Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Low-carbohydrate diet wikipedia , lookup
Ketogenic diet wikipedia , lookup
Hadrosaur diet wikipedia , lookup
Food choice wikipedia , lookup
Coeliac disease wikipedia , lookup
Human nutrition wikipedia , lookup
Diet-induced obesity model wikipedia , lookup
Raw feeding wikipedia , lookup
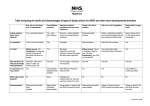
Medina Blanchet, Dietetic Intern Utah State University Autism first classified in 1943 by Dr. Leo Kanner of Johns Hopkins. 1964 - Dr. Bernard Rimland of the Autism Research Institute helped dispel “refrigerator mother” theory. 1980 - became an official diagnosis, separate from other conditions (1). No clear etiology or cure. There is a genetic link. Some children can appear to be developing normally until one or two years of age, with a vocabulary of dozens of words, then within a matter of weeks lose the ability to communicate and become withdrawn. During the 1990s, it was speculated that the thimerosol in childhood vaccinations may have caused autism. Thimerosol has been used since the 1930s. Numerous studies concluded that thimerosol did not cause autism. However, in 2001 the FDA decided to discontinue using it in routine childhood vaccinations. •Precaution •Parents were refusing to immunize their children. Prevalence reports show that this did not slow down the rise in the number of cases of autism (2). Fall under the general category of Pervasive Developmental Disorder (PDD). Autistic disorder Asperger syndrome and Pervasive developmental disorder – not otherwise specified (PDD-NOS) The American Psychiatric Association’s DSMIV specifies that child must have at least six symptoms (from table) by age three for autistic disorder. Children with Asperger syndrome are often referred to as “high functioning”. No history of language delay Normal IQ The diagnosis for Asperger Syndrome is up to five symptoms. PDD-NOS includes individuals with symptoms who do not meet the criteria for the other disorders and onset may occur after the age of three (3). DSM-IV List of Symptoms Social Interaction (minimum 2) Marked impairment in the use of multiple nonverbal behaviors Failure to develop appropriate peer relationships (prefers to be alone, little or no eye contact) Lack of spontaneous seeking to share enjoyment, interests or achievements with others Lack of social or emotional reciprocity (not affectionate) Communication (minimum 1) Delay or lack of development of spoken language Marked impairment in ability to initiate or sustain conversation Repetitive use of language, such as echolalia (repeating or phrases) or pronoun reversal Lack of varied, spontaneous pretend or social imitative play Restricted repetitive, stereotyped behaviors, interests, activities (minimum 1) Preoccupation with restricted patterns of interest with abnormal intensity or focus (sustained odd play) Apparently inflexible adherence to specific nonfunctional routines or rituals (resists change) Repetitive motor mannerisms (flapping, walking on toes) Unusual interest in sensory things (lines things up, twirls or flick objects, etc.) Delays or abnormal functioning after the age of three (minimum 1) Social interaction Language as used in social communication Symbolic or imaginative play According to the CDC, ASDs occur in all racial, ethnic and socioeconomic groups. 4x more likely to occur in boys than girls. The average prevalence in the United States in 2009 was one in every 110 eight-year-old children. (4) The prevalence by state varies dramatically. (See figure 1) (15). Even more dramatic is the rate at which ASD is increasing each year. Over the past decade it has increased over 500%. (See figure 2) (16). This rapid rise is an area of controversy. Some experts believe it is due to an increase in the rate of reporting officially diagnosed cases. Sharon Lemons, RD is an officer for the Dietetics in Development and Psychiatric Disorders practice group with the American Dietetics Association. She also has two sons with autism. She states that early on parents did not want their children diagnosed with autism because of the negative stigma of “refrigerator mother” attached to it. As the diagnosis evolved, the stigma faded and families were eligible for various services. Today, even very mild cases are being diagnosed, which she believes could account for the rapid rise in reported cases (1). Most likely, it is a combination of better diagnostics and an increase in the incidence of children being born with the disorder. Acknowledges that some families have found that dietary intervention helps reduce the symptoms of autism. Until recently there has been no evidence from controlled scientific studies to prove that to be true. It is recommended that families wishing to pursue dietary intervention do so with the guidance of a nutrition professional (5). GI disorders in ASD include GERD, abdominal bloating, enzyme deficiencies, constipation, diarrhea and