Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
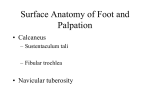
Atance: Posterior Leg and Plantar Foot The tibia and fibula are joined in two basic ways • The tibiofibular joint - Synovial • The tibiofibular syndesmosis - Fibrous joint (Includes interosseous membrane) The tibiofibular joints (together) permit the malleoli to separate slightly – During ankle dorsiflexion the wide anterior part of the trochlea can wedge itself in between the malleoli creating great stability • As well, fibers of the joints resist downward muscular pull on fibula Leg has 3 muscle compartments (formed by fascial septa) -Anterior, Posterior, and Lateral -generally closed spaces, ending at the joint -fascia of leg is very strong and unyielding (resistant to expansion, esp. proximally) -Swelling (inflammation) can build up and compromise circulation compartment syndrome fasciotomy relieves pressure Posterior Leg -separated from other compartments by interosseous membrane and posterior intermuscular septum -the muscle Plantarflex and Invert the foot -all muscles innervated by Tibial nerve -blood supply from posterior tibial artery (longer terminal branch of popliteal artery) -compartment with the most muscle mass (locomotion and propulsion) greatest amount of energy used is during concentric contraction of the plantarflexors -During gait cycle: midstance, terminal stance (heel off), and preswing (toe off) 2 subcompartments of muscles (superficial and deep) 1. Superficial group (3 muscles) -form the prominence of the calf -insertion: achilles Gastrocnemius - most superficial Soleus - Workhorse of plantarflexion Plantaris - Absent in ~ 5-10% of population (proprioception? Palmaris longus analog?) 2. Deep group (4 muscles) (all put popliteus are plantarflexors) -account for less than 7% of the total force of plantarflexion (Tendons too close to ankle joint) -Alone, it cannot raise the body (Achilles tendon rupture) 1. Flexor hallucis longus 2. Flexor digitorum longus FHL and FDL are curcial in “toe-off” action They complete the action of superficial muscles thus creating walking stride FHL is most important to our sense of foot position and leverage 3. Tibialis posterior - main invertor muscle of the leg, supports arch, initiates heel elevation 4. Popliteus Absence of Plantarflexion -much less effective push-off may be performed from the midfoot • Extension of hip with gluteus maximus, hamstrings • Extension of knee with quadriceps THE FOOT -supports body weight, provides leverage for walking and running, tremendous clinical importance (podiatry) -2 surfaces: dorsal and plantar -variation in strength and texture of the skin and fascia of the foot -stronger on plantar side bc of grip, abrasion, and its weight-bearing • • Dorsum – Thin, less sensitive skin, Loose subcutaneous tissue (Swelling) Sole (called plantar fascia) – Thick, highly-vascularized, sensitive skin – Strong, fibrous subcutaneous tissue -plantar pressure chambers – Thick central part plantar aponeurosis Plantar Aponeurosis -provides protection to underlying structures, maintains the arch, attachment for skin -arises proximally from the calcaneal tuberosity -distally, it becomes continuous with the flexor tendons of the toes Foot Joints 30 joints in the foot (26 bones) -classified according to articulating bones -Interphalangeal, metatarsalphalangeal, Intermetatarsal, tarsometatarsal, intertarsal 2 Groups of Action: -foot: eversion/inversion - toes: flexion/extension -joints also involved in spreading of the foot to absorb shock Eversion and Inversion -Intertarsal and tarsometatarsal 2 important intertarsal joints: 1. Subtalar Joint – synovial articulation btw the talus (resting on the) calcaneus 2. Transverse Tarsal Joint – 2 separate joints aligned transversely Talonavicular and Calcaneocuboid *Btw hind and mid-foot: where amputation is most likely to take places Where the midfoot and forefoot rotate on the hindfood around a longitudinal axis o Augments inversion/eversion at subtalar joint o Greatest amount of foot movement occurs here* (Transverse Tarsal) TMT joint permit soms rotation and flexion/extension o important in adaptation to unevern surfaces Flexion and Extension Joints occurs at the metatarsophalangeal and interphalangeal MTP joints are located 2.5 cm from the webbing Metatarsophalangeal joints also produce AB/Adduction -articular surfaces of the bones will allow for AB/Adduction of the toes Foot Ligaments Plantar Aspect (3) - mainly involved in supporting the longitudinal arch 1. Plantar calcaneonavicular (spring ligament) 2. Long plantar 3. Plantar calcaneocuboid (short plantar) Forefoot (2) – unite the bones of MTP and IP joints 1. Collateral ligaments 2. Deep transverse metatarsal ligaments Nerves of the Foot (5) – Tibial, Deep fibular, Superficial fibular, Saphenous, Sural (all sensory, with tibial and deep fibular also being motor) Arteries of the Foot -terminal branches of two main arteries of the leg 1. anterior tibial artery dorsalis pedis 