Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
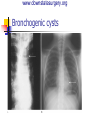
www.downstatesurgery.org Foregut Duplication Cysts Maria Georgiades April 25, 2013 Grand Rounds www.downstatesurgery.org Case Presentation 25 yo female presents with 3 year history of progressive dysphasia and weight loss PMH/PSH: rheumatoid arthritis NKDA Medications: methotrexate www.downstatesurgery.org Case Presentation 11 4.65 33 295 9.9 2.0 3.6 12 138 13 8 4.4 8 0.6 82 Vital Signs: T 97.5 BP 128/67 HR 76 RR 16 O2 sat 98% General: thin, appearing female CV: RRR, S1S2 normal Pulm: CTA bilaterally Abdom: soft nontender, nondistended Extr: no edema or tenderness 30 1.1 Upreg: negative www.downstatesurgery.org CXR CXR www.downstatesurgery.org www.downstatesurgery.org www.downstatesurgery.org www.downstatesurgery.org www.downstatesurgery.org www.downstatesurgery.org www.downstatesurgery.org www.downstatesurgery.org www.downstatesurgery.org www.downstatesurgery.org www.downstatesurgery.org Operative Summary Bronchoscopy, esophagoscopy, Right thoracotomy, resection of posterior mediastinal mass www.downstatesurgery.org www.downstatesurgery.org Pathology Esophageal Duplication Cyst www.downstatesurgery.org Postoperative Course Patient tolerated clear liquids on POD#1. Chest tubes were removed on POD#2 and 3. Discharged on POD #5 www.downstatesurgery.org Discussion History of foregut cysts Different types of foregut cysts Surgical Technique Questions www.downstatesurgery.org History of foregut cysts 1674- Charles James Blasius Esophageal duplication cyst 1881- Roth 1884- Fitz - (“duplication”) Omphalomesenteric duct remnants within abdomen www.downstatesurgery.org Foregut cysts histology Remnants from primitive foregut May contain organized histologic architecture respiratory tract or alimentary tract compoments Heterotropic lung tissue, ganglia, gastric Ileum (50%), esophagus (23%), colon (15%), stomach (5%), duodenum (4%), pancreas (1%) www.downstatesurgery.org Esophageal Duplication Cysts “Dorsal enteric cysts”, “gastroenteric cysts”, “gastrocytomas”, “enterogenous cysts” Middle and lower 1/3 of esophagus Congenital 2Men : 1Females ( 75% < 16 yo) Blood supply derived from esophagus www.downstatesurgery.org Criteria to characterize esophageal cyst Palmer criteria: 1-Attachment to the esophagus 2-Epithelium characteristic of some level of gastrointestinal tract 3-Presence of 2 layers of muscularis propria www.downstatesurgery.org Presentation Identified on routine antenatal ultrasound Asymptomatic throughout childhood Airway compression Perihilar region and younger Dysphagia, substernal pain Ectopic gastric mucosa in cyst Pain, bleeding and perforation Fistula formation www.downstatesurgery.org Associations… Contiguous or distal alimentary tract 2nd cyst Associated with congenital anomalies VACTERL Skeletal anomalies Spina bifida, hemivertebrae, vertebral fusion Genitourinary duplications, intestinal malrotation, hindgut anomalies, atresia www.downstatesurgery.org How they come about Persistent vacuoles in the wall of the foregut Simple columnar, pseudostratified ciliated columnar or stratified squamous epithelium Within or in close proximity to esophageal wall Overtime- fill with mucus and size increases Obstruction www.downstatesurgery.org Presentation Identified on routine antenatal ultrasound Asymptomatic throughout childhood Airway compression Perihilar region and younger Dysphagia, substernal pain Ectopic gastric mucosa in cyst Pain, bleeding and perforation Fistula formation www.downstatesurgery.org Diagnosis CXR Barium esophagram CT scan Smooth oval mass obstructing lumen Smooth, well defined cystic lesion devoid of calcifications EUS **Townsend: Sabiston Textbook of Surgery, 19th ed. www.downstatesurgery.org Treatment If untreated obstruction, infection, rupture Aspiration inadequate Surgical Resection Extramucosal resection or enucleation www.downstatesurgery.org Surgical Managment Indications: Symptomatic Malignancy cannot be ruled out www.downstatesurgery.org Surgical Approach Thoracotomy Thoracoscopic resection Large cysts initially drained Trocar sites directed toward post mediastinum 3 ports- 1- 5 mm camera port , 2- 5mm www.downstatesurgery.org Thoracoscopic Resection of Esophageal Duplication Cyst www.downstatesurgery.org Bronchogenic cysts Most are primary cysts of mediastinum Common in pediatric