Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
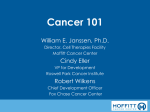
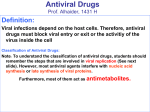
Cytomegalovirus, Human Herpesvirus-6, and Human Herpesvirus-7 in Hematological Patients Duncan A. Clark, Vincent C. Emery, and Paul D. Griffiths The prototype member of the Betaherpesvirinae subfamily, cytomegalovirus (CMV), is the most important infectious pathogen in transplant recipients, including those receiving bone marrow or stem cell grafts. Overt CMV disease such as pneumonitis is notoriously difficult to treat. Antiviral prophylaxis, rapid diagnostic tests to identify CMV infection, and preemptive antiviral chemotherapy are significant improvements in the management of CMV. As the kinetics of the immune response to CMV become better defined, immunotherapeutic approaches should be introduced to complement current management strategies. Two newly identified betaherpesviruses, human herpesvirus-6 (HHV-6) and human herpesvirus-7 (HHV-7), are genetically more closely related to each other than to CMV. Both are highly prevalent in the general population and infections post– bone marrow transplantation are common. These viruses are not as pathogenic as CMV but HHV-6 at least can cause disease such as encephalitis, hepatitis, and bone marrow suppression. Both of these newer herpesviruses are potentially susceptible to existing and licensed antiherpesvirus drugs. Semin Hematol 40:154-162. © 2003 Elsevier Inc. All rights reserved. T HE BETAHERPESVIRUS subfamily includes cytomegalovirus (CMV) and the closely related human herpesviruses-6 and -7 (HHV-6 and HHV-7). CMV is well known as the most important infectious pathogen in transplant recipients, and there is now accumulating evidence that HHV-6 and HHV-7 also exhibit enhanced pathogenicity in the immunocompromised host. This review will consider the relevance of infection with these viruses in hematology patients. Cytomegalovirus CMV infects approximately 60% of adults in developed countries and almost all of those in developing nations. The virus is usually acquired by close contact between individuals, mainly by the transfer of saliva but also through intrauterine or perinatal infection. In addition, iatrogenic transmission can occur, as from donated solid organs and through blood transfusion.78 Primary infections are usually asymptomatic although delayed infection in adulthood can cause infectious mononucleosis–like illness. CMV establishes life-long infection after primary infection. Persistence likely includes both a latent state with infectious virus only produced during episodes of reactivation, and chronic replication with continuous or frequent but intermittent production From the Department of Virology, Royal Free and University College Medical School of UCL, London, UK. Address correspondence to Duncan A. Clark, PhD, Department of Virology, Royal Free and University College Medical School, Royal Free Campus, Rowland Hill Street, London NW3 2PF, UK. © 2003 Elsevier Inc. All rights reserved. 0037-1963/03/4002-0006$30.00/0 doi:10.1053/shem.2003.50015 154 of infectious virus. Monocyte/macrophages and endothelial cells are implicated as sites of CMV persistence and latency, and replication of the virus in these two cell types is likely to be important in maintaining life-long infection.42,82,87 CMV causes a variety of diseases in the immunocompromised host (Table 1), although the anatomical sites most commonly affected vary among patient groups. In addition to these direct end-organ diseases, CMV has repeatedly been associated with rejection of solid organs or graft-versus-host disease (GvHD) in bone marrow transplantation. Secondary bacterial and fungal infections also are frequent after CMV infection and, together with rejection and GvHD, are considered indirect effects of the virus.79 CMV Infection Following Bone Marrow Transplantation Historically, CMV has been one of the most feared infectious complications following bone marrow transplantation. CMV disease in this setting can manifest as pneumonitis, gastrointestinal syndromes, hepatitis, bone marrow suppression, and occasionally retinitis (Table 1). The lungs of the recipients become a site for CMV replication, and CMV pneumonitis was one of the major diseases following transplantation which, once established, led to high morbidity and mortality. Prior to the advent of more rapid diagnostic methods, the slow growth of CMV in vitro allowed a diagnosis of active CMV infection only late in the clinical course. Under these conditions, antiviral therapeutic intervention was of limited success.74 As discussed below, in more recent years antiviral prophylaxis36 and/or improved diagnostic methods and correct deployment of antiviral chemotherapy against CMV22 have dramatically re- Seminars in Hematology, Vol 40, No 2 (April), 2003: pp 154-162 Betaherpesviruses in Hematological Patients Table 1. CMV Diseases in Transplant Recipients Symptoms Solid Transplant Bone Marrow Transplant Fever/hepatitis Gastrointestinal Retinitis Pneumonitis Immunosuppression Myelosuppression Rejection, GvHD ⫹⫹ ⫹ ⫹ ⫹ ⫹ ⫹ ⫹ ⫹ ⫹⫹ ⫹ ⫹⫹ ? Adapted from Griffiths et al,34 by permission of Oxford University Press. duced the incidence of CMV pneumonitis in hematology patients and also led to improved outcomes in infected patients. CMV Replication and Viral Burden CMV has the reputation of a slowly growing virus. While true in conventional in vitro culture systems in primary human fibroblasts, it is unlikely that such an artificial system parallels in vivo complexity. The recent application of dynamic mathematical modeling has illuminated our understanding of the replication rate of many human pathogens in vivo. Using such analyses, we have shown that CMV replication in vivo occurs rapidly, with doubling times of approximately 1 day.23 These findings have implications for the development of disease