Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
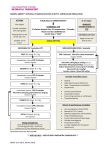
ROC ALPS Amiodarone, Lidocaine, or Placebo Study Version 24: Rev. 2012-4-24 RESUSCITATION OUTCOMES CONSORTIUM Learning Objectives • Understand the rationale for antiarrhythmic use in out-of-hospital cardiac arrest • Understand how to carry out the ROC ALPS study protocol NOTE: IN ALPS, unless otherwise noted, the abbreviation “VF/VT” refers to ventricular fibrillation or pulseless ventricular tachycardia. 2012-4-24 v24 Reason for the Study • About 24% of cardiac arrests are due to VF/VT • 70% will re-fibrillate after the first shock • Antiarrhythmic drugs (good or bad?): Unlikely to chemically convert patients out of VF/VT May increase probability of shock success May prevent VT/VF recurrence after defibrillation May result in higher incidence of bradycardia/asystole May improve, not change, or worsen patient outcome • Current options: Lidocaine Amiodarone 2012-4-24 v24 Prior Amiodarone Studies • Seattle/King County medics (ARREST) Amiodarone vs. placebo Amiodarone improved admission alive to hospital→ NSD* in survival to discharge • Toronto medics (ALIVE) Amiodarone vs. lidocaine Amiodarone improved admission alive to hospital→ NSD* in survival to discharge • Oslo medics IV/drugs vs. no IV IV/drugs improved admission alive to hospital → NSD* in survival to discharge • All trials underpowered to address survival *No significant difference 2012-4-24 v24 New Formulation of Amiodarone • Amiodarone previously diluted in Polysorbate 80 (“Tween”) as Cordarone® & now generic formulations Caused hypotension Foaming issues Adherent to plastic—requires all-glass packaging • New formulation: Nexterone® (PM101) Amiodarone diluted in Captisol Does not cause hypotension Safe for bolus administration Plastic-friendly—allows for prefilled non-glass syringes in future Currently FDA-approved only in glass syringe 2012-4-24 v24 Benefit of Antiarrhythmics Unclear • American Heart Association 2010 ACLS Guidelines Amiodarone or lidocaine (each is a class IIb weak “may be considered” recommendation for shock-refractory VF/VT) • Amiodarone and lidocaine may have other adverse effects • Neither drug ever proven to improve survival • Unproven therapies may be . . . Beneficial Inconsequential (make no difference) Harmful • The only way to know if lidocaine or amiodarone “work” is to compare either against neither (placebo) 2012-4-24 v24 Trial Design Population Persistent or recurrent VF/VT* after >1 shock Vascular Access Intervention Amiodarone Outcome * In RANDOMIZE Lidocaine Neither (saline placebo) SURVIVAL TO HOSPITAL DISCHARGE ALPS, ‘VF/VT’ refers to ventricular fibrillation or pulseless ventricular tachycardia 2012-4-24 v24 Inclusion Criteria YES: • Non-traumatic out-of-hospital cardiac arrest • Vascular access (IV or IO) • Persistent/recurrent VF/VT after 1 (or more) shocks… (“it’s baaack!”) NO: • Open label IV amiodarone or lidocaine use in-field1 • Known hypersensitivity or allergy to amiodarone or lidocaine • Protected population (prisoners, children2, pregnancy, etc.) 1This also excludes use of IO lidocaine to minimize pain when inserting/flushing IO line 2Under 2012-4-24 v24 local age of consent Inclusion continued… • What counts as a “shock”? ROC-EMS agency administered shock(s) » First responder or BLS-AED delivered a shock » ALS delivered a shock PAD and non-ROC agency shock(s) Not ICD shock(s) 2012-4-24 v24 Inclusion continued… It’s baaack! • What is persistent/recurrent VF/VT? Confirmed VF/pulseless VT (operationally, pulseless means needing CPR) seen anytime after first shock » VF/VT seen (see-through CPR in systems that “look” at the rhythm after a shock before drug treatment ) after ≥1 shock » VF/VT seen on second or later rhythm analysis (in systems that perform a formal rhythm analysis before each shock or drug intervention, or those who give drugs “blindly” (during CPR) following a shock) after ≥1 shock If thinking antiarrhythmic drug for VF/pulseless VT… give ALPS drug 2012-4-24 v24 Drug Kit Design Three (3) identical (blinded) syringes SYRINGE # AMIODARONE KIT LIDOCAINE KIT PLACEBO KIT 1A Amiodarone 150 mg (3 cc) Lidocaine 60 mg (3 cc) Placebo (3 cc) 1B Amiodarone 150 mg (3 cc) Lidocaine 60 mg (3 cc) Placebo (3 cc) 2 Amiodarone 150 mg (3 cc) Lidocaine 60 mg (3 cc) Placebo (3 cc) 2012-4-24 v24 Drug Kit Design continued… Length: 7.75 in. 2012-4-24 v24 Width: 4.5 in. Height: 1.75 in. ClearLink Adapter Kits are packaged with a Baxter CLEARLINK Adapter Adapter must be used to ensure compatibility with all IV infusion sets 2012-4-24 v24 ClearLink Adapter View supplemental ALPS training video, “Mandatory use of CLEARLINK Adapters with ALPS Syringes” dated 2012-4-19 Six minute video reviewing background for CLEARLINK requirement, method of use, and reporting potential adverse events Posted on ROC-web: https://roc.uwctc.org/tiki/alps-training-materials Available for download: Windows Media or QuickTime formats 2012-4-24 v24 Study Protocol • Cardiac Arrest—VF/pulseless VT • After Shock #1 (or more) NSR/ROSC/Asystole/PEA?