inflammation of the GI tract and altered intestinal permeability. Non – GI issues include behavioral problems and sleep disturbances. Studies indicate these issues tend to be ↑ in ASD children than in healthy age-matched controls. ASD children have a limited ability to communicate. Very challenging to identify the source or location of pain and discomfort. May manifest in behavior problems and sleep disturbances. Inadequate sleep can further aggravate behavior problems. There is not sufficient scientific evidence to identify a unique GI pathophysiology specific to ASDs (6). Regardless, the GI disorders listed above can cause maldigestion and malabsorption, which contributes to nutrient deficiencies and food sensitivities. Occurs when the gut becomes inflamed. Tight junctions holding the endothelial wall (gut lining) together start to loosen, causing increased permeability. Allows foods to pass into the bloodstream from the intestine before the food has been completely broken down. Partially digested food is not recognized by the immune system. The immune system sends out “the troops” known as antibodies to attack the unknown food. Anytime the immune system is activated, it causes inflammation throughout the entire body. Fatigue Headaches “Foggy brain” Rashes Congestion Sleep disturbances Achy joints Asthma Ear infections, etc Food that would normally have no ill effects on a person with a healthy gut can cause a whole host of symptoms when the food is not properly digested and absorbed. (See figure 3) Broad category that includes food allergies and food intolerances/sensitivities. Food allergies are IgE mediated hypersensitive reactions that occur within minutes of contact with an allergen. Once an IgE allergy has developed, it is often a life-long condition. An example would be developing anaphylaxis after eating peanuts. Some hypersensitive reactions can be lifethreatening. Food intolerances are slow-reacting allergies and are rarely life-threatening. These sensitivities often resolve once the gut heals. Some laboratories use IgG antibody tests to determine food intolerances. Many in the allopathic medical community do not consider these tests to be valid in the clinical realm, but are useful in research (7). The natural medicine community is more likely to use this form of testing. IgG antibodies indicate that there has been exposure to food. They react significantly slower than IgE antibodies, often taking days to manifest symptoms (7). This makes it very difficult for a person to recognize a food intolerance/sensitivity. Research has shown that children with ASD have higher amount of IgG antibodies to gliadin (part of gluten) than those of the control group of healthy children of the same age (8). Anytime the immune system is activated, inflammation results, regardless of the types of antibodies involved. A clinical trial done in the late 90s studied 149 autistic children. As much as 87% of the children had high titer IgG antibodies to gliadin. After being on a gluten-free/casein-free (GF/CF) diet for 3 months 81% of the children showed improvements. This study included both physiological and behavioral components. The weakness of the study was that it was not blinded. Behavioral results relied heavily on parents and teachers who knew the children were on a GF/CF diet (9). An area of controversy with dietary interventions in ASDs is the “parental placebo effect”. Some researchers believe that the extra attention given to the children during a study may have more influence on behavior than the dietary intervention (10). “epi” means above The study of how a person’s environment can turn on or off genes. At conception a person receives a genetic blueprint, which cannot be altered. Many factors influence whether a gene is expressed or not, including development in utero, early childhood development, environmental pollutants, drugs, diet and aging. If a person’s parents and grandparents both have heart disease, there is a strong likelihood that the person will inherit the gene for heart disease. This does not automatically mean that he/she will develop the disease. Many factors such as smoking, diet and exercise will greatly influence the expression of that gene. One of the ways the cells control which genetic information they will use is by methylation. Methyl groups are commonly found in the diet. A methyl group is a carbon molecule and two hydrogen molecules. When this chemical modification process goes haywire, hypermethylation can cause abnormal expression or repression of genes. (see figure 4) (11). The National Institute of Mental Health announced in its Science News (December 2009) that research has identified a silenced gene which contributes to aberrant social behavior in autism (11). The study used postmortem brain tissue samples from the temporal cortex of eight autistic individuals. Eight control samples were selected to match patients on gender and age. There was