and the successful treatment of infection in patients with hematological malignancies undergoing bone marrow transplantation. Many risk factors for CMV disease have been defined in prospective studies spanning 20 years. Using conventional cell culture methods and subsequently rapid culture methods such as shell vial culture and the detection of early antigen fluorescent foci (DEAFF) test, active CMV replication in blood (viremia) was associated with an increased risk of development of CMV disease post– bone marrow transplantation.46,64,93 Subsequently, the detection of virus using more sensitive methods such as antigenemia assays (where polymorphonuclear cells expressing the ppUL83 protein of CMV are identified using specific monoclonal antibodies) and the polymerase chain reaction (PCR) have shown that both CMV presence and the quantity of virus found in the blood are risk factors for CMV disease.4,7,21,25,31,52,73,86 The traditional major predictor for a high risk of CMV disease has been the transplantation of donor marrow from CMV-seronegative individuals into a recipient who is already CMV-seropositive. Under such conditions, the donor marrow is naive to CMV, and when endogenous CMV is reactivated the marrow-derived immune cells mount a primary immune 155 response to control replication. In contrast, donor and recipient seropositivity for CMV is associated with a lower risk of CMV disease, probably due to the transfer of antiviral immunity with donor marrow.35 These qualitative effects of donorrecipient serostatus manifest themselves quantitatively through viral load, such that patients in the D⫺R⫹ category exhibit higher viral loads (and hence a higher probability of disease) post-transplantation compared to patients who are in the D⫹R⫹ or D⫹R⫺ categories (Fig 1).31 Regression of the probability of CMV disease with viral load showed an acute transition at critical quantities of virus, resulting in a large increase in disease risk for relatively small increases in viral load. As a consequence, viral load levels can be defined that identify patients at risk of disease with reasonable sensitivity and specificity. The advent of real-time PCR monitoring of viral load is allowing these concepts to be translated practically, to identify patients at risk of future CMV disease and to initiate therapy in a timely, cost-effective manner.60,67,73,86 Immune Control of CMV Following Bone Marrow Transplantation T cells are critical in the control of CMV replication. Extensive research has shown that the cytotoxic T lymphocyte (CTL) response to CMV is dominated by activity against the pp65 (ppUL83) tegument protein, with contributions from T cells directed against the immediate early 1 protein among others.95 In the immunocompetent host, CD8 T cells specific for ppUL83 can be visualized using human leukocyte Figure 1. CMV peak virus load and its association with CMV serostatus at the time of bone marrow transplantation. (F) Patients who experienced CMV disease; (E) asymptomatic patients. Median viral load in the R⫹D⫺ group was significantly higher than in the R⫹D⫹ group. Adapted with permission.31 156 Clark, Emery, and Griffiths antigen (HLA) tetramer technology (⬃1%),29,37 and in bone marrow transplant recipients undergoing high-level CMV replication, frequencies as high as 20% of the total CD8⫹ T-cell population have been observed.3,32 Using a series of phenotypic markers, these CD8 T cells have a late effector phenotype (CD45RO⫹, CD27⫺, CCR7⫺, or CD45RA⫹, CD27⫺, CCR7⫺) and are therefore fully differentiated cytotoxic T cells.1,26 A large proportion of CMV-specific CD8 T cells reside in the CD45RA population traditionally regarded as naive T cells. For CD4 T-cell helper responses, there is a predominance in responses against glycoprotein B (gB, UL55; a major target for neutralizing antibody response) and ppUL83, although individual epitopes restricted by HLA class II alleles have not been as extensively mapped as have HLA class I–restricted peptides.5,53 Nevertheless, in immunocompetent individuals the T-helper responses against total CMV antigens also are relatively high and appear to be important to maintain CMV-specific CD8 T cells.26 In the context of bone marrow transplant, the engrafting marrow must cope with a range of infectious agents experienced by the stem cell recipient. CD4 T-helper cells regenerate relatively slowly following allogeneic bone marrow transplantation, and so appropriate help to CD8 T cells able to control CMV replication may be limited. The importance of the regeneration of T-cell immunity after bone marrow transplantation for the control of CMV replication has been demonstrated in studies of CMV-specific T cells and by adoptive transfer of CMV-specific T cells.3,20,75 HLA tetramer technology50 has improved our understanding of the kinetics of regeneration of CD8-specific CTL responses against CMV following transplantation and provided insight into the level of CD8 T cells required to ensure that CMV infection is maintained at very low levels. An absolute CMV CD8 T-cell level of approximately 108 cells/L was associated with total suppression of CMV replication, at least at the level of sensitivity of the PCR assay employed (⬃200 genomes/mL blood).3 However, in patients who experienced a period of active CMV infection (PCR positivity ⬎ 200 genomes/mL blood), the median CMV CD8 T-cell frequency was substantially lower, at approximately 107 cells/L, whereas during periods where replication was suppressed, the median frequency increased to about 3 ⫻ 107 cells/L. From these and other data it would appear that certain threshold levels of CMV CD8 T cells may be required to effectively suppress CMV replication; when the absolute number of cells is below this threshold, high levels of CMV replication ensue, leading to a high risk of disease. A variety of mechanisms might render the CMV CD8 T-cell