Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
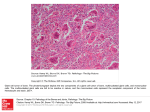
Giant Cell Lesions - A review Giant Cell Lesions - A review Introduction Giant cell lesions of bones represent a broad category of entities. These include, giant cell lesions of the bones, central and peripheral giant cell granulomas, aneurysmal bone cysts, brown tumors of hyperparathyroidism and cherubism. Introduction There is a longstanding controversy regarding the relationship between giant cell tumors of the axial skeleton and giant cell granulomas of the jaws. Controversies : Giant Cell Lesions Until the mid 1950’s giant cell tumors of the extragnathic skeleton were considered closely related to giant cell lesions which occurred in the jaws. Controversies : Jaffe’s recommendations In 1953, Jaffe separated the giant cell lesions occurring in the jaws from the giant cell tumors of the long bones, based on the differences in the clinical presentation, histopathology, radiography and treatment response between these two lesions. Controversies : Jaffe’s recommendations Jaffe called these giant cell lesions of the jaws as “giant cell reparative granulomas”. He indicated that the jaw lesions tend to occur in younger patients (10 to 25), where as giant cell tumors of the axial skeleton usually appeared after the age of 20. Controversies : Jaffe’s recommendations He suggested that giant cell tumors of long bones were far more aggressive, with higher rates of recurrence with potential to undergo malignant transformation. Controversies : Giant Cell Lesions In 1966, Waldron and Shafer argued that the “giant cell tumors” of the long bones and “giant cell reparative granulomas” of the jaws are one and the same entity but may differ in presentation and histology. Controversies : Giant Cell Lesions Currently there are two schools of thought regarding the existence of giant cell tumors in the facial skeleton. Controversies : Giant Cell Lesions Some like Jaffe, firmly believe that true giant cell tumors either do not exist or occur very rarely in the maxillofacial region. However other pathologists and clinicians remain convinced that giant cell tumors do occur within the jaws. Controversies : Giant Cell Lesions Abrams and shear in 1974, consolidated these two positions, and suggested that certain jaw lesions may be true giant cell tumors and certain giant cell lesions outside the jaws maybe giant cell granulomas. Giant cell lesions of the long bones Giant cell lesions of the long bones: Clinical features The females have a slight predilection. The peak incidence is in the third decade with the tumor occurring in over 80% of cases after the age of 20. Giant cell lesions of the long bones: Clinical features Most long bone lesions are located at the epiphyseal region of the bone. Most of these lesions appear as a solitary lesion, and multifocal disease is very rare. Patients present with pain, localized swelling and tenderness at the site of the affected bone. Giant cell lesions of the long bones: Clinical features These lesions present with a wide range of aggressiveness, ranging from the more conventional giant cell tumor to true malignancies with a high potential for recurrence and metastasis. Incidence of truly malignant giant lesion ranges from 3% to 30%.(Franklin et al). Giant cell lesions of the long bones: Clinical features Giant cell lesions of the long bones: Histopathology There are large number of multinucleated giant cells of varying density separated by stromal cells. This type of histologic pattern is similar in many other bone lesions like (browns tumor, non ossifying fibroma, Aneurysmal bone cyst, e.t.c.,) Giant cell lesions of the long bones Therefore, the clinician must also correlate the histological findings with the clinical and radiographic presentation to make the correct diagnosis. Giant cell lesions of the long bones: Treatment The surgical treatment is either curettage or resection and is performed based on the type and extension of the tumor which affects the bone. Central Giant cell lesions of the Jaws Central Giant cell lesions of the Jaws The literature regarding giant cell lesions of the jaw is confusing because some authors have included both central and peripheral lesions in their series. Central Giant cell lesions of the Jaws It is now well recognized that the peripheral giant cell lesion differs in clinical presentation and behavior from the central lesion. Central Giant cell lesions of the Jaws: Clinical features These lesions occurs between the age of 2 to 81 