significantly more hypermethylation of the oxytocin receptor in the autistic samples. This genomic deletion silences that receptor. Not necessary to take brain tissue samples to determine excess methylation of the oxytocin receptor. Methylation status can also be determined from blood samples. Has the potential to be used as a biomarker for autism. Epigenomic profiles undergo reprogramming during very early gestation (12). Since early detection and intervention are crucial, blood tests done early in a child’s life, or even at birth, may prove to have significantly more impact on outcome. One of the most popular dietary interventions for ASD children is a gluten-free/casein-free diet. Gluten is a protein found in wheat, barley and rye. It is a combination of two proteins – gliadin and glutenin. Gluten compromises 80% of the protein in wheat. It provides elasticity, which makes wheat flour the best grain for making bread. Casein is a protein found in milk products. Proteins are large, complex molecules. Gluten and casein seem to be particularly hard to digest for many individuals. Instead of being broken down into individual amino acids, they are partially broken down into peptides (several amino acids chained together). Improperly digested and absorbed gluten/gliadin and casein peptides can have an opiod-type effect on the nervous system, interfering with neurotransmission. This is thought to contribute to behavior problems in individuals with ASD. These dietary peptides show up in the urine in abnormally high amounts in autistic children (8). Clinical trials restricting gluten and casein are difficult to conduct due to the nature of ASD (behaviors causing dietary challenges) dietary restriction of the study Of major concern are nutrient deficiencies as the standard American diet consists of many foods prepared with wheat products. In Asian countries this is less of an issue as their diets are mainly rice and vegetables. In 2010, a two-staged randomized controlled trial out of Norway concluded that a GF/CF diet significantly improved hyperactivity and attention deficit in children with ASD. 72 Danish children were tested at baseline, 8 mo., 12 mo. and 24 mo. Children were randomly selected to be in the diet and non-diet groups. Due to improvements in the diet group that exceeded the researchers’ expectations, the non-diet group was reassigned to the diet group at 12 mo. The most dramatic results occurred in the first 8 mo of the diet intervention. All study members, except the nutritionists and the parents were blinded. A weakness of the study was that they did not have a placebo group (13). A smaller study done in Norway in 2002 looked at the effects of dietary intervention in autistic children with high urinary peptides. These peptides originate as dietary gluten, gliadin and casein. Children were randomized into the GF/CF diet or the control group. The project leaders were blinded. The study lasted for one year. Results indicated that the diet group had significant improvements in attention, social skills and communication (14). A weakness of this study is that it only involved a total of 20 children. In both of the Norwegian studies researchers concluded that if hyperactivity and/or attention deficit were minimized, capability to learn would improve. Examples of other diseases/conditions that require dietary intervention: Disease/Condition Dietary Intervention Cardiovascular disease Low saturated fat, low salt (TLC diet or DASH diet) Kidney disease Restrictions on protein, salt, potassium and phosphorus Cystic Fibrosis Type 2 diabetes Increased fat, sodium, energy and extra digestive enzymes Low glycemic diet (45-60 carbs per meal) PKU (Phenylketonuria) Restrict phenylalanine (amino acid) Celiac Sprue No gluten (found in the grains wheat, barley and rye) In some disease states, dietary intervention or medical nutrition therapy (MNT) can reduce the incidence of complications, or slow the rate of advancement. Example - cardiovascular disease. Severe complications or even death can result without dietary intervention Example – PKU A PKU diet is considerably more restrictive than a GF/CF diet as phenylalanine is found in almost all foods. Newborn babies are routinely tested for PKU, which is an inborn error of metabolism. Early diet intervention can significantly reduce brain damage. As researchers inch closer to finding the cause of ASDs, it is apparent that something in the diet may be a contributing factor to improper gene expression via hypermethylation. Further research is needed to determine specific nutrients (or lack of nutrients), chemicals or metabolic pathways that are responsible for this aberration. Until the etiology is determined, early detection and intervention can provide significant reduction in the progression of the disorder. Now doctors depend on developmental signs to make a diagnosis, making it very difficult to do so before the age of one. Hopefully soon, blood tests