population suboptimal for control of viral replication, including slow reconstitution of T-helper Figure 2. CMV immunity in a patient following sibling donor peripheral blood stem cell transplantation (CMV serostatus D⫺/ R⫹). In the top panel are simultaneously represented the levels of CMV peptide AE42 tetramer-specific (Tet⫹) T cells expressed as an absolute number per liter of blood (䢇——䢇, unbroken line) or as a percentage of CD8⫹ T cells (} – – – }). The periods of prednisolone, ganciclovir (G), and foscarnet (F) therapy are also shown. The CMV viral load is shown in the lower panel (䢇——䢇, unbroken line). Adapted with permission of the University of Chicago Press.3 responses in the post-transplant period and the effects of immunosuppressive drugs such as corticosteroids used to control GvHD. Prolonged exposure to prednisolone is associated with relentless suppression of CMV specific CD8 T cells and a consequent increase in viral load (Fig 2).3 The powerful effect of CMV-specific T cells in limiting CMV replication was dramatically demonstrated when an adoptive immunotherapeutic approach achieved suppression of CMV replication in patients who had high viral loads that were unresponsive to conventional antiviral chemotherapy.20 Studies are in progress to determine whether a combination of viral load measurement and CMV-specific CD8 T-cell determinations might provide complementary information to identify patients at high risk of developing CMV infection and disease following transplantation. Therapeutic Interventions Against CMV Following Bone Marrow Transplantation Two anti-CMV agents have been the mainstay for the treatment of established disease in the hematology patient: ganciclovir (an acyclic guanosine analogue) and foscarnet (an analogue of inorganic pyrophosphate). Both block activity of CMV DNA polymerase (UL54 gene), ganciclovir by acting as a competitive inhibitor of the natural substrate and thus causing chain termination, and foscarnet as a product inhibitor of the DNA synthetic reaction catalyzed by the Betaherpesviruses in Hematological Patients viral-specific DNA polymerase. For ganciclovir to be effective it must be phosphorylated to the triphosphate moiety; the first stage of phosphorylation is effected by a viral specific protein kinase encoded by the UL97 gene, while subsequent phosphorylation steps are catalyzed by cellular kinases. Ganciclovir therapy (5 mg/kg twice daily) has an antiviral efficacy of approximately 91.5% at controlling CMV replication.23 Similar estimates for the efficacy of foscarnet are not available, but trials comparing ganciclovir with foscarnet indicate much similarity.76 The effectiveness of preemptive therapy triggered by antigenemia positivity or PCR positivity has been shown in two trials6,19; in both the treatment was initiated far earlier than using conventional cell culture methods and patients required less overall ganciclovir therapy with the benefits of minimizing the associated neutropenia. Consequently, many centers now use antigenemia- or PCR-triggered preemptive therapy (usually 14 days) for patient management. An alternative approach to reduce the probability of CMV infection/disease has been the prophylactic deployment of agents such as aciclovir and/or ganciclovir. Placebo-controlled clinical trials showed that high-dose aciclovir could reduce CMV disease and also improve survival.65,72 More recently, the availability of the pro-drug of aciclovir, valaciclovir, which produces increased oral bioavailability, has been shown to reduce the incidence of CMV disease in bone marrow transplant recipients54 and also in other immunocompromised hosts.56 Intravenous, or more recently oral ganciclovir (1 g three times per day), have produced clinical benefit in controlled trials.30,96 Therapy up to 100 days following bone marrow engraftment is effective at controlling CMV infection and its consequent disease. However, there are a variety of ramifications to these strategies. First, since CMV replication is substantially inhibited by oral ganciclovir (this formulation has an antiviral efficacy of approximately 46.5%),23 the regenerating immune system is not exposed to sufficient levels of viral replication to elicit a T-cell–mediated immune response, and so patients remain unprimed to CMV following the cessation of prophylaxis.16 Second, because the drug concentration is inadequate to fully eradicate replication during the period of prophylaxis, coupled with the lack of regeneration of an early immune response against CMV, viremia can appear following the cessation of prophylaxis (usually between 3 and 4 weeks) especially in the highrisk D⫺R⫹ group. Unfortunately, late CMV infection has been associated with a high incidence of late CMV disease,68 which has been difficult to manage, stimulating many centers to pursue aggressive preemptive therapy triggered by antigenemia or PCR positivity. Although drug resistance is an emerging question 157 in the context of CMV,24,51 a recent report has shown that antigenemia-driven preemptive therapy with ganciclovir did not produce ganciclovir-resistant viruses: there was no selection of viruses with mutations in UL97, despite recurrence of antigenemia.28 A major risk factor for the recurrent viremia appears to be the slope of decline in viral load during initial therapy, so that a tardy viral load response to intervention increases the likelihood of subsequent viremic episodes.38 Intravenous and oral formulations of ganciclovir have been used extensively, but the prodrug of ganciclovir, valganciclovir is now available.62,71 Although there are no results from controlled trials of this compound in bone marrow transplant recipients, the prodrug should provide levels of ganciclovir in the blood that are comparable to intravenous ganciclovir, but attention to poor absorption may be necessary in the presence of gut