Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
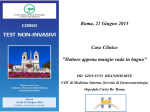
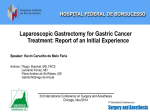
European Review for Medical and Pharmacological Sciences 2000; 4: 81-87 Diffuse gastrointestinal dysmotility by ultrasonography, manometry and breath tests in colonic inertia P. PORTINCASA, A. MOSCHETTA, M. GIAMPAOLO, G. PALASCIANO Istituto di Semeiotica Medica e Sezione di Medicina Interna, Dipartimento di Medicina Interna e Medicina Pubblica (DIMIMP), University Hospital of Bari (Italy) Abstract. – Patients with colonic inertia, the most severe form of chronic functional constipation, may present with a more diffuse panenteric motility disorder. We describe a case of a woman with severe longstanding colonic inertia associated with chronic functional dyspepsia and defective gastric, gallbladder and small intestinal motility, as confirmed by several diagnostic tests including two breath tests with the 13 C-stable isotope. A subclinical form of authonomic sympathetic neuropathy was diagnosed, providing a possible pathophysiological explanation for the presence of simultaneous multiple motility defects of the gastrointestinal tract. Key Words: 13 C-breath test, Ultrasonography, Motility, Constipation. Introduction Constipation due to colonic inertia is a frequent condition in Western countries, particularly in the female sex1. The existence of a pan-enteric motility disorder has been described in a subset of patients with colonic inertia2-4 and might be secondary to an otherwise subclinic idiopathic autonomic neuropathy involving several organs3,5-7. Case history A 42-year-old woman was referred to our clinic for severe chronic and progressively worsening constipation starting in the childhood. During the last four years she had been treated with several agents, including bulk laxatives, stool softeners, osmotic agents and senna with poor benefit. She had stopped such medications and using instead enemas and suppositories with little effect. Spontaneous bowel movements had a frequency of one in every 20-25 days. Dyspeptic symptoms such as bloating and postprandial fullness were reported several times during each week. At physical examination the nutritional status was good; her last evacuation had been 20 days before and she felt very unconfortable. There was a mildly distended abdomen with poor bowel sounds. Rectal examination was normal. The blood count, serum electrolytes, calcium, thyroid hormones were all normal and occult fecal blood was absent. An upper abdominal ultrasound was normal with respect to liver, pancreas and kidneys. Although the gallbladder was normally shaped with a thin wall (estimated fasting volume of 25 mL8), there were small asymptomatic gallstones. A pancolonoscopy was normal, apart from melanosis coli mainly in the proximal colon and mild dilatation of the sigmoid. The relevance of dyspepsia was assessed by ranking severity, frequency, and duration of four separate symptoms: epigastric pain, heartburn, belching, and bloating 9 . Total symptom score indicated a high-grade condition and was 21 out of a maximum of 48 (upper cut-off value equal to 8.7 in a control group of 100 healthy subjects from our series). An upper gastrointestinal endoscopy was normal and Helicobacter pylori infection was absent (negative rapid urease test). Several functional tests were performed to assess the motility of the gastrointestinal tract: anorectal manometry, plain abdominal X-ray films after ingestion of 60 radiopaque markers for whole-gut (colonic) transit time10, H2-breath test with 10 g lactulose as 81 P. Portincasa, A. Moschetta, M. Giampaolo, G. Palasciano substrate for small intestinal transit (orocecal transit time, OCTT) and functional ultrasonography for gallbladder and gastric emptying in response to liquid meal (200 ml Nutridrink, Nutricia, NL)11,12. Gastric emptying and small bowel transit time were also measured using the 13C stable isotope breath tests. These are noninvasive, radiation-free tests; for the stomach 100 mL 13 C-octanoic acid is added to a the yolk of a scrambled egg cooked with 5 g of margarine and eaten together with 2 slices of white bread and 150 mL of water; after passing the pylorus, rapid disintegration of the meal takes