Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
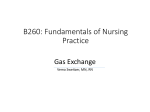
Tracheostomy Care and Suctioning Manual © 2009 Breath of Life Home Medical Equipment and Respiratory Services Parts of a Tracheostomy Tube: • Outer Cannula - The outer cannula is the main body of the tracheostomy tube. It is held in place with a trach tube holder that fits around the patients neck. Some trach tubes have a cuff on the end of them. This cuff is an inflatable balloon that seals against the tracheal wall when inflated. It helps to protect the airway from aspiration of oral secretions and prevents air from escaping through the mouth. Some patients do not require a cuff such as a patient who is not on a ventilator, patients who do not have swallowing issues and pediatric patients. Some outer cannulas have holes called fenestrations that allow airflow to escape and allow the patient to speak. • Inner Cannula – Some trach tubes have inner cannulas. The inner cannula fits inside the outer cannula. It is important to remove the inner canula and clean it to prevent mucus plugging and build up. The inner cannula locks into place to avoid removal. • Obturator - The obturator is used to help make insertion of the trach tube easier. The obturator has a round tip that sticks out of the end of the outer cannula. This protects the trachea from any damage as the trach tube is inserted into the airway. This must be removed as soon as the trach tube is inserted as it occludes the airway while in place. NOTE: Patients can NOT breathe while this is in place How to Deflate and Inflate the Cuff Minimal leak technique is used to limit the amount of air that is put in the cuff that sits against the tracheal wall. Once the cuff is inflated, withdraw a small amount of air until you hear a slight leak at the end of inspiration. The inflated cuff seals the airway so that the patient can get the prescribed tidal volume that the physician has ordered. It is important to monitor this pressure so that damage to the tracheal wall does not occur. Another technique used to check cuff pressure is to use the minimal occluding volume. To do this procedure you put enough air in the cuff so that no leak is heard during inspiration. If you are using a pressure manometer it is preferred to have a cuff pressure reading of 25 cm H2O. Tracheosotmy Care It is important to keep the stoma and the trach tube clean. To do this trach care should be done at least twice a day and as needed. This includes cleaning the inner cannula, around the trach tube and the stoma. Cleaning the trach tube is done by using clean technique. The trach tube should be changed once a month. This is always done using a sterile technique. Good hand washing technique is vital to prevent infections. You must always use gloves when dealing with trach tubes. Tracheostomy Dressings: Trach tubes have a dressing around them that is used to protect the skin. The dressing should be changed when doing trach care or as needed. Trach dressings should not be moist or soiled. Tracheostomy Tube Ties: Tracheostomy tube ties are used to keep the trach tube in place to prevent accidental removal and to minimize movement of the trach tube. The ties should be changed daily with trach care or as needed. They should not be moist or soiled. Equipment Needed: Suction equipment Dale trach holder Procedure: Wash your hands Take the old holder off while holding the tube in place . Insert the end of the new holder into the slit on the side of the outer flange of the trach tube. Place the other end in the other side. Pull the sides so that they are tightly secure making sure to get two fingers under the holder. Wash your hands Cleaning the Inner Cannula: It is very important to keep the inner cannula of the trach tube clean and free from dried secretions. Dried secretions can occlude the trach tube and make it difficult for the patient to breathe. To remove the inner cannula, turn the inner cannula counter clockwise, then remove it. If the inner cannula has flange clips, pinch them and then remove the inner cannula. The inner cannula should be changed at least daily or as needed. It should be replaced with a clean new inner cannula or should be washed using sterile technique if using a non-disposable inner cannula. Tracheostomy Care: It is important to use sterile technique to minimize infection. Equipment Needed: • • • • • • • Sterile tracheostomy cleaning kit which includes Sterile tray Sterile field Sterile brush Sterile 4x4 gauze pads Sterile pipe cleaners Sterile gloves Sterile dressing pads Sterile trach ties Clean inner cannula 3% Hydrogen peroxide Sterile water Sterile suction catheter Suction machine Ambu bag Procedure: 1. Wash your hands 2. Open the cleaning kit and spread the sterile field out on to the work area. 3. Pour the hydrogen peroxide in one tray and the sterile water in the other side 4. Place the sterile glove on your dominant hand 5. Remove the items from the kit with the sterile gloved hand and put them on the sterile field 6. Suction the patient 7. Disconnect the patient from the vent with your non-sterile hand. 8. Unlock and remove the inner cannula with your non-sterile hand and place it in the tray with the hydrogen peroxide to soak. If using a non-disposable inner cannula. 