GvHD. Valganciclovir likely will replace intravenous ganciclovir. Since the effective concentration of ganciclovir has been increased over oral ganciclovir, the antiviral efficacy achieved should be also be greater. How use of valganciclovir in treatment and prophylaxis will affect late infection and generation of ganciclovir-resistant viruses remains to be defined, but analysis of samples obtained from a clinical trial of valganciclovir versus intravenous ganciclovir in HIV-infected individuals showed that the frequency of ganciclovir-resistant strains of CMV were comparable between the two treatment groups.8 Human Herpevirus-6 HHV-6 is highly prevalent worldwide and infection usually occurs in early childhood. In young children, HHV-6 is a causative agent of febrile illness including exanthem subitum (ES).97 Two variants of HHV-6 have been defined (termed A and B), and they are increasingly viewed as closely related although distinct species.18 HHV-6 is tropic for T lymphocytes and neural cells but has the ability to infect a wide variety of cell types in vitro.13 HHV-6 utilizes CD46 as a cellular receptor (CD46, also termed membrane cofactor protein, is a member of a family of complement regulators).80 Activated CD4⫹ T cells and monocytes/macrophages appear to be the preferential targets for replication in vivo.48,83 Similar to CMV, HHV-6 remains in the host lifelong following primary infection. The virus, predominantly variant B, can be detected in the peripheral blood of healthy individuals by nested PCR when sufficient quantities of DNA are tested.14 The actual site of latency has yet to be established, although candidates include monocytes47 and early bone marrow progenitor cells.58 An uncommon form of 158 Clark, Emery, and Griffiths Table 2. Prospective Studies of HHV-6 Infection Following Bone Marrow or Stem Cell Transplantation Study Method of Detection Observed Disease Wilborn et al94 Appleton et al2 Kadakia et al43 Wang et al91 Chan et al11 Cone et al15 Maeda et al61 Ljungman et al55 Imbert-Marcille et al39 Yoshikawa et al99 PCR PCR⫹IHC VI PCR PCR PCR PCR QCPCR PCR VI GvHD* GvHD* (PCR in skin/rectal biopsies) None Delayed granulocyte and platelet engraftment* None Rash* Delayed platelet engraftment Viral load correlated with delayed platelet engraftment Myelosuppression and fever Rash* * Analysis on subgroup of patient population Abbreviations: PCR, polymerase chain reaction; QCPCR, quantitative competitive PCR, VI, virus isolation; IHC, immunohistochemistry. Updated and adapted with permission.13 Copyright 2000. © John Wiley & Sons Ltd. HHV-6 persistence is characterized by integration of apparently whole-genome length HHV-6 sequences into host-cell chromosomes,89 but the clinical relevance of this unusual biology, if any, is not clear. Integration sites have been mapped to chromosome 17p13.3, chromosome 22q13, and chromosome 1q44 in different individuals. The inheritance of chromosomally integrated HHV-6 also has been reported.17 HHV-6 and Lymphoproliferative Disease The involvement of HHV-6 in a range of hematological malignancies has been investigated with largely negative findings.13 In situ detection of HHV-6 has been demonstrated in the abnormal cells of T-cell chronic lymphoproliferative disease9 and sinus histiocytosis with massive lymphadenopathy (RosaiDorfman disease).57 Further studies are necessary to determine if HHV-6 is causally associated with either of these disorders. HHV-6 Infection Following Bone Marrow Transplantation Infection with HHV-6 following bone marrow transplantation is common and, considering the high rate of seroprevalence of the population, is likely to be due almost always to reactivation of recipient’s virus or reinfection from the donor. The virus has been found in 28% of bone marrow samples from healthy individuals, suggesting that it can be transmitted from the donor to the recipient,27 and cases of primary infection have been reported.49 HHV-6A and especially HHV-6B infections have been detected in the post-transplant period; most HHV-6 infections occur within the first 4 weeks.39,61,99 Case reports and selective studies have associated HHV-6 with a range of clinical diseases following bone marrow transplantation, including encephalitis, idiopathic interstitial pneumonitis, hepatitis, early and late graft failure, and bone marrow suppression.12,13 In vitro, both HHV-6 variants are able to suppress the maturation and growth of normal bone marrow precursors, including granulocyte/macrophage, erythroid, and megakaryocytic lineages.40,41 The detection of HHV-6 in cerebrospinal fluid by PCR also has been associated with a range of CNS disease in bone marrow transplant recipients.90,92,100 Prospective studies have been conducted to measure the medical impact of HHV-6 following stem cell transplantation (Table 2). Some have reported associations between HHV-6 and delayed engraftment, myelosuppression, and fever.39,61 HHV-6 viral load also significantly correlated with delayed platelet engraftment following stem cell transplantation.55 However, other analyses have failed to show a clear association between HHV-6 and disease when the whole study population was analyzed2,11,15,43,91,94; subgroup analysis sometimes has linked the virus to GvHD,94 delayed engraftment,91 and rash.15,99 Contradictory findings in prospective studies are likely to represent variations in the demographics of transplant populations, their medical care, and, importantly, the methods used in detection of virus infection (although the majority have employed PCR). Most authors have found a low incidence of the disease types previously identified by case reports when large numbes of bone marrow transplant recipients were examined. Human Herpesvirus-7 As with HHV-6, HHV-7 also is highly prevalent worldwide and infection usually occurs in early childhood, perhaps slightly delayed in comparison to