place in the duodenum, followed by rapid trans-mucosal absorption of octanoic acid into the portal vein system. For the intestine, 200 mg L-lactosyl-[ 13C]ureide 13 is added to a liquid meal (250 mL Cecemel, Nutricia, NL); this step is followed by substrate biotransformation by the bacterial intestinal flora (Clostridium innocuum and/or Klebsiella). After a further liver mithocondrial oxidation of substrates, 13CO2 is rapidly transferred into the plasma bicarbonate pool and promptly excreted in exhaled air where it can be reliably assessed by isotope-mass spectrometry. Samples of breath are collected at fixed time points (e.g. every 15-30 min) for up to 6 and 10 hours after ingestion of the substrate for gastric emptying and small bowel transit, respectively14. Before performing each test, the patient was asked to fast overnight, avoiding fibers and other fermentable products. The possible influence of the physical presence of feces on proximal gut motility was prevented by performing an enema the evening before studying the gallbladder, the stomach and the small intestine. Such tests yelded the following results: presence of rectoanal inibitory reflex without pelvic floor dysfunction (as confirmed by a normal balloon expulsion test), grossly delayed colonic transit (i.e. 133 hours compared with an upper normal limit of 68 hours in our control healthy group of 15 subjects), delayed gastric and gallbladder emptying to liquid meal (half-emptying time of 48 min and 40 min, respectively; Figure 1 and 2), and delayed orocecal transit time (OCTT: 250 min. compared with an upper normal limit of 139 min. in our control healthy group of 67 subjects). Also with 13C-breath tests, the patient 82 had delayed gastric emptying to solid meal (half emptying time of 130 min) 15 and delayed small bowel transit time (460 min)16. The integrity of the autonomic sympathetic nervous system was studied with the acetylcholine sweat-spot-test on the dorsum of the foot and resulted abnormal17. A conservative treatment was started by increasing the fiber content in the diet, cisapride (up to 20 mg t.i.d.) and subsequently erythromycin (up to 200 mg b.i.d.). There was no change in bowel movements and a mild improvement of dyspepsia. The patient was then offered surgical treatment (colectomy with ileorectostomy)18,19 because of the severity and unresponsiveness of symptoms and a progressive deterioration of the quality of life; surgery was carried out 9 months later. Immediately after operation the patient described 3-4 daily bowel movements with emission of few loose stools each time, mainly postprandially. After few weeks bowel movements could be fully controlled and she resumed normal daily activities. So far, a follow-up of 30 months has been completed and the patient is now stable describing one daily evacuation. After operation the score of dyspepsia decreased to 9, almost a normal value. A second study of combined gallbladder and gastric emptying was performed 6 months postoperatively and showed a persistent emptying delay of both organs (Figure 1 and 2). Discussion It has been suggested that functional constipation can be a symptom of a more generalized gastrointestinal motility disorder3. We describe a patient with severe and longstanding constipation due to colonic inertia associated with a major delay of gallbladder and gastric emptying, small intestinal transit and a subclinical autonomic neuropathy of the sympathetic system. To achieve such a composite diagnosis, several tests had to be carried out to study separate segments and organs of the gastrointestinal tract. This integrated approach requires a well standardized laboratory and experienced operators20. In this woman the chief complaint – constipation – was associated with high-grade dyspeptic symptoms on a background of diffuse Diffuse gastrointestinal dysmotility by ultrasonography, manometry and breath tests in colonic inertia Figure 1. Ultrasonographic study of postprandial gastric emptying showing time-related changes of cross sections of antral area at epigastrium expressed as cm2 (panel A) or normalized to fasting antral area (panel B) (small uppercase 20) in the patient with colonic inertia before and after colectomy and in a group of 60 healthy subjects (mean ± SE shown). The test meal was ingested at time 0 and consisted of 200 mL drink (300 Kcal with 13 g fat, 10 g protein, 35 g carbohydrate). The regression line is depicted for the control group (panel B) and is used for calculation of each half emptying time (T/2). The patient had both delayed and incomplete gastric emptying which persisted after colectomy. 