9. Insert a clean inner cannula into the trach tube and reconnect the patient to the vent. 10.Use the sterile brush to clean the inner cannula with 11.Rinse the inner cannula with the sterile water 12.Use the sterile 4x4 to dry the inner cannula. 13.Store the clean inner cannula in a covered container 14.Suction the patient as needed 15.Remove the soiled trach dressing using the non-sterile hand 16.Clean the skin with a gauze pad moistened in the sterile water. Dry the skin with a sterile 4x4. 17.Apply a clean trach dressing and change the tube holder if needed. 18.Throw away all of the disposable supplies 19.Wash your hands Tracheostomy Tube Change: Tracheostomy tubes need to be changed monthly to decrease the chance of infection. You should always have a back up trach tube. One of the same size and one a size smaller. Do Not change the trach tube unless you have gone through proper training. It is very important to use sterile technique during the trach change procedure. Equipment Needed: • • • • • • • • • • • Sterile tracheostomy tube Sterile gloves Sterile water soluble lubricant Sterile towel Suction equipment 10 cc syringe Ambu bag Sterile 4x4 gauze Trach tube holder Trach dressing Hydrogen Peroxide Procedure: 1. Wash your hands 2. Open the sterile towel for the sterile field 3. Open the sterile supplies and place them on the sterile field 4. Put the sterile glove on your dominant hand 5. Make sure the new trach tubes cuff is fully deflated. Be sure to not contaminate the tube by touching anything with it. 6. Remove the inner cannula and replace it with the obturator 7. Check the cuff by inserting 10 cc of air in the cuff and check holes. 8. Lubricate the tip of the tube with a water soluble lubricant. Do not use a petroleum based product. 9. Suction the patient if needed 10.If the patient has a cuff, deflate the cuff by pulling out all of the air out of the cuff. 11.Remove the trach dressing and the trach tube holder 12.Clean the skin as needed with a sterile 4x4 and sterile water 13.Disconnect the patient from the ventilator. You may need for someone to ventilate the patient with the ambu bag while you change out the trach 14.Remove the trach tube using a forward, downward motion. 15.With your sterile hand, gently insert the new trach tube within 30 minutes with the obturator in place. 16.Immediately remove the obturator 17.Insert the inner cannula into the trach tube 18.Inflate the cuff using minimal leak technique or using a Cuff manometer. 19. Check to see if adequate air exchange is taking place by placing your hand over the opening of the cannula. If no air exchange, the tube is not in the trachea and should be removed immediately and the patient manually ventilated with a mask 20.Once the tube is in place, stabilize the tube with one hand until secured in place with a tube holder. 21.After the tube is secure, reconnect the patient to the ventilator 22.Apply trach dressing 23.Dispose of all supplies 24.Wash your hands Early Warning Signs It is very important for you to know the signs and symptoms of infection or other problems. Signs of Infection: • Changes in sputum color, volume, odor and consistency Causes of infection include not washing hands properly, using • • • • Dirty equipment Improper suctioning Improper trach changes Improper stoma care Breathing Symptoms: • • • • • Increased shortness of breath Wheezing Increased coughing Increased respiratory rate Increased accessory muscle use Sputum Changes: • Color change (yellow, green, tan or brown) • Increase in quantity • Change in consistency • Bloody Stoma Symptoms: • • • • Pulsating tracheostomy tube Bleeding from the stoma Discharge or odor from the stoma Swelling or redness Other Symptoms: • • • • • • • • • • Fever Loss of appetite Rapid weight gain Swelling of hands and feet Headaches Sleepiness Visual disturbances Dizziness Cyanosis Confusion or anxiety Call Breath of Life with any equipment problems. If you are having any physical problems contact your physician If you are having severe physical problems call 911 Emergency Procedures Emergency Reinsertion of the Tracheostomy Tube Sometimes as a patient is being suctioned or as trach care is being performed the trach tube could accidentally become displaced. If this happens, try to replace the trach immediately. To keep the patients airway open the following actions should be taken: 1. Replace the trach tube, using a new sterile trach tube OR 2. Reinsert the original trach tube OR 3. Occlude the stoma and use an ambu bag and mask to ventilate the patient at a rate of 8-16 breaths per minute until EMS arrives. Reinsertion Procedure: 1. If at all possible, insert the obturator and put the water soluable lubricant on the outer cannula. 2. Insert the trach tube, using an upward curved motion. The tube will slide into place as you apply gentle pressure. 3. When the tube is in place, immediately pull the obturator out. 4. Apply the trach tube holder to stabilize the trach tube. 5. Insert the inner cannula . 