years, but the average age is within the second decade of life. Sex: 2:1 female predilection. The mandible is clearly the preferred site. Central Giant cell lesions of the Jaws: Clinical features These lesions mainly occur in the anterior portion of the maxilla and mandible. Posterior maxilla or mandible is rarely involved. Central Giant cell lesions of the Jaws: Clinical features Multiple central giant cell lesions in a single patient are exceedingly rare. A painless local swelling is the most commonest presenting symptom although some patients may have pain or anesthesia. Central Giant cell lesions of the Jaws: Radiographic features The most characteristic X-ray feature is a radiolucency within bone and can either have an multilocular or unilocular configuration. Central Giant cell lesions of the Jaws: Radiographic features Thin, wispy septa. Resorption of teeth very common. “Salt & Pepper “ calcification can be seen. Central Giant cell lesions of the Jaws: Radiographic features V-shaped bony ridges separating the locules. Central Giant cell lesions of the Jaws: Histopathology Histologically a central giant cell lesion is characterized by numerous multinucleated giant cells within a loose fibrous connective tissue Stroma. Central Giant cell lesions of the Jaws: Clinical behaviour Small, slow growing, asymptomatic responds well to curettage. mass However, the large and aggressive mass produces pain and recurs frequently, especially in younger patients. True malignant giant cell tumors of the jaw may produce distant and local metastases. Central Giant cell lesions of the Jaws: Clinical behaviour There are no definitive histological parameter to predict the clinical behavior. Therefore, the clinician must use his judgment, appropriate treatment strategies and long-term follow-up in order to properly manage these lesions. Central Giant cell lesions of the Jaws: Treatment Surgical curettage is the most commonest procedure. Large aggressive lesions of the maxilla and mandible may require an en-bloc resection. Central Giant cell lesions of the Jaws: Treatment In some lesions both the overlying mucosa and periosteum must be removed. Non surgical modalities of treatment include systemic calcitionin administration, antiangiogenic therapy with interferon, and intralesional corticosteroids. Central Giant cell lesions of the Jaws: Treatment Harris (1992) reported regression of these masses with systemic calcitonin therapy. Two of the four patients in his study exhibited complete regression, while the other required additional surgery to eradicate the lesion. Central Giant cell lesions of the Jaws: Treatment Lange et. al. (1999) had obtained significant regression of the lesions(central giant cell granuloma) in all his four patients following cacitonin treatment. The efficacy of intra-lesional steroids use in the treatment of giant cell lesions remains to be proven. Peripheral Giant cell lesions of the Jaws Peripheral Giant cell lesions of the Jaws In the past these lesions were referred to as “giant cell epulis”. Peripheral Giant cell lesions of the Jaws : Etiology The exact etiology for these lesions is not known. However, it is believed that these lesions are reactive in nature and develop as a result of localized trauma or irritation ( e.g., tooth extraction, calculus deposits, ill fitting dentures and poor restorations). Peripheral Giant cell lesions of the Jaws: Clinical features Although the peripheral giant cell lesion occurs at a much higher frequency than the central type, it remains relatively uncommon (accounting for only 0.3% to 0.5% of all oral biopsies). They are usually seen in patient’s between the third and fifth decades of life. Peripheral Giant cell lesions of the Jaws: Clinical features There is a significant female predilection, suggesting the role of hormone levels in the development of these lesions. Most lesions occur on the gingiva or the edentulous alveolar ridge in either a posterior or anterior portion on the jaw. The mandible is affected slightly more than the maxilla . Peripheral Giant cell lesions of the Jaws: Clinical features The lesions can be either pedunculated or sessile. They rarely exceed 2 cm in size and typically present with a bluish – purple color. Peripheral Giant cell lesions of the Jaws: Radiographic features As most of these lesions are usually manifestations within the gingiva, no radiological finding is reported other than an occasional ovoid surface erosion of the underlying bone. Peripheral Giant cell lesions of the Jaws: Histopathology The