breathing
◦ Slow and labored breathing
Eyes, ears, nose, and throat
◦ Dry mouth
◦ Extremely small pupils,
sometimes as small as the
head of a pin ("pinpoint
pupils")
◦ Tongue discoloration
Cardiac
◦ Hypotension
◦ Weak pulse
◦ Bradycardia
Skin
◦ Cyanosis
◦ Notable track marks/difficulty
establishing an IV
Stomach and intestines
◦ Constipation
◦ Spasms of the stomach and
intestinal tract
Nervous system
◦
◦
◦
◦
◦
Coma
Delirium
Disorientation
Drowsiness
Muscle spasticity
INITIAL MEDICAL CARE/
OBTAIN BLOOD GLUCOSE READING
*AIRWAY-BREATHING-CIRCULATION-CARDIAC
MONITOR
SUSPECTED SYNTHETIC NARCOTIC OVERDOSE AND
RESPIRATORY RATE <12
SMO Review:
Code 33
Drug Overdose
CONSIDER NARCAN 2 MG INTRANASALLY (ALS or
BLS) one mg per nostril, IF AVAILABLE -OR-
(ALS) 2MG NARCAN IV/IM
CONSIDER RESTRAINTS PRIOR TO
ADMINISTRATION
TRANSPORT
Drug of the
Month
Narcan
(naloxone)
Opioid antagonist
Counters the effects of opiate overdoses:
◦ Heroin
◦ Morphine
◦ Vicodin
◦ Codeine
◦ Oxycodone
◦ Fentanyl
◦ Methadone
May be administered intranasally (ALS or BLS)
IV, IM, and IO (with medical direction) are all ALS
administration routes for Narcan
Narcan
(naloxone)
Given in 2mg increments every five minutes, up to 6mg
Opioid withdrawal syndrome may occur in some patients
given large doses of Narcan.
Severe side effects of Narcan:
Emesis and aspiration, agitation, hypo- and hypertension,
cardiac arrhythmias, dyspnea, pulmonary edema,
encephalopathy, seizures, coma, and death.
Narcan reduces constipation, and in repeat doses can cause
explosive diarrhea.
Nasopharyngeal airway skill review:
Skill review:
Nasopharyngeal
airway
Your EMT textbook might have explained that the
proper way to measure is from the tip of the nose
to the ear lobe. True.
But you can grab the right size on the first try most
of the time with this rule:
Big adults – grab the 8-9mm (24-27 french).
Regular sized adults get a 7-8mm (21-24 french).
Small adults get a 6-7mm (18-21 french).
Kids start at 5mm and work down.
Taken from: theemtspot.com (2014)
When deciding if a patient is “big” or “regular” use
their height as a guide, not their weight. Patient
height is the most accurate predictor of correct NPA
sizing.
Indicated in cases of respiratory depression/arrest and:
◦ Intact gag reflex
◦ No signs of facial trauma
◦ Signs of drug overdose
Considerations for
nasopharyngeal
airway insertion
◦ Do not force NPA into the nostril as this may cause unnecessary
edema and trauma.
◦ Use NRB or AMBU to assist patient with adequate oxygenation
and ventilation.
◦ Choose larger nostril
◦ Lubricate to reduce trauma to soft tissues
Nasopharyngeal
Airway Insertion
http://www.atitesting.com/ati_next_gen/skillsmodules/co
ntent/airway-management/equipment/devices.html
Prevents the tongue from occluding/covering the
epiglottis
Skill Review:
Oropharyngeal
Airway
Indicated in the patient with:
◦ No gag reflex
◦ Excessive secretions and frequent suctioning is
needed
◦ Larger tongue/tongue occluding the airway
Skill review:
Oropharyngeal
Airway Insertion
http://www.atitesting.com/ati_next_gen/skillsmodules/content
/airway-management/equipment/devices.html
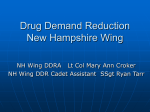
TITLE:
LVAD PROTOCOL
POLICY:
This policy is to be used for patients with Left Ventricular Assist Devices.
Adopted from Thoratec Corporation for HeartMate II LVAD Training for Hospitals and EMS
Always attempt to:
-Contact implanting center
-Keep patient’s companion
with the patient
Patient Calls 9-1-1
System Policy
Update:
LVAD Protocol
Manual Page
300-78
LVAD Functioning?
Auscultate left upper quadrant.
Continuous hum = pump running
Green arrows = pump running
Attention: Patient may not have palpable pulse
or measurable BP even if the pump is working
YES
Patient Stable
NO
Patient Unstable
Pump connected to controller?
Pump connected to power?
Assess for other general
medical problem
Treat per
medical protocol
Treat per standard
protocol
Place an EKG
monitor
Treat per ACLS
protocol
Transport Urgently to ED
If possible, transport to implant center
Controller
Alarming
Treat for cardiogenic shock.
Change controller
if instructed
Thank you for your time and
attention!
Silver Cross EMS System
January 2014