2. posterior tibial artery plantar arteries (medial and lateral) Muscles of the Foot Intrinsic muscles of the foot originate and insert in the foot 1. Dorsal extensors(2) 2. Plantar flexors (18) (2 categories) Shared characteristics with the hands: names (lumbricles, interossei), and pads of muscles for 1st and 5th digits Function: support the arches, assist the long muscles during locomotion Plantar Foot -18 muscles, tucked under the bony arch between heel and toes (4 layers) -Innervation: Medial and Lateral Plantar Nerves (terminal branches of Tibial nerve) -Blood Supply: Medial and Lateral Plantar Arteries (from posterior tibial artery) (Lateral = larger, gives rise to deep plantar arch) Layer 1: relatively large muscles, all originate on calcaneal tuberosity and extend to phalanges 1. Flexor digitorum brevis 2. Abductor digiti minimi 3. Abductor halluces Layer 2: 1. Quadrus Plantae -helps with alignment (I: tendon of FDL) 2. Lumbricals – flex and extend (O: FDL tendons) Layer 3: *note the “channel” in FHB for passage of tendon of FHL 1. Adductor hallucis 2. Flexor digiti minimi brevis 3. Flexor hallucis brevis Layer 4: Interossei muscles (3 plantar, 4 dorsal) Atance: Anterolateral Leg and Dorsal Foot Anterior Compartment of the Leg – located just lateral to the sharp medial border of the tibia -separated by the interosseous membrane and anterior intermuscular septum -Relatively small, prone to compartment syndrome -Shin Splints (milder form) – caused by repetitive microtrauma to tibialis anterior, occurs following sudden overuse. Tx: rest and strengthening -Innervation: Deep Fibular Nerve -Blood Supply: Anterior Tibial Artery (smaller terminal branch of popliteal a.) -begins at inferior border of popliteus Retinacula- 2 band like thickenings of deep (crural) fascia, located at inferior end of anterior compart. -superior and inferior extensor retinaculum -Function: bind the tendons of the anterior compartment -prevents anterior bowstringing during dorsiflexion) Muscles of Anterior Compartment (4): Dorsiflex at the Ankles and Extend the toes -Dorsiflexion Range = 20% from neutral, and 25% strength of plantarflexion -Play critical roles in walking and balance while standing -“Digging in” Requires Dorsiflexion -during gait cycle: smooth lowering and toe ground clearance 1. Tibialis anterior – most medial and superficial (palpate tendon lateral to tibia) Leverage for strong dorsiflexion and inversion (Inferior attach.: far medial foot) Repetitive microtrauma shin splints 2. Extensor hallucis longus – deep, btw tibialis anterior and EDL Extends the great toe and dorsiflexes the ankle 3. Extensor digitorum longus – most lateral of dorsiflexors (O: fibula) The 4 tendons should be visible during dorsiflexion Each tendon forms an extensor expansion that divides One central band – base of middle phalanx Two lateral bands – base of distal phalanx 4. Fibularis tertius – separated part of EDL (share a synovial sheath), Attaches to 5th met. Weak dorsiflexor, plays a role in eversion (may protect Ant. T/F ligament) **Most frequently sprained ligament = anterior tibiofibular ligament Lateral Compartment of the Leg – smallest compartment, its an everter -separated by the anterior intermuscular septum and posterior intermuscular septum -Function: eversion (with some weak plantarflexion) -hold down medial margin of foot during toe-off -prevent excessive inversion (injury potential) -standing on one leg (balance) -Innervation: Superficial fibular nerve -Blood supply – no artery coursing through it, -receives blood indirectly from perforating arteries from fibular and anterior tibial A. Muscles: Fibularis longus and brevis Fibularis Longus: primary evertor bc greater leverage O: more superficial I: 1st metatarsal Fibularis Brevis: O: more inferior I: 5th metatarsal Plantarflexion: tendons of both muscle pass through Superior and Inferior fibular retinacula -use the lateral malleolus as a trochlea plantarflexion Uniqueness of human foot: extreme medial placement of fibularis longus Greater ability to evert more emphasis on medial foot -other primates walk on outer part of foot Clinical Stuff Most often injured nerve in lower limb = common fibular (bc superficial location) - Fx of fibular neck or knee injury may sever this nerve Foot Drop: severance of common fibulat nerve paralysis of anterior and lateral compartment muscles -no dorsiflexion or eversion Dorsal Foot 1. Extensor digitorum brevis – (more lateral) Aids extensor digitorum longus 2. Extensor hallucis brevis – (more medial) Aids extensor hallucis longus Innervation: deep fibular nerve Dorsalis Pedis: major source of blood to the forefoot -direct continuation of anterior tibial artery -begins at level of malleoli **common site to take a pulse: diminished pulse may be indicator of peripheral artery disease Key Branches of Dorsalis Pedis: – Arcuate artery - Branches supply the toes – Lateral tarsal artery - Anastomoses with arcuate artery – Deep plantar artery - Anastomoses with deep plantar arch