HHV-6. Similar to HHV-6, HHV-7 can cause febrile 159 Betaherpesviruses in Hematological Patients Table 3. Prospective Studies of HHV-7 Infection Following Transplantation Study Transplant Type Method of Detection Wang et al91 Chan et al11 Maeda et al61 Osman et al70 Kidd et al45 Bone marrow Bone marrow Bone marrow Renal Renal PCR PCR PCR PCR PCR Tong et al88 Griffiths et al33 Mendez et al63 Renal Liver Liver PCR PCR PCR Observed Disease None Delayed engraftment* None CMV disease CMV disease Graft rejection* CMV disease None CMV disease * Analysis on subgroup of patient population. illness in young children.85 Analysis of the HHV-7 genome shows that it is most closely related to HHV6.69 HHV-7 utilizes CD4 as a cellular receptor to infect T cells59 and although CXCR4 was initially reported to be downregulated in infected cells,81 more recent studies suggest that this molecule is not a co-receptor.102 The virus has also been shown to productively infect macrophages in vitro.101 Similar to HHV-6, HHV-7 can be detected in the peripheral blood of healthy individuals by nested PCR,44 although the actual site of latency has yet to be identified. Monocyte/macrophages harbor virus in a nonreplicating form following infection in vitro.101 HHV-7 Following Transplantation Fewer studies have examined the role of HHV-7 infection post-transplantation (Table 3). Similar to HHV-6, active HHV-7 infection does occur, likely due to reactivation of recipient’s virus or reinfection, given the high seroprevalence in the population. HHV-7 DNA has been detected by PCR in 50% of bone marrow samples from healthy persons,27 including CD34⫹ and CD34⫺ cell fractions,66 suggesting that donor material may be a potential source of virus. Prospective studies in bone marrow transplant recipients have not found an obvious correlation between HHV-7 infection and a range of clinical endpoints including GvHD and engraftment61,91 (Table 3). The detection of HHV-7 in peripheral blood by PCR during the early post-transplantation period was associated with a longer time to neutrophil engraftment.11 In vitro HHV-7 was not suppressive of granulocyte/macrophage, erythroid, and megakaryocyte colony formation in some experiments,40,41 but inoculation of cord blood CD34⫹ cells in vitro with HHV-7 significantly decreased the number of pluripotent (granulocyte/monocyte/erythroid/megakaryocyte) progenitors in semisolid assays with a more modest effect on committed (granulocyte/macrophage and erythroid) progenitors.66 In addition, HHV-7 appeared to hasten differentiation of cord blood CD34⫹ cells to myeloid but not erythroid cells.66 Thus, there are in vitro data to suggest the ability of HHV-7 to perturb the maturation of haematopoietic progenitor cells. Two cases of HHV-7 encephalitis, one fatal, following bone marrow or stem cell transplantation have been reported.10,11 A number of prospective studies have followed solid organ transplant patients (Table 3).33,45,63,70,88 In renal recipients, concomitant CMV and HHV-7 infection was associated with a greater risk of developing CMV disease70 (Table 3). Others have reported a similar association between HHV-7 and an increased risk of CMV disease,45,63,88 but putative mechanisms are unknown. HHV-6 and HHV-7 Antiviral Susceptibility Ganciclovir, foscarnet, and cidofovir have been reported to be inhibitors of HHV-6 and HHV-7 replication in vitro,84 although not consistently.77,98 There have been no controlled trials of antiviral therapy against HHV-6 or HHV-7 infection, but individual published cases suggested a clinical response to treatment of HHV-6 disease (encephalitis/CNS disease and bone marrow suppression) after bone marrow transplantation, using either ganciclovir or foscarnet or both.12 Currently licensed antiherpetic compounds may be effective against HHV-6 and HHV-7, but treatment strategies need to be formulated through appropriate clinical protocols. Conclusion CMV remains an important pathogen in hematological patients, specifically bone marrow/stem cell transplant recipients. However, important advances have been made in the monitoring and treatment of CMV infection in these patients. The future use of immunotherapeutic approaches may complement the current management strategies. The clinical relevance of HHV-6 and HHV-7 in hematological patients is certainly more restricted than CMV, although accumulating evidence highlights the ability of HHV-6 to cause disease post bone marrow/stem cell transplantation. References 1. Appay V, Dunbar PR, Callan M, et al: Memory CD8⫹ T cells vary in differentiation phenotype in different persistent virus infections. Nat Med 8:379-385, 2002 2. Appleton AL, Sviland L, Peiris JS, et al: Human herpesvirus-6 infection in marrow graft recipients: Role in pathogenesis of graft-versus-host disease. Bone Marrow Transplant 16:777-782, 1995 160 Clark, Emery, and Griffiths 3. Aubert G, Hassan-Walker AF, Madrigal JA, et al: Cytomegalovirus-specific cellular immune responses and viremia in recipients of allogeneic stem cell transplants. J Infect Dis 184:955-963, 2001 4. Baldanti F, Revello MG, Percivalle E, et al: Use of the human cytomegalovirus (HCMV) antigenemia assay for diagnosis and monitoring of HCMV infections and detection of antiviral drug resistance in the immunocompromised. J Clin Virol 11:51-60, 1998 5. Beninga J, Kropff B, Mach M: Comparative analysis of fourteen individual human cytomegalovirus proteins for helper T cell response. J Gen Virol 76:153-160, 1995 6. Boeckh M, Gooley TA, Myerson D, et al: Cytomegalovirus pp65 antigenemia-guided early treatment with ganciclovir versus ganciclovir at engraftment after allogeneic marrow transplantation: A randomized double-blind study. Blood 88:4063-4071, 1996 7. Boivin G, Belanger R, Delage R, et al: Quantitative analysis of cytomegalovirus (CMV) viremia using the pp65 antigenemia assay and the Cobas Amplicor CMV Monitor