→ Move on Still in VF/ VT?→ Give Syringes #1A and #1B • After Subsequent shock(s) NSR/ROSC/Asystole/PEA?→ Move on Still in VF/ VT?→ Give Syringe #2 • Move on 2012-4-24 v24 What if VF/VT Returns? • “It’s baaaack…” Carry out the full ALPS Protocol • What if I gave Syringes #1A and #1B, got pulses (ROSC) back, but VF/pulseless VT later returns? Shock again If this shock fails to stop VF/VT, give Syringe #2 2012-4-24 v24 What about late-occurring VF/VT? • VF/pulseless VT is treated the same way anytime it recurs after 1 or more prior shocks. This applies to: VF/VT on EMS arrival VF/VT arrest after EMS arrival Late-occurring VF/VT • Anytime VF/pulseless VT returns after 1 or more prior shocks (“it’s baaack”)→ give ALPS drug ASAP 2012-4-24 v24 A) My EMS agency does not “stop to look” after giving a shock VF/pulseless VT seen on second or later rhythm analysis after ≥1 shock… • Shock→ immediate CPR (without look) • Give study drug during 2-minute period of CPR after shock, in the belief that VF/ VT is still present The rationale for this approach is that re-fibrillation during this 2-minute period is likely, even if the shock was initially successful. • Shock at next scheduled pause 2012-4-24 v24 B) My EMS agency stops to look (peek) after giving a shock, or uses "see-thru" technology • Shock→ immediate CPR • Brief (5-second max) pause at approximately 1 minute into CPR for rhythm check/confirmation • If VF/VT, resume CPR and give ALPS drug • Shock at next scheduled pause • If no VF/VT or unable to determine, resume CPR and await next scheduled rhythm analysis 2012-4-24 v24 C) My EMS agency stops to look (peek) when changing compressors at 2 minutes after a shock • After 2 minutes of CPR, as compressors are switched, quickly look at the rhythm • If VF/VT seen, resume CPR and charge monitor Give ALPS drug while charging→ then shock If not possible to give drug before shock, give it immediately afterward, as CPR is resumed • If no VF/VT or unable to determine, resume CPR and await next scheduled rhythm analysis 2012-4-24 v24 D) My EMS agency performs a formal rhythm analysis before each drug or shock intervention • Analyze rhythm at customary end of 2-minute CPR period (maximum 5 seconds) • If VF/ VT → start next 2-minute CPR period, give ALPS drug and charge defibrillator • Shock at next scheduled pause • If no VF/VT → resume CPR (or check pulse if organized rhythm seen) and treat per local protocol • If unable to determine rhythm, resume CPR and await next scheduled rhythm analysis 2012-4-24 v24 Should I give epinephrine or vasopressin? • Yes • Give epinephrine or vasopressin ASAP per local protocol If participating in CCC study, give within 5 minutes of arrival of ALS-capable EMS provider • ALPS drug does not cause hypotension; does not require concurrent vasopressor • If vasopressor not already just given, may administer epinephrine/vasopressin and first dose of ALPS drug back-to-back,* in order to expedite getting ALPS drug on board sooner *After flushing between drugs. 2012-4-24 v24 Is the first dose of the study drug two syringes or one? • Two syringes • First Dose = Syringe #1A and Syringe #1B • Second Dose = Syringe #2 • Exception = Small persons 2012-4-24 v24 What if the patient is small? (<100 lbs/45 kg) • Change from standard protocol • First Dose = Syringe #1A only • Second Dose = Syringe #1B only • Do not use Syringe #2 2012-4-24 v24 For any ALPS patient, what potential adverse events must be reported to ROC? • Non-function of ALPS syringe • Anaphylaxis (severe allergic reaction) • Pacing started in field • Seizures, shivering, myoclonus • Complications of IV or IO administration after ALPS given 2012-4-24 v24 What if VF/VT persists (or recurs) after I give all the study drug? Further management at discretion of providers… • May use other antiarrhythmics available to the agency (e.g., magnesium, beta blockers and/or procainamide) • Additional shock(s) • NO open label amiodarone or lidocaine in field permitted before or after ALPS drug* *Also excludes use of IO lidocaine to minimize pain when inserting/flushing IO line. 2012-4-24 v24 Should I start an infusion after achieving ROSC? • No known value of prophylactic antiarrhythmic