6. Inflate the tracheostomy cuff. 7. Make sure you can feel air coming from the opening of the cannula by placing your hand over the opening. If the patient is on a ventilator, connect him/her to the ambu bag and watch for the chest to rise and fall as you squeeze the bag. Assessment After Reinsertion: After you have reinserted the tracheost tracheostomy tube observe the patient skin color and heart rate. If at anytime during reinsertion you notice the patient becoming blue or the heart rate changes significantly, stop trying to reinsert the tube and occlude the stoma and ventilate the patient with an ambu bag and mask. Call 911 immediately and ventilate the patient. Continue to ventilate the patient with the bag and mask until EMS arrives. Reinsertion of the trach tube should take no longer than 30 seconds. You should have at least one trach tube that is 1 size smaller than the tube that the patient has. This will make insertion easier if you are having difficulty due to a swollen airway. NOTE: Reinsertion of trach tubes can be difficult. It is important to make sure you perform this procedure re in front of the respiratory therapist at the hospital before the patient is discharged to home. Infection Control: It is important to keep infections from spreading to or from patients and caregivers. To prevent this from occurring it is important to use good handwashing techniques before and after having contact with blood, body fluids and after removing your gloves. It is equally important to wear gloves when doing any procedure where the hands may come into contact with blood or body fluids. A mask should be worn if the patient has any communicable respiratory diseases. Handwashing: Good handwashing must be done with all procedures to prevent infections. Not doing proper handwashing technique is one of the most common sources of infections. The following is proper procedure for washing hands: 1. Wet your hands with warm water 2. Use antibacterial soap 3. Wash your hands for 1-2 minutes making sure to wash with friction the back and palm of each hand and between all fingers. 4. Rinse your hands thoroughly under the running water 5. Dry hands well with a paper towel Suctioning: Coughing is important to clear out secretions from the airway. Some patients with respiratory illness have weak coughs and have difficulty getting the secretions out of the airway. Secretions can obstruct the airway making it difficult for the lungs to get the oxygen they need. Suctioning removes the secretions from the airways which will allow the patient to breathe better. Suctioning can be done either by performing a sterile procedure or a clean procedure. When a patient needs suctioned they will begin to breathe noisy, cough or if on a ventilator the high pressure alarm may be alarming. More experienced patients will request to be suctioned. Notify the physician if you notice an increase in sputum production or blood in the sputum. Points to remember: • Always wash your hands before and after suctioning the patient. • Always wear gloves when suctioning • Make sure to follow either the sterile or clean technique • Discard used suction catheters • Suctioning should only be done when necessary The Suction Machine: Suction machines have a negative pressure when applied to the airway, the secretions can be removed. Each machine comes with a vacuum gauge. The recommended ranges are: • Adults: -80 to -120mmHg • Children: -80 to -100 mmHg • Infants: -60 to -80 mmHg There will also be a container for the secretions to accumulate in; a connection tube that attaches to the suction catheter; a short tube that connects to the machine pump, and a bacterial filter. How to Use the Suction Machine: 1. Connect the short, clear plastic tubing between the canister and the suction machine. 2. Connect the long, clear plastic connecting tube to the connector that goes to the canister. 3. Plug the machine into a standard wall outlet. 4. Turn the machine on and occlude the end of the long connecting tube. Adjust the regulator setting according to the recommended values. • Clockwise – increases the suction • Counterclockwise – decreases the suction 5. Empty and clean the canister at least once a day, or whenever the fluid level reaches the full line. Flush the fluid down the toilet. 6. Before the canister is replaced, it should be washed with a mild, non-detergent soap such as Palmolive and water. Rinse well with hot water. NOTE: It is important to always clean the suction canister after emptying the contents. This helps to prevent bacteria from contaminating the suction machine. 7. Clear the suction tubing by suctioning water up through the tubing. 8. The longer suction tubing should be thrown away monthly or whenever it can no longer be cleared adequately. Portable Suction Units Portable suction units are used for those patients who travel. It can also be used as a back-up system in case of power failure. Instructions: 1. Turn the unit on by turning the switch to the ON position. The unit will be running on power from one of three sources: • Home electricity • Vehicle, cigarette lighter adapter • Units internal battery 2. The charging light will come on if the unit is plugged into a wall outlet. 