83 P. Portincasa, A. Moschetta, M. Giampaolo, G. Palasciano Figure 2. Ultrasonographic study of postprandial gallbladder emptying showing time-related changes of gallbladder volume expressed as mL (panel A) or normalized to fasting volume (panel B)20 in the patient with colonic inertia before and after colectomy and in a group of 60 healthy subjects (mean ± SE shown). Same test meal as for Figure 1. The regression line is depicted for the control group (panel B) and is used for calculation of each half emptying time (T/2). The patient had both delayed and incomplete gallbladder emptying which persisted after colectomy. 84 Diffuse gastrointestinal dysmotility by ultrasonography, manometry and breath tests in colonic inertia impairement of gastrointestinal motility. Indeed, in a subgroup of patients functional dyspepsia can be related to either a delay of gastric emptying 21 or H. pylori infection 22. Neither conditions, however, might have been relevant in this case since H. pylori infection was absent and gastric emptying was still delayed despite improved dyspepsia postoperatively. Clinical symptoms or gastric half emptying times are poor predictors of gastrointestinal dysmotility in patients with functional dyspepsia23 and dyspepsia could also originate from altered small intestinal motility and sensory thresholds24. Indeed, we found severe delay of small intestinal transit as confirmed by two indipendent breath tests. Both ultrasonography and 13C-octanoic breath test confirmed that in colonic inertia gastric emptying can be delayed to both a liquid and a solid meal. Gastric emptying of solids has been studied using stable isotopes substrates like 13C-octanoic acid and 13CSpirulina platensis compared with radionuclide scintigraphy25-28; preliminary results are encouraging29,30 and further validation studies are being performed at our laboratory (Portincasa P. et al., personal data)14,31. In the small intestine, whereas the correlation between 13C-lactose-ureide breath test and scintigraphy was fairly good31, OCTT appears much shorter with H2-breath test than with 13C-lactose-ureide breath test; this might be due to the osmotic effect of lactulose itself which is missing for the lactose-ureide molecule32; such a difference was also noticed in this study and further information are required to widely extend the stable isotope breath test to a variety of conditions in health and disease. The presence of gallstones, although small and asymptomatic, points to an early defect of gallbladder motility causing stasis and cholesterol crystallization from a supersaturated, concentrated bile33. An additional pathogenic factor is the sluggish intestinal transit which has been associated with increased colonic bacterial dehydroxylation of primary bile salts and increased intestinal input of the lithogenic secondary bile salt deoxycholate, an additional risk of cholesterol gallstone formation34,35. An abnormal colonic motility per se, at least in the present condition, may play a minor role with respect to the gallbladder, as gallbladder hypomotility persisted after colectomy. Few items must be discussed when considering the diffuse impairment of gastrointestinal motility in colonic inertia. Firstly, a delay of the most proximal gut might be secondary to “mechanical” obstruction for longstanding retention of fecal material; however this condition is unlikely to play a major role since the motility defect was found when the colon had been properly cleaned. Secondly, a colonic inertia per se might negatively affect proximal transit even without luminal obstruction. This might not be completely true since in the present report neither gallbladder or gastric emptying improved after colectomy. By contrast, abnormal sweat-spot test points to an early defect of the autonomic sympathetic system leading to loss of fine regulation of gastrointestinal