will be available to detect abnormalities much earlier. A component of many GI disorders, especially leaky gut. When offending foods are eliminated, inflammation subsides and the digestive tract heals. A healthy digestive tract digests and absorbs nutrients as they were intended to be. The immune system recognizes the “food” as safe. This reduces systemic inflammation and resolves or greatly reduces non-GI symptoms. Diet intervention or MNT is commonly used in many disease states. The success of the outcome is mostly dependent on adherence to the diet. Guidance from wellqualified nutritionists can be very helpful as families implement dietary interventions. A GF/CF diet can reduce some of the signs and symptoms associated with ASDs. Gluten and casein are not found in vegetables, fruits, meats, eggs, legumes, nuts, seeds and all other grains, except wheat, barley and rye. There can be small amounts of gluten in oats, mainly due to cross-contamination. It is possible to have a well-balanced GF/CF diet. Widespread use of flour in the standard American diet - incorporating this diet can be challenging. The most likely complication from strict dietary interventions may be nutrient deficiencies. Those may be remedied with appropriate and consistent nutritional supplementation. The ScanBrit study of 72 Danish children mentioned earlier reported “no significant adverse effects for any participant on [GF/CF] diet intervention.” (13). Families must decide for themselves if the strictness of the intervention is worth the reduction of the adverse manifestations of ASDs. Peregrin T. Registered dietitians’ insights in treating autistic children. J Am Diet Assoc. 2007; 107:727730. Centers for Disease Control and Prevention. Thimerosal. February 2010. Available at http://www.cdc.gov/vaccinesafety/Concerns/thimerosal/. Accessed September 9, 2010. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders DSM-IV-TR. 4th Edition. Arlington, VA: American Psychiatric Publishing, Inc., (June 2000). Centers for Disease Control and Prevention. Autism and Family Health. Available at http://www.cdc.gov/genomics/resources/diseases/autism.htm. Accessed September 1, 2010. Marcason W. What is the current status of research concerning use of a gluten-free, casein-free diet for children diagnosed with autism? J Am Diet Assn. 2009; 109: 572 Buie T, Campbell D, Fuchs G, Furuta G, Levy J, VandeWater J, Whitaker A, Atkins D, Bauman M, Beaudet A, Carr E, Gershon M, Hyman S, Jirapinyo P, Jyonouchi H, Kooros K, Kushak R, Levitt P, Levy S, Lewis J, Murray K, Natowicz N, Sabra A, Wershil B, Weston S, Zeltzer L, Winter H. Evaluation, diagnosis, and treatment of gastrointestinal disorders in individuals with ASDs: A concensus report. Pediatrics. 2010; 125:S1-S18. Mahan L, Escott-Stump S. Krause’s Food & Nutrition Therapy. 12th Edition. Philadelphia, PA: Saunders Elsevier, (2008). pp. 740-753. Vojdani A, O’Bryan T, Green JA, McCandless J, Woeller K.N, Vojdanis E, Nourian A.A, Cooper E.L. Immune Response to Dietary Proteins, Gliadin and Cerebellar Peptides in Children with Autism. Nutritional Neuroscience. 2004; 7:151-161. Cade R, Privette R.M., Fregly M, Rowland N, Sun Z, Sele V, et al. Autism and schizophrenia: Intestinal disorders. Nutritional Neuroscience. 1999; 2:57-72. Cormier E, Harrison-Elder J. Diet and child behavior problems: fact or fiction? Pediatric Nursing. March-April 2007; 33:138-143. The National Institute of Mental Health. Silenced Gene for Social Behavior Found in Autism. December 3, 2009. Available at http://www.nimh.nih.gov/science-news/2009/silenced-gene-for-social-behavior-found-in-autism.shtml. Accessed September 2, 2010. Gregory S, Connelly J, Towers A, Johnson J, Biscocho D, Markunas C, Lintas C, Abramson R, Wright H, Ellis P, Langford C, Worley G, Delong G, Murphy S, Cuccaro M, Persico A, Pericak-Vance M. Genomic and epigenetic evidence for oxytocin receptor deficiency in autism. BMC Medicine 2009; 7: 62. Whiteley P, Haracopos D, Knivsberg A, Reichelt K, Parlar, S, Jacobsen J, Seim A, Pedersen L, Schondel M, Sattock P. The ScanBrit randomized, controlled, single-blind study of a gluten- and casein-free dietary intervention for children with autism spectrum disorders. Nutritional Neuroscience. 2010; 13:87-100. Knivsberg A, Reichelt K, Hoien T, Nodland M. A randomized, controlled study of dietary intervention in autistic syndromes. Nutritional Neuroscience. 2002; 5: 251-261. Thoughtful House Center for Children. Autism State Rankings Prevalence. 2010. http://www.thoughtfulhouse.org/tech-labs/disabilities/autism-state-rankings-prevalence.php Accessed September 1, 2010. Thoughful House Center for Children. Cumulative Growth of Number of Cases. 2010. Available at http://www.thoughtfulhouse.org/tech-labs/disabilities/autism.php?s=US. Accessed September 1, 2010. Lupus Treatment.org. Food Allergy and Leaky Gut Inflammaton. July 29,2009. Available at http://www.lupustreatment.org. Accessed September 4, 2010.