population Men> females www.downstatesurgery.org Histology www.downstatesurgery.org How do they develop? Abnormal budding or branching of tracheobranchial tree Location depends on developmental stage Paratracheal-usually to the right Adhered to esophageal wall Most common- right hilar and subcarinal www.downstatesurgery.org Clinical Presentation Not associated with other congenital anomalies Symptoms: Obstructive- neonate Infectious/inflammatory- older child Dysphagia Congenital lobar emphysema www.downstatesurgery.org Diagnosis CXR CT scan Mediastinal opacification if cyst autonomous Radiolucent if communicates with airway Air fluid levels in mediastinum Size, location and anatomic relationship Bronchoscopy www.downstatesurgery.org Bronchogenic cysts www.downstatesurgery.org Bronchiogenic cyst in middle mediastinum www.downstatesurgery.org Management and Surgical Considerations Assessment of airway Need a secure airway if in respiratory distress Clear infection prior to surgical resection Minimize adhesions and postoperative infectious complications www.downstatesurgery.org Operative Approach www.downstatesurgery.org Gastric Duplication Cysts 2 male: 1 female 3 morphologic criteria: 1-attached to stomach, contiguous with wall 2-at least one layer muscle 3-normal gastric mucosa 2-7% of all GI duplications www.downstatesurgery.org GASTRIC DUPLICATION CYST www.downstatesurgery.org Diagnosis and Treatment of gastric duplication cysts Diagnosis CT scan, MRI Treatment Surgical cystectomy or partial gastrectomy www.downstatesurgery.org Excision of Esophageal Duplication Cysts with Robotic-Assisted thoracoscopic Surgery Case 1: 12 yo female 2 cm x 1.5cm mass in posterolat mid thoraci esophagus on right JSLS. 2011 Apr-Jun; 15(2): 244–247. www.downstatesurgery.org Excision of Esophageal Duplication Cysts with Robotic-Assisted thoracoscopic Surgery Technique: Left lateral decubitus Double lumen tube 8mm port at 6th intercostal space-midaxilla 3- 8 mm ports inserted Upper chest behind scapula 2 x right lower chest JSLS. 2011 Apr-Jun; 15(2): 244–247. www.downstatesurgery.org DaVinci resection of esophageal cyst JSLS. 2011 Apr-Jun; 15(2): 244–247. www.downstatesurgery.org In Summary Esophageal duplication cysts can present with dysphagia and respiratory symptoms Differentiated by histology Operative intervention if patient is symptomatic or malignancy cannot be ruled out VATS and robotics www.downstatesurgery.org Question 1 The criteria for esophageal duplication cyst include all of the following except: A- attached to the esophageal wall B- has 2 muscularis layers C- includes cartilage in the wall D-has squamous epithelium www.downstatesurgery.org Question 2 33 year old female presents with 2 month history of dysphagia and a 2 week history of substernal chest pain. She is hemodynamically normal. She undergoes a barium swallow which is shown below. The next step in management would be: A- CT scan of the chest B- Take to operating room immediately C- Manometry D- Observation and repeat barium study in 6months www.downstatesurgery.org References Townsend: Sabiston Textbook of Surgery, 19th . - 2012 - Saunders, An Imprint of Elsevier Holcomb & Murphy: Ashcraft's Pediatric Surgery, 5th ed.- 2010 - Saunders, An Imprint of Elsevier Patterson: Pearson's Thoracic and Esophageal Surgery, 3rd ed.- 2008 - Churchill Livingstone, An Imprint of Elsevier Shew SB, Holcomb GW., III . Alimentary tract duplications. In: Ashcraft KW, Murphy JP, Holcomb GW III, editors. Pediatric Surgery. 4th ed. Amsterdam: Elsevier; 2005. pp. 543– 52. Lund DP. Alimentary tract duplication. In: Grosfeld J, O’neill J, Fonkalsrud E, Coran A, editors. Pediatric surgery. Toronto: Judith Fletcher; 2006. pp. 1389–98. Nazem M, Amouee AB, Eidy M, Khan IA, Javed HA. Duplication of cervical oesophagus: A case report and review of literatures. Afr J Paediatr Surg. 2010;7:203–5. Carachi R, Azmy A. Foregut duplications. Pediatr Surg Int. 2002;18:371–4. Takeda SI, Miyoshi S, Minami M, Ohta M, Masaoka A, Matsuda H. Clinical spectrum of mediastinal cysts. Chest. 2003;124:125–32. Nakao A, Urushihara N, Yagi T, Choda Y, Hamada M, Kataoka K, et al. Case report: Rapidly enlarging esophageal duplication cyst. J Gastroenterol. 1999;34:246–9. Bravo LO, Walls JG, Ly JQ, Lisanti CJ, Roberts SP. Esophageal duplication cyst presenting as chronic cough. Chest. 2003;124:263–4.