motility; we recently described this finding in a larger study3. From a practical point of view, we believe that patients with severe slow transit constipation deserve an extensive diagnostic workup to detect and to quantitate motility disturbances of the gastrointestinal tract. It is suggested that the prognosis might be poorer in the presence of severe and multiple gastrointestinal motility defects36. Lastly, although patient’s compliance is fairly good for noninvasive tests, breath tests with stable isotope require longer observation times; this, together with high costs for substrates might decrease their diagnostic power for routine clinical workups. Nevertheless, stable isotope breath tests might represent major research tools for wide epidemiological and simultaneous field studies for detecting gastrointestinal motility disturbances28,31,37,38. References 1) Gastrointestinal Disease: pathophysiology, diagnosis, management. 5th ed. Philadelphia: W.B. Saunders, 1993. 2) WATIER A, DEVROEDE G, DURANCEAU A, ABDEL-RAHMAN M, DUGUAY C, FORAND MD et al. Constipation with colonic inertia. A manifestation of systemic disease? Dig Dis Sci 1983; 28: 1025-1033. 3) ALTOMARE DF, PORTINCASA P, RINALDI M, DI CIAULA A, MARTINELLI E, AMORUSO AC et al. Slow-transit constipation: a solitary symptom of a systemic gastrointestinal disease. Dis Colon Rectum 1999; 42: 231-240. 85 P. Portincasa, A. Moschetta, M. Giampaolo, G. Palasciano 4) BASSOTTI G, STANGHELLINI V, CHIARIONI G, GERMANI U, DE GIORGIO R, VANTINI I et al. Upper gastrointestinal motor activity in patients with slow-transit constipation. Further evidence for an enteric neuropathy. Dig Dis Sci 1996; 41: 1999-2005. 5) ALTOMARE D, PILOT MA, SCOTT M, WILLIAMS N, RUBINO M, ILINCIC L et al. Detection of subclinical autonomic neuropathy in constipated patients using a sweat test. Gut 1992; 33: 1539-1543. 6) CAMILLERI M, FEALEY RD. Idiopathic autonomic denervation in eight patients presenting with functional gastrointestinal disease. A causal association? Dig Dis Sci 1990; 35: 609-616. 7) KERRIGAN DD, LUCAS MG, SUN WM, DONNELLY TC, READ NW. Idiopathic constipation associated with impaired urethrovesical and sacral reflex function. Br J Surg 1989; 76: 748-751. 8) K ISHK SMA, D AR WEESH RMA, D ODDS WJ, et al. Sonographic evaluation of resting gallbladder volume and postprandial emptying in patients with gallstones. A J R 1987; 148: 875-879. 9) BUCKLEY MJ, SCANLON C, MCGURGAN P, O’MORAIN C. A validated dyspepsia symptom score. Ital J Gastroenterol Hepatol 1997; 29: 495-500. 10) METCALF A, PHILLIPS SF, ZINSMEISTER AR, MACCARTY RL, BEART RW, WOLFF BG. Simplified assessment of segmental colonic transit. Gastroenterology 1987; 92: 40-47. 11) PORTINCASA P, DI CIAULA A, PALMIERI V, VELARDI A, VANBERGE-HENEGOUWEN GP, PALASCIANO G. Impaired gallbladder and gastric motility and pathological gastro-esophageal reflux in gallstone patients. Eur J Clin Invest 1997; 8: 653-661. 18) PICCIRILLO MF, REISSMAN P, WEXNER SD. Colectomy as treatment for constipation in selected patients. Br J Surg 1995; 82: 898-901. 19) WEXNER SD, DANIEL N, JAGELMAN DG. Colectomy for constipation. Physiologic investigation is the key to success. Dis Colon Rectum 1991; 34: 851-856. 20) PORTINCASA P, COLECCHIA A, DI CIAULA A, LAROCCA A, PALASCIANO G, RODA E et al. Standards for diagnosis of gastrointestinal motility disorders. Ultrasonography. Dig Liver Dis 2000; 32: 160172. 21) STANGHELLINI V, TOSETTI C, PATERNICÒ A, BARBARA G, MORSELLI LABATE AM, MONETTI N et al. Risk indicators of delayed gastric emptying of solids in patients with functional dyspepsia. Gastroenterology 1996; 110(4):1036-1042. 22) T ESTONI PA, B AGNOLO F, B OLOGNA P, C OLOMBO E, B ONASSI U, L ELLA F et al. Higher prevalence of Helicobacter pylori infection in dyspeptic patients who do not have gastric phase III of the migrating motor complex. Scand J Gastroenterol 1996; 31: 1063-1068. 23) W ILMER A, V AN C UTSEM E, A NDRIOLI A, T ACK J, COREMANS G, JANSSENS J. Ambulatory gastrojejunal manometry in severe motility-like dyspepsia: lack of correlation between dysmotility, symptoms, and gastric emptying. Gut 1998; 42: 235-242. 24) HOLTMANN G, TALLEY NJ, GOEBELL H. Association between H. pylori, duodenal mechanosensory thresholds, and small intestinal motility in chronic unexplained dyspepsia. Dig Dis Sci 1996; 41: 1285-1291. 