PCR test after blood and marrow allogeneic transplantation. J Clin Microbiol 38:4356-4360, 2000 8. Boivin G, Gilbert C, Gaudreau A, et al: Rate of emergence of cytomegalovirus (CMV) mutations in leukocytes of patients with acquired immunodeficiency syndrome who are receiving valganciclovir as induction and maintenance therapy for CMV retinitis. J Infect Dis 184:1598-1602, 2001 9. Braun DK, Pellett PE, Hanson CA: Presence and expression of human herpesvirus 6 in peripheral blood mononuclear cells of S100-positive, T cell chronic lymphoproliferative disease. J Infect Dis 171:1351-1355, 1995 10. Chan PK, Chik KW, To KF, et al: Case report: human herpesvirus 7 associated fatal encephalitis in a peripheral blood stem cell transplant recipient. J Med Virol 66:493496, 2002 11. Chan PK, Peiris JS, Yuen KY, et al: Human herpesvirus-6 and human herpesvirus-7 infections in bone marrow transplant recipients. J Med Virol 53:295-305, 1997 12. Clark DA, Griffiths PD: Human herpesvirus 6: Relevance of infection in the immunocompromised host. Br J Haematol (in press) 13. Clark DA: Human herpesvirus 6. Rev Med Virol 10:155-173, 2000 14. Clark DA, Ait-Khaled M, Wheeler AC, et al: Quantification of human herpesvirus 6 in immunocompetent persons and post-mortem tissues from AIDS patients by PCR. J Gen Virol 77:2271-2275, 1996 15. Cone RW, Huang ML, Corey L, et al: Human herpesvirus 6 infections after bone marrow transplantation: Clinical and virologic manifestations. J Infect Dis 179:311-318, 1999 16. Cwynarski K, Ainsworth J, Cobbold M, et al: Direct visualization of cytomegalovirus-specific T-cell reconstitution after allogeneic stem cell transplantation. Blood 97:12321240, 2001 17. Daibata M, Taguchi T, Nemoto Y, et al: Inheritance of chromosomally integrated human herpesvirus 6 DNA. Blood 94:1545-1549, 1999 18. Dominguez G, Dambaugh TR, Stamey FR, et al: Human herpesvirus 6B genome sequence: Coding content and comparison with human herpesvirus 6A. J Virol 73:8040-8052, 1999 19. Einsele H, Ehninger G, Hebart H, et al: Polymerase chain reaction monitoring reduces the incidence of cytomegalovirus disease and the duration and side effects of antiviral therapy after bone marrow transplantation. Blood 86:28152820, 1995 20. Einsele H, Roosnek E, Rufer N, et al: Infusion of cytomegalovirus (CMV)-specific T cells for the treatment of CMV infection not responding to antiviral chemotherapy. Blood 99:3916-3922, 2002 21. Einsele H, Steidle M, Vallbracht A, et al: Early occurrence of human cytomegalovirus infection after bone marrow transplantation as demonstrated by the polymerase chain reaction technique. Blood 77:1104-1110, 1991 22. Emery VC: Prophylaxis for CMV should not now replace pre-emptive therapy in solid organ transplantation. Rev Med Virol 11:83-86, 2001 23. Emery VC, Cope AV, Bowen EF, et al: The dynamics of human cytomegalovirus replication in vivo. J Exp Med 190: 177-182, 1999 24. Emery VC, Griffiths PD: Prediction of cytomegalovirus load and resistance patterns after antiviral chemotherapy. Proc Natl Acad Sci USA 97:8039-8044, 2000 25. Emery VC, Sabin CA, Cope AV, et al: Application of viralload kinetics to identify patients who develop cytomegalovirus disease after transplantation. Lancet 355:2032-2036, 2000 26. Gamadia LE, Rentenaar RJ, Baars PA, et al: Differentiation of cytomegalovirus-specific CD8(⫹) T cells in healthy and immunosuppressed virus carriers. Blood 98:754-761, 2001 27. Gautheret-Dejean A, Dejean O, Vastel L, et al: Human herpesvirus-6 and human herpesvirus-7 in the bone marrow from healthy subjects. Transplantation 69:1722-1723, 2000 28. Gilbert C, Roy J, Belanger R, et al: Lack of emergence of cytomegalovirus UL97 mutations conferring ganciclovir (GCV) resistance following preemptive GCV therapy in allogeneic stem cell transplant recipients. Antimicrob Agents Chemother 45:3669-3671, 2001 29. Gillespie GM, Wills MR, Appay V, et al: Functional heterogeneity and high frequencies of cytomegalovirus- specific CD8(⫹) T lymphocytes in healthy seropositive donors. J Virol 74:8140-8150, 2000 30. Goodrich JM, Bowden RA, Fisher L, et al: Ganciclovir prophylaxis to prevent cytomegalovirus disease after allogeneic marrow transplant. Ann Intern Med 118:173-178, 1993 31. Gor D, Sabin C, Prentice HG, et al: Longitudinal fluctuations in cytomegalovirus load in bone marrow transplant patients: relationship between peak virus load, donor/recipient serostatus, acute GVHD and CMV disease. Bone Marrow Transplant 21:597-605, 1998 32. Gratama JW, van Esser JW, Lamers CH, et al: Tetramerbased quantification of cytomegalovirus (CMV)-specific CD8⫹ T lymphocytes in T-cell-depleted stem cell grafts and after transplantation may identify patients at risk for progressive CMV infection. Blood 98:1358-1364, 2001 33. Griffiths PD, Ait-Khaled M, Bearcroft CP, et al: Human herpesvirus 6 and 7 as potential pathogens after liver transplant: Prospective comparison with the effect of cytomegalovirus. J Med Virol 59:496-501, 1999 34. Griffiths PD, Clark DA, Emery VC: Betaherpesviruses in transplant recipients. J Antimicrob Chemother 45:29-34, 2000 (suppl T3) 35. Grob JP, Grundy JE, Prentice HG, et al: Immune donors can protect marrow-transplant recipients from severe cytomegalovirus infections. Lancet 1:774-776, 1987 36. Hart GD, Paya CV: Prophylaxis for CMV should now replace pre-emptive therapy in solid organ transplantation. Rev Med Virol 11:73-81, 2001 37. Hassan-Walker AF, Vargas Cuero AL, Mattes FM, et al: CD8⫹ cytotoxic lymphocyte responses against cytomegalovirus after liver transplantation: correlation with time from Betaherpesviruses in Hematological Patients 38. 39. 40. 41. 42. 43. 44. 45. 46. 47. 48. 49. 50. 51. 52. 53. 