drug infusions after cardiac arrest • Since no open label amiodarone or lidocaine can be given in the field, no infusions of these drugs should be given by EMS providers (includes no IO administration of lidocaine given to minimize pain when inserting or flushing IO line) • Duration of drug effect (“half-life”) should last until ED arrival • Use of open label lidocaine or amiodarone is permitted in hospital 2012-4-24 v24 What to do about wide complex tachycardia with pulse/BP? • ALPS is strictly for shock-resistant VF/pulseless VT needing CPR. This applies to all doses of ALPS drug. • If the rhythm doesn’t need CPR it shouldn’t get ALPS • A perfusing wide complex tachycardia can be a supraventricular rhythm with BBB and not need further treatment. Drugs can make it worse! • Transport to hospital for definitive diagnosis/care • If in doubt, consider synchronized electrical cardioversion 2012-4-24 v24 What if one or more syringes are broken or do not function? • If any syringe in the kit is broken upon opening, or does not function prior to giving… Stop ALPS, shut the box, and move on Use open label lidocaine or amiodarone, if needed Usual drug doses • If any portion of any ALPS syringe has already been given and syringe breaks or does not function… Stop ALPS, shut the box, and move on Use open label lidocaine or amiodarone, if needed Limit lidocaine to ≤ 200 mg total dose May use amiodarone at usual doses 2012-4-24 v24 What must be reported when any ALPS syringe is broken or does not function? • Quarantine ALPS kit with the damaged syringe • Document circumstances On patient record ROC-report form • Promptly notify ROC coordinator • Return ALPS kit with syringes to ROC coordinator 2012-4-24 v24 What should the Emergency Department do? • Notify ED that the patient may have received amiodarone or lidocaine or neither in the field • Written script left with ED • The script will indicate the drugs/doses the patient may have received in the field Limit lidocaine to an additional 100–120 mg over the next 2 hours in ED No restriction on additional amiodarone in ED All other ED treatments may be given as required 2012-4-24 v24 The Emergency Department really wants to know what drug we gave? • The ED script will include ROC physician name and phone number for the ED physician to contact for more information or questions Contact information for rare request to un-blind study drug • Defer questions to local ROC staff 2012-4-24 v24 Drug Kit Peel-off Barcode labels PCR Affix to… Hospital Notification Sheet 2012-4-24 v24 FDA Directive • When feasible, this written script will be presented to the LAR by the prehospital provider. • The acute circumstances of cardiac arrest may rarely, if ever, afford such opportunity on-scene without compromising patient care. • Accordingly, determining if or when presenting this script on-scene is feasible …will be left to clinical discretion of the provider. LAR Script May choose to use ROC or own EMS logo here Resuscitation Outcomes Consortium Amiodarone, Lidocaine or Neither (Placebo) for Out-OfHospital Cardiac Arrest Due to Ventricular Fibrillation or Tachycardia Principal Investigator: Study Coordinator: 2012-4-24 v24 “Your family member is having a cardiac arrest due to a very dangerous heart rhythm. We will do everything possible to save his/her life. [Local EMS Agency] are also performing an important study to find the best heart rhythm medication to use for this condition, in hope of saving more lives. Unless you say no, we will give this treatment, in addition to all other standard treatments for your family member. You will receive more information about this later, and a chance to ask questions.” Do I carry out ALPS and CCC at the same time? Yes, both protocols can be done at the same time. CCC 2012-4-24 v24 ALPS Five Take-to-the-Street Principles of ALPS Think of the ALPS drug as you would about any antiarrhythmic for VF/pulseless VT and use it accordingly… • Prioritize vascular access • Expedite ALPS drug for shock-resistant VF/VT rhythms requiring CPR VF/pulseless VT that persists/recurs after ≥1 shocks (“It’s baaack!”) OK to give vasopressor plus ALPS back-to-back to speed treatment* Give ALPS drug ASAP from when recurrent VF/VT last seen (≤2 minutes) • Judge patient’s size Normal: 2 syringes→ 1 syringe rescue Small (<100 lbs/45 kg): 1 syringe→ 1 syringe rescue *After flushing between drugs 2012-4-24 v24 Five Take-to-the-Street Principles of ALPS continued… • Document when ALPS drug given Time-stamp each dose of ALPS drug Document shock number that follows each dose of ALPS drug • Inform ED/Notify ROC of ALPS use 2012-4-24 v24 Questions?