3. The suction pressure can be adjusted by Turning the knob on the top of the side unit clockwise. 4. Empty and clean the canister at least once per day. The fluids should be flushed down the toilet. 5. The canister should be washed with a mild non-detergent soap and water and rinsed with warm water. Sterile Suction Procedure: When sterile technique is used, a sterile suction catheter kit is used each time. Equipment: • • • • • • Suction machine and tubing Sterile suction catheter kit Sterile distilled water Sterile normal saline, for thick secretions Ambu bag Oxygen if ordered Instructions: 1. Wash your hands 2. Plug in the suction machine, connect the tubing to the jar and turn on the machine 3. Set the vacuum gauge to the proper suction pressure. 4. Open the sterile catheter kit being careful not to touch the glove or the catheter. 5. Fill the suction kit water cup with sterile water. 6. Ambu the patient for 4-6 breaths. If oxygen is ordered, make sure the ambu bag is attached to the oxygen source. 7. Put the sterile glove on your dominant hand. 8. With the non-sterile hand, grasp the suction tubing 9. With the sterile hand, pick up the package with the suction catheter and attach the suction catheter to the suction tubing. 10. Remove the protective covering from the suction catheter with your non-sterile hand. DO NOT touch anything but the catheter with your sterile hand. 11. Coil the catheter around the gloved hand making sure to protect the tip of the catheter with your gloved hand. 12. Disconnect the patient from the ambu bag 13.Gently insert the catheter into the trach tube until resistance is met. Do not jam the catheter into the trach. Do not apply suction as you are inserting the catheter. 14. Apply suction as you withdraw the suction catheter from the airway. DO not suction longer than 10-15 seconds. 15.Reconnect the patient to the ambu bag and ventilate the patient for 30 seconds. Do not touch the ambu bag with the sterile hand. 16. Repeat the suctioning and ventilating procedure, give several deep breaths with the ambu bag. 17. If the patient has trouble swallowing, you may use the same catheter and glove to suction the mouth and around the trach. Note: Remember once you have suctioned the mouth or around the trach tube, you cannot re-suction the trach until you have replaced the suction catheter with a new one. 18. If the patient is on a ventilator, reconnect them to the ventilator. 19. Rinse the suction tubing until it is clear by using the tip of the catheter in the sterile water with the suction turned on. 20.Discard the disposable suction kit supplies. Clean Suction Procedure: A clean suction technique utilizes clean gloves, but not sterile gloves each time the patient is suctioned. Instructions: 1. Wash your hands before starting the procedure 2. Plug in the suction machine, connect the tubing to the suction canister. 3. Set the vacuum gauge to the proper suction pressure. • Adult: -80 to -120mmHg 120mmHg • Children: -80 80 to -100mmHg • Infants: -60 to --80mmHg 4. Put on clean gloves. 5. Attach a clean suction catheter to the suction tubing. 6. Connect the patient to an ambu bag and ventilate for 30 seconds 7. Gently insert the catheter into the trach tube until resistance is met. Do not apply suction as you with withdraw the catheter from the airway. Never suction longer than 10-15 15 seconds. 8. Reconnect the patient to the ambu bag and ventilate for 30 seconds. 9. Repeat suctioning until the airway is clear. 10. You may clear the mouth and around the trach with the same cat catheter and glove if needed. It is important to remember you can not re-suction suction the trach until you replace the catheter with a new one. 11. Place the patient back on the ventilator and ensure that he or she is comfortable. 12. Rinse the catheter and suction connecting tube with distilled water until it is clear of mucus. 13.Wash your hands Guidelines For Caregiver Training Caregiver training will be into sections that will require successful completion of a section of training; the caregiver will continue to be involved, on a weekly basis, with the care of the patient. The caregiver will complete each individual section of the training record with instruction from Breath of Life staff and then will return demonstrate each task without assistance and then will return demonstrate each task without assistance and/or verbal cues from the staff. The staff will be present at the bedside to observe. Section One: Caregiver will begin learning care Staff will be teaching trach care, trach changes, suctioning and manual resuscitation Caregiver will demonstrate 2 independent trach changes Caregiver will demonstrate 5 independent suctioning Caregiver will be required to do trach changes and suctioning on a weekly basis Patient will have a pulse oximeter on at all times Caregiver will be independent in use of manual resuscitator Section Two: Completion