54. transplant to receipt of tacrolimus. J Infect Dis 183:835-843, 2001 Humar A, Kumar D, Boivin G, et al: Cytomegalovirus (CMV) virus load kinetics to predict recurrent disease in solid-organ transplant patients with CMV disease. J Infect Dis 186:829-833, 2002 Imbert-Marcille BM, Tang XW, Lepelletier D, et al: Human herpesvirus 6 infection after autologous or allogeneic stem cell transplantation: A single-center prospective longitudinal study of 92 patients. Clin Infect Dis 31:881-886, 2000 Isomura H, Yamada M, Yoshida M, et al: Suppressive effects of human herpesvirus 6 on in vitro colony formation of hematopoietic progenitor cells. J Med Virol 52:406-412, 1997 Isomura H, Yoshida M, Namba H, et al: Suppressive effects of human herpesvirus-6 on thrombopoietin-inducible megakaryocytic colony formation in vitro. J Gen Virol 81: 663-673, 2000 Jarvis MA, Nelson JA: Human cytomegalovirus persistence and latency in endothelial cells and macrophages. Curr Opin Microbiol 5:403-407, 2002 Kadakia MP, Rybka WB, Stewart JA, et al: Human herpesvirus 6: Infection and disease following autologous and allogeneic bone marrow transplantation. Blood 87:5341-5354, 1996 Kidd IM, Clark DA, Ait-Khaled M, et al: Measurement of human herpesvirus 7 load in peripheral blood and saliva of healthy subjects by quantitative polymerase chain reaction. J Infect Dis 174:396-401, 1996 Kidd IM, Clark DA, Sabin CA, et al: Prospective study of human betaherpesviruses after renal transplantation: association of human herpesvirus 7 and cytomegalovirus coinfection with cytomegalovirus disease and increased rejection. Transplantation 69:2400-2404, 2000 Kidd IM, Fox JC, Pillay D, et al: Provision of prognostic information in immunocompromised patients by routine application of the polymerase chain reaction for cytomegalovirus. Transplantation 56:867-871, 1993 Kondo K, Kondo T, Okuno T, et al: Latent human herpesvirus 6 infection of human monocytes/macrophages. J Gen Virol 72:1401-1408, 1991 Kondo K, Kondo T, Shimada K, et al: Strong interaction between human herpesvirus 6 and peripheral blood monocytes/macrophages during acute infection. J Med Virol 67: 364-369, 2002 Lau YL, Peiris M, Chan GC, et al: Primary human herpes virus 6 infection transmitted from donor to recipient through bone marrow infusion. Bone Marrow Transplant 21:1063-1066, 1998 Lechner F, Cuero AL, Kantzanou M, et al: Studies of human antiviral CD8⫹ lymphocytes using class I peptide tetramers. Rev Med Virol 11:11-22, 2001 Limaye AP, Corey L, Koelle DM, et al: Emergence of ganciclovir-resistant cytomegalovirus disease among recipients of solid-organ transplants. Lancet 356:645-649, 2000 Limaye AP, Huang ML, Leisenring W, et al: Cytomegalovirus (CMV) DNA load in plasma for the diagnosis of CMV disease before engraftment in hematopoietic stem-cell transplant recipients. J Infect Dis 183:377-382, 2001 Liu YN, Curtsinger J, Donahue PR, et al: Molecular analysis of the immune response to human cytomegalovirus glycoprotein B. I. Mapping of HLA-restricted helper T cell epitopes on gp93. J Gen Virol 74:2207-2214, 1993 Ljungman P, de La CR, Milpied N, et al: Randomized study of valacyclovir as prophylaxis against cytomegalovirus reac- 55. 56. 57. 58. 59. 60. 61. 62. 63. 64. 65. 66. 67. 68. 69. 70. 71. 72. 161 tivation in recipients of allogeneic bone marrow transplants. Blood 99:3050-3056, 2002 Ljungman P, Wang FZ, Clark DA, et al: High levels of human herpesvirus 6 DNA in peripheral blood leucocytes are correlated to platelet engraftment and disease in allogeneic stem cell transplant patients. Br J Haematol 111:774781, 2000 Lowance D, Neumayer HH, Legendre CM, et al: Valacyclovir for the prevention of cytomegalovirus disease after renal transplantation. N Engl J Med 340:1462-1470, 1999 Luppi M, Barozzi P, Garber R, et al: Expression of human herpesvirus-6 antigens in benign and malignant lymphoproliferative diseases. Am J Pathol 153:815-823, 1998 Luppi M, Barozzi P, Morris C, et al: Human herpesvirus 6 latently infects early bone marrow progenitors in vivo. J Virol 73:754-759, 1999 Lusso P, Secchiero P, Crowley RW, et al: CD4 is a critical component of the receptor for human herpesvirus 7: Interference with human immunodeficiency virus. Proc Natl Acad Sci USA 91:3872-3876, 1994 Machida U, Kami M, Fukui T, et al: Real-time automated PCR for early diagnosis and monitoring of cytomegalovirus infection after bone marrow transplantation. J Clin Microbiol 38:2536-2542, 2000 Maeda Y, Teshima T, Yamada M, et al: Monitoring of human herpesviruses after allogeneic peripheral blood stem cell transplantation and bone marrow transplantation. Br J Haematol 105:295-302, 1999 Martin DF, Sierra-Madero J, Walmsley S, et al: A controlled trial of valganciclovir as induction therapy for cytomegalovirus retinitis. N Engl J Med 346:1119-1126, 2002 Mendez JC, Dockrell DH, Espy MJ, et al: Human betaherpesvirus interactions in solid organ transplant recipients. J Infect Dis 183:179-184, 2001 Meyers JD, Ljungman P, Fisher LD: Cytomegalovirus excretion as a predictor of cytomegalovirus disease after marrow transplantation: Importance of cytomegalovirus viremia. J Infect Dis 162:373-380, 1990 Meyers JD, Reed EC, Shepp DH, et al: Acyclovir for prevention of cytomegalovirus infection and disease after allogeneic marrow transplantation. N Engl J Med 318:70-75, 1988 Mirandola P, Secchiero P, Pierpaoli S, et al: Infection of CD34(⫹) hematopoietic progenitor cells by human herpesvirus 7 (HHV-7). Blood 96:126-131, 2000 Mori T, Okamoto S, Watanabe R, et al: Dose-adjusted preemptive therapy for cytomegalovirus disease based on realtime polymerase chain reaction after allogeneic hematopoietic stem cell transplantation. Bone Marrow Transplant 29: 777-782, 2002 Nguyen Q, Champlin R, Giralt S, et al: Late cytomegalovirus pneumonia in adult allogeneic blood and marrow transplant recipients. Clin Infect Dis 28:618-623, 1999 Nicholas J: Determination and analysis of the complete nucleotide sequence of human herpesvirus. J Virol 70:59755989, 1996 Osman HK, Peiris JS, Taylor CE, et al: “Cytomegalovirus disease” in renal allograft recipients: Is human herpesvirus 7 a co-factor for disease progression? J Med Virol 48:295301, 1996 Pescovitz MD, Rabkin J, Merion RM, et al: Valganciclovir results in improved oral absorption of ganciclovir in liver transplant recipients. Antimicrob Agents Chemother 44: 2811-2815, 2000 Prentice HG, Gluckman E, Powles RL, et al: Impact of long-term acyclovir on cytomegalovirus infection and survival after allogeneic bone marrow transplantation. Euro- 162 73. 