histological features demonstrate the characteristic giant cells in a fibrous connective tissue stroma which is covered by a surface epithelium. Peripheral Giant cell lesions of the Jaws: Treatment The treatment of choice is a surgical excision. In lesions involving the gingival mucosa around the teeth, care must be taken to debride the surrounding teeth and surgical site, so as to remove all sources of possible irritation. Extraction is no longer recommended. Peripheral Giant cell lesions of the Jaws: Recurrence Recurrence rate ranges between 5% and 10%. These recurrences are most often due to failure in removing the entire lesion or the source of any local irritation. Brown’s Tumor Of Hyperparathyroidism Hyperparathyroidism (Brown’s tumor) Brown’s tumor of hyperparathyroidism is clinically, histologically and radiographically indistinguishable from other types of giant cell lesions. Hyperparathyroidism: Types Primary hyperparathyroidism is caused by an overproduction of parathormone by the parathyroid gland affected by adenoma or hyperplasia. Secondary hyperparathyroidism also results in increased production of parathormone and is found to occur in various disease states where there is resistance to the metabolic actions of the parathormone. Hyperparathyroidism: Clinical features The typical hyperparathyroidism patient presents without any significant symptoms. Some patients present with renal calculi or some skeletal manifestations. The disease is easily diagnosed by measuring the patient’s serum calcium and parathormone levels. Hyperparathyroidism: Radiographic features Hyperparathyroidism: Treatment Treatment is directed towards normalizing calcium/phosphate/parathyroid homeostasis. If a parathyroid adenoma is the cause of elevated hormone level, surgical excision of this tumor produces a complete recovery. In secondary hyperparathyroidism, the treatment efforts is on correcting the underlying metabolic disturbance. Aneurysmal bone cyst Aneurysmal bone cyst In 1942, Jaffe and Lichenstein, introduced the term aneurysmal bone cyst. Other names for this lesion include, aneurysmal giant cell tumor, subperiosteal giant cell tumor e.t.c. Aneurysmal bone cyst : Etiology There is controversy regarding the etiology of this lesion. For the moment there are no strong evidences to prove that these lesions develop primarily, or to say that they develop secondarily due to another underlying disease process. Aneurysmal bone cyst: Etiology Lichenstein indicates that this lesion results from a locallised vascular disturbance such as a venous thrombosis or arteriovenous malformation. Aneurysmal bone cyst: Etiology Others believe that this lesion can either be a separate reactive process, arising from another primary bone lesion such as fibrous dyplasia, central giant cell granuloma, or pagets disease. Aneurysmal bone cyst : Clinical features This lesion occurs in younger patients usually below 20 years of age. The mandible appears to be more commonly affected than the maxilla. Aneurysmal bone cyst: Clinical features The posterior molar-bearing segments of the maxilla and mandible seem to be more commonly affected region. Clinically these lesions are characterized by a non-pulsatile swelling of variable duration. Aneurysmal bone cyst: Clinical features 50% of patients present with pain in the affected region. Tooth displacement and external root resorption may also be seen. There is a slight female predilection in both the long bones and jaw lesions. Aneurysmal bone cyst: Radiographic features This lesion is classically described as an expanded, cystically transformed, eccentric ballooning of the bone. Fine bony trabeculations in the lesion give a “soap bubble appearance”. Aneurysmal bone cyst: Histopathology Microscopically this lesion is not a true cyst, as it does not have a epithelial lining, and is characterized by large, blood filled cavities contained within a thin, bony framework. The histologic pattern of the stroma between the sinusoids is very similar to that of other giant cell lesions. Aneurysmal bone cyst: Recurrence The recurrence rate of these lesions in th long bones is about 21% to 40%, and in the jaws is about 19%. Aneurysmal bone cyst: Treatment Despite the recurrence rates, a thorough curettage is the most commonest treatment modality for this lesion. Aneurysmal bone cyst: Treatment In some lesions with associated vascular malformations, preoperative super-selective embolization of the feeding vessels to the lesion is mandatory before surgery. Following embolization either