of section one CPR module Education will be started on the ventilator and the circuit Caregiver will be able to recognize signs and symptoms of respiratory distress after a discussion with the attending physician and/or staff member Caregiver will complete ventilator and/or CPAP training. Patient will have a pulse oximeter on at all times Section Three: Completion of section two Caregiver will review CPR Caregiver will independently change 2 circuits on ventilator. (No Cues) Caregiver will demonstrate getting the child and the equipment in and out of the care independently a minimum of one (1) time Caregiver will have completed all training records and have records signed Section Four: Caregiver will complete total independent care of their patient as ordered by the attending physician Section Five: Completion of section four Caregiver will have a pulse oximeter at all times I have read the above guidelines for the caregiver and understand that I will required to participate with the Breath of Life staff to have training completed. Caregiver Signature: __________________________________________________________ BOL Staff Signature: __________________________________________________________ Date: __________________________ HOME NEBULIZER TREATMENTS Many medications are most effective when inhaled directly into lungs. To be inhaled into the airways of the lungs, medication must be changed from a liquid to a fine mist. To create this fine mist at home, you need a nebulizer and an air compressor. A nebulizer is a plastic container that changes liquids into a fine mist using a jet of air. The compressor, runs by electricity or battery, provides the jet of air to the nebulizer. How is the home nebulizer used? 1. Place the compressor on a hard surface. Make sure the filter is free of dust and dirt. If it is dirty, rinse it with water and then dry it. Plug in the compressor. 2. Place the prescribed amount of medication(s) into the nebulizer with a dropper or a syringe. Two medications can usually be mixed together. If you have any questions please contact your physician or Breath of Life. 3. Some asthma medicines come premixed with saline. Other medications need saline added. You can buy sterile normal saline in two ways: in unit dose plastic vials or a pressurized canister (Bronchosaline). Two squirts from the canister should be enough. Never put a homemade saline solution into a nebulizer. 4. Attach the nebulizer to the compressor tubing. Turn the power on. (The medication will immediately begin to nebulizer) Place the mouthpiece in the mouth and breathe in and out slowly through the mouth until the medication is gone. If the patient is able, tell them to take an extra deep breath every 10 breaths or so, hold that breath for 10 seconds, and then breathe out slowly. This technique permits the medication to stay in the lungs longer for better effect. If the patient can’t use a mouthpiece, use a mask. The mask can be secured loosely over the nose and mouth if needed. Most nebulizers must be held in an upright position to work well. If the mixture has coated the sided and isn’t being nebulized, gently shake the nebulizer occasionally during the treatment. An average treatment takes 10-15 minutes. The treatment is over when all medication is gone and the nebulizer makes a constant sputtering noise. Some patients cough up mucus after breathing treatments. Observe the mucus color and thickness. Normal secretions are usually thin and white or clear. Thick and sticky mucus that is yellow or green may indicate an infection. Call your physician to report a change. If the patient needs more treatments than prescribed by your doctor, or if the treatments do not improve the symptoms, call your physician. HUMIDIVENT OR “ARTIFICIAL NOSE” Purpose: To provide humidification for the respiratory system, to assist in keeping secretions manageable, and to prevent airway damage due to dryness. When to use a humidivent: When the patient is disconnected from bedside, water humidity source. How to use: The humidivent is placed between the trach tube under the patient’s chin and the ventilator tubing attachment. If the patient has a trach, but not a ventilator, the humidivent sits directly on the trach opening. How it works: There is moisture in our exhaled air. The tiny, rolled fiber inside the humidivent collects the moisture from the patients exhaled air, holds it in the paper, and uses that moisture to humidify the next breath taken in. NOTE: The humidivent helps add moisture to each inhaled breath, but doesn’t do as thorough of a job as the heated humidifier used at the patients bedside. IF the patient will be away from the bedside humidification system for several hours, or the air is particularly dry, it may be helpful to place three or four drops of normal saline on the rolled fiber areas of the humidivent. REMEMBER: The humidivent is disposable and is not to be cleaned. For infection control purposes, it would be wise to discard the used humidivent daily. If the inside of the humidivent is saturated with secretions, discard it and use a new humidivent.