74. 75. 76. 77. 78. 79. 80. 81. 82. 83. 84. 85. 86. 87. Clark, Emery, and Griffiths pean Acyclovir for CMV Prophylaxis Study Group. Lancet 343:749-753, 1994 Qamruddin AO, Oppenheim BA, Guiver M, et al: Screening for cytomegalovirus (CMV) infection in allogeneic bone marrow transplantation using a quantitative whole blood polymerase chain reaction (PCR) method: Analysis of potential risk factors for CMV infection. Bone Marrow Transplant 27:301-306, 2001 Reed EC, Shepp DH, Dandliker PS, et al: Ganciclovir treatment of cytomegalovirus infection of the gastrointestinal tract after marrow transplantation. Bone Marrow Transplant 3:199-206, 1988 Reusser P, Attenhofer R, Hebart H, et al: Cytomegalovirusspecific T-cell immunity in recipients of autologous peripheral blood stem cell or bone marrow transplants. Blood 89:3873-3879, 1997 Reusser P, Einsele H, Lee J, et al: Randomized multicenter trial of foscarnet versus ganciclovir for preemptive therapy of cytomegalovirus infection after allogeneic stem cell transplantation. Blood 99:1159-1164, 2002 Reymen D, Naesens L, Balzarini J, et al: Antiviral activity of selected acyclic nucleoside analogues against human herpesvirus 6. Antiviral Res 28:343-357, 1995 Roback JD: CMV and blood transfusions. Rev Med Virol 12:211-219, 2002 Rubin RH: The indirect effects of cytomegalovirus infection on the outcome of organ transplantation. JAMA 261:36073609, 1989 Santoro F, Kennedy PE, Locatelli G, et al: CD46 is a cellular receptor for human herpesvirus 6. Cell 99:817-827, 1999 Secchiero P, Zella D, Barabitskaja O, et al: Progressive and persistent downregulation of surface CXCR4 in CD4(⫹) T cells infected with human herpesvirus 7. Blood 92:45214528, 1998 Soderberg-Naucler C, Fish KN, Nelson JA: Reactivation of latent human cytomegalovirus by allogeneic stimulation of blood cells from healthy donors. Cell 91:119-126, 1997 Takahashi K, Sonoda S, Higashi K, et al: Predominant CD4 T-lymphocyte tropism of human herpesvirus 6-related virus. J Virol 63:3161-3163, 1989 Takahashi K, Suzuki M, Iwata Y, et al: Selective activity of various nucleoside and nucleotide analogues against herpesvirus 6 and 7. Antiviral Chem Chemother 8:24-31, 1997 Tanaka K, Kondo T, Torigoe S, et al: Human herpesvirus 7: Another causal agent for roseola (exanthem subitum). J Pediatr 125:1-5, 1994 Tanaka Y, Kanda Y, Kami M, et al: Monitoring cytomegalovirus infection by antigenemia assay and two distinct plasma real-time PCR methods after hematopoietic stem cell transplantation. Bone Marrow Transplant 30:315-319, 2002 Taylor-Wiedeman J, Sissons JG, Borysiewicz LK, et al: Monocytes are a major site of persistence of human cytomegalovirus in peripheral blood mononuclear cells. J Gen Virol 72:2059-2064, 1991 88. Tong CY, Bakran A, Williams H, et al: Association of human herpesvirus 7 with cytomegalovirus disease in renal transplant recipients. Transplantation 70:213-216, 2000 89. Torelli G, Barozzi P, Marasca R, et al: Targeted integration of human herpesvirus 6 in the p arm of chromosome 17 of human peripheral blood mononuclear cells in vivo. J Med Virol 46:178-188, 1995 90. Wainwright MS, Martin PL, Morse RP, et al: Human herpesvirus 6 limbic encephalitis after stem cell transplantation. Ann Neurol 50:612-619, 2001 91. Wang FZ, Dahl H, Linde A, et al: Lymphotropic herpesviruses in allogeneic bone marrow transplantation. Blood 88: 3615-3620, 1996 92. Wang FZ, Linde A, Hagglund H, et al: Human herpesvirus 6 DNA in cerebrospinal fluid specimens from allogeneic bone marrow transplant patients: Does it have clinical significance? Clin Infect Dis 28:562-568, 1999 93. Webster A, Blizzard B, Pillay D, et al: Value of routine surveillance cultures for detection of CMV pneumonitis following bone marrow transplantation. Bone Marrow Transplant 12:477-481, 1993 94. Wilborn F, Brinkmann V, Schmidt CA, et al: Herpesvirus type 6 in patients undergoing bone marrow transplantation: Serologic features and detection by polymerase chain reaction. Blood 83:3052-3058, 1994 95. Wills MR, Carmichael AJ, Mynard K, et al: The human cytotoxic T-lymphocyte (CTL) response to cytomegalovirus is dominated by structural protein pp65: Frequency, specificity, and T- cell receptor usage of pp65-specific CTL. J Virol 70:7569-7579, 1996 96. Winston DJ, Ho WG, Bartoni K, et al: Ganciclovir prophylaxis of cytomegalovirus infection and disease in allogeneic bone marrow transplant recipients. Results of a placebocontrolled, double-blind trial. Ann Intern Med 118:179-184, 1993 97. Yamanishi K, Okuno T, Shiraki K, et al: Identification of human herpesvirus-6 as a causal agent for exanthem subitum. Lancet 1:1065-1067, 1988 98. Yoshida M, Yamada M, Tsukazaki T, et al: Comparison of antiviral compounds against human herpesvirus 6 and 7. Antiviral Res 40:73-84, 1998 99. Yoshikawa T, Asano Y, Ihira M, et al: Human herpesvirus 6 viremia in bone marrow transplant recipients: clinical features and risk factors. J Infect Dis 185:847-853, 2002 100. Zerr DM, Gupta D, Huang ML, et al: Effect of antivirals on human herpesvirus 6 replication in hematopoietic stem cell transplant recipients. Clin Infect Dis 34:309-317, 2002 101. Zhang Y, de Bolle L, Aquaro S, et al: Productive infection of primary macrophages with human herpesvirus 7. J Virol 75:10511-10514, 2001 102. Zhang Y, Hatse S, De Clercq E, et al: CXC-chemokine receptor 4 is not a coreceptor for human herpesvirus 7 entry into CD4(⫹) T cells. J Virol 74:2011-2016, 2000