curettage or en-bloc resection can be performed. Cherubism Cherubism Jones reported on the clinical entity known as Cherubism in the year 1933. He coined the term cherubism due to these patients resemblance to the cherubs portrayed in renaissance art. Cherubism: Clinical features Classic cherubic appearance is due to a characteristic bilateral enlargement of the maxillae, causing retraction of the lower eyelids and exposure of the sclera, giving an “eyes raised to heaven” appearance. Cherubism: Clinical features In contrast to other giant cell lesions, cherubism has a hereditary predilection which helps to differentiate it from other similar entities. Cherubism: Clinical features Cherubism is an autosomal dominant disorder with variable expressivity. Cherubism may also result from a spontaneous mutation with no apparent familial involvement. The disease occurs with a 2 : 1 male preponderance. Cherubism: Clinical features Cherubism is not found to occur very commonly. Typically, it appears in young children before the age of five, most commonly prior to the second birthday. Cherubism: Clinical features The lesion occurs almost exclusively in the mandible and maxilla, but in some cases have occurred in extragnathic sites. They are most often seen in the mandible, with the ascending rami and the retromolar area being most commonly affected. Cherubism: Clinical features In rare cases the mandibular condyles can also be involved. The lesions are classically bilateral, although unilateral involvement has been reported. Cherubism: Clinical features Maxilla involvement is less frequent. However,when it occurs it involves the maxillary tuberosity region. These lesions may also involve the orbital floor and anterior maxilla. Cherubism: Grading The diverse clinical presentation has prompted some clinicians to adopt a grading system which categorizes these lesions according to extent of involvement. Cherubism: Grading Grade 1 : Involvement of both mandibular ascending rami. Grade 2 : Involvement of both rami and both maxillary tuberosities. Grade 3 : Diffuse bilateral involvement of the entire maxilla and mandible with sparing of the condyle. Grade 4 : Lesions with the features of grade 3 but with orbital floor involvement. Cherubism: Clinical behavior These lesions present as a progressively enlarging, painless swelling with marked bony expansion. The dentition in the affected region is often displaced. Cherubism: Clinical behavior The deciduous teeth are usually exfoliated by the age of three and the permanent tooth follicles are displaced, resulting in delayed eruption, multiple impacted teeth or both. Cherubism: Clinical behavior Uniform, bilateral mandibular involvement can commonly result in gross malocclusion in addition to facial disfigurement. In the most severe cases, speech, swallowing, and respiration can be affected. Cherubism: Radiographic features The typical radiographic presentation is a diffuse osteolytic radiolucent process with diffuse cortical expansion and thinning of the involved bone. In the tooth-bearing segments of the mandible, the teeth are described as “floating in cyst-like spaces”. Cherubism: Histopathology The histologic profile of cherubism is similar to other giant cell lesions and shows numerous multinucleated giant cells are contained within highly vascular fibrous stroma. Cherubism: Treatment The prognosis for cherubism remains good, given the fact that these lesions usually are self-limiting and tend to regress with time. The lesions become static as a patient approaches puberty and thereafter begins to slowly regress. Cherubism: Treatment Most cases undergo a surgical procedure for cosmetic or functional needs. Curettage and re-contouring is advocated by some to arrest the disease process and stimulate bone deposition. Few others recommend no treatment other than following the patient. Giant Cell Lesions: Discussion Miles et al (1991) provided the following comments regarding their understanding of giant cell lesions: A central giant cell lesion may consists of several related reactive lesions which result from trauma or vascular insult which produces intramedullary bleeding. Giant Cell Lesions: Discussion - Miles et al (1991) If the blood supply is cut off completely, no giant cell reaction occurs and the traumatic bone cyst occurs. Conversely, if the blood supply is maintained fully, an A-V malformation develops. However, if the blood supply is maintained only partially, then an aneurysmal bone cyst or central giant cell lesion could result. Thank you