12) L A B ROOY SJ, M ALE PJ, B EAVIS AK, M ISIEWICZ JJ. Assessment of the reproducibility of the lactulose H2 breath test as a measure of mouth to caecum transit time. Gut 1983; 24: 893-896. 25) CHOI MG, CAMILLERI M, BURTON DD, ZINSMEISTER AR, FORSTROM LA, NAIR KS. [13C]octanoic acid breath test for gastric emptying of solids: accuracy, reproducibility, and comparison with scintigraphy. Gastroenterology 1997; 112: 1155-1162. 13) WUTZKE KD, HEINE WE, PLATH C, LEITZMANN P, RADKE M, MOHR C et al. Evaluation of oro-coecal transit time: a comparison of the lactose- [13C, 15N]ureide 13CO2- and the lactulose H2-breath test in humans. Eur J Clin Nutr 1997; 51: 11-19. 26) CHOI MG, CAMILLERI M, BURTON DD, ZINSMEISTER AR, FORSTROM LA, NAIR KS. Reproducibility and simplification of 13C-octanoic acid breath test for gastric emptying of solids. Am J Gastroenterol 1998; 93: 92-98. 14) PORTINCASA P, PALASCIANO G. Breath testing for gastric emptying and intestinal transit evaluation. Gastroenterology International 1999; 12 (Suppl 2): 46-48. 27) M A E S BD, G E Y P E N S BJ, G H O O S YF, H I E L E MI, R UTGEERTS PJ. 13C-Octanoic acid breath test for gastric emptying rate of solids. Gastroenterology 1998; 114: 856-859. 15) GHOOS YF, MAES BD, GEYPENS BJ, MYS G, HIELE MI, RUTGEERTS PJ et al. Measurement of gastric emptying rate of solids by means of a carbon- labeled octanoic acid breath test. Gastroenterology 1993; 104: 1640-1647. 28) LEE JS, CAMILLERI M, ZINSMEISTER A, BURTON D, KOST LJ, KLEIN PD. A valid, accurate, office based, nonradioactive test for gastric emptying of solids. Gut 2000; 46:768-773. 16) G EYPENS B, B ENNINK R, P EETERS M, E VENEPOEL P, MORTELMANS L, MAES B et al. Validation of the lactose-[13C]ureide breath test for determination of orocecal transit time by scintigraphy. J Nucl Med 1999; 40: 1451-1455. 17) RYDER RE, MARSHALL R, JOHNSON K, RYDER AP, OWENS DR, HAYES TM. Acetylcholine sweatspot test for autonomic denervation. Lancet 1988; 1(8598): 1303-1305. 86 29) PERRI F, CLEMENTE R, FESTA V, QUITADAMO M, NIRO G, ANDRIULLI A. 13C-octanoic acid breath test: a reliable tool for measuring gastric emptying. Ital J Gastroenterol Hepatol 1998; 30: 211-217. 30) MAES BD, SPITZ B, GHOOS YF, HIELE MI, EVENEPOEL P, RUTGEERTS PJ. Gastric emptying in hyperemesis gravidarum and non-dyspeptic pregnancy. Aliment Pharmacol Ther 1999; 13: 237-243. 31) PORTINCASA P, MOSCHETTA A, PALASCIANO G. Nuovi breath test per lo studio dello svuotamento gastri- Diffuse gastrointestinal dysmotility by ultrasonography, manometry and breath tests in colonic inertia co e del transito intestinale. Rilevanza in pazienti con stipsi funzionale. UCP News 2001; in press. 32) M ILLER MA, PARKMAN HP, U RBAIN JL, B ROWN KL, DONAHUE DJ, KNIGHT LC et al. Comparison of scintigraphy and lactulose breath hydrogen test for assessment of orocecal transit: lactulose accelerates small bowel transit. Dig Dis Sci 1997; 42: 10-18. 33) PORTINCASA P, DI CIAULA A, BALDASSARRE G, PALMIERI V, G ENTILE A, C IMMINO A et al. Gallbladder motor function in gallstone patients: sonographic and in vitro studies on the role of gallstones, smooth muscle function and gallbladder wall inflammation. J Hepatol 1994; 21: 430-440. 34) THOMAS LA, VEYSEY MJ, BATHGATE T, KING A, FRENCH G, SMEETON NC et al. Mechanism for the transit-induced increase in colonic deoxycholic acid formation in cholesterol cholelithiasis. Gastroenterology 2000; 119: 806-815. 35) HEATON KW, EMMETT PM, SYMES CL, BRADDON FEM. An explanation for gallstones in normal-weight woman: slow intestinal transit. Lancet 1993; 341: 8-10. 36) R EDMOND JM, S MITH GW, B AROFSKY I, R ATYCH RE, GOLDSBOROUGH DC, SCHUSTER MM. Physiological tests to predict long-term outcome of total abdominal colectomy for intractable constipation. Am J Gastroenterol 1995; 90(5):748-753. 37) LEE JS, CAMILLERI M, ZINSMEISTER A, BURTON D, CHOI MG, NAIR KS. Accurate, simple measurement of gastric emptying by 13C-octanoic acid breath test (OBT) in diabetics. Gastroenterology 116, A3055 1999. 38) CAMILLERI M, HASLER WL, PARKMAN HP, QUIGLEY EM, SOFFER E. Measurement of gastrointestinal motility in the GI laboratory. Gastroenterology 1998; 115: 747-762. 87