Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
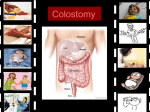
PAT IE N T IN F OR MAT ION Bowel Resection with Colostomy Please bring this book to the hospital on the day of your surgery THE OTTAWA HOSPITAL CP 55 D (REV 09 / 2008) (05/2006) Disclaimer This is general information developed by The Ottawa Hospital. It is not intended to replace the advice of a qualified healthcare provider. Please consult your healthcare provider who will be able to determine the appropriateness of the information for your specific situation. All rights reserved. No part of the contents of this book may be produced or transmitted in any form or by any means, without the written permission of The Ottawa Hospital, Clinical Pathway Project Team. © The Ottawa Hospital, February 2006. Table of Contents Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1 The Clinical Pathway –Bowel Resection With Colostomy my . . . . . Clinical Pathway – Bowel Resection With Colostomy Post-op Day Clinical Pathway – Bowel Resection With Colostomy Post-op Day Clinical Pathway – Bowel Resection With Colostomy Post-op Day Clinical Pathway – Bowel Resection With Colostomy Post-op Day Clinical Pathway – Bowel Resection With Colostomy Post-op Day .. 1. 2. 3. 4. 5. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1 2 3 4 5 6 The Bowel: How it Works . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7 Surgical Procedures That Result in a Colostomy my . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7 What is a Colostomy? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8 Basic Care . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8 How to change your appliance . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9 How to empty your bag . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10 Diet Information. n . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11 What More Should I Know? Constipation . . . . . . . . . . . Diarrhea . . . . . . . . . . . . . . Odours . . . . . . . . . . . . . . . Gas . . . . . . . . . . . . . . . . . . Effects of medication . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11 12 12 12 13 13 After You Leave the Hospital a . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13 Where Can I Get Help When I Go Home?. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14 Where and What to Buy u . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15 Tips and Timesavers . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15 When Should I Call My Doctor? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16 When Should I Call My ET Nurse? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16 Words You May Be Hearing For The First Time . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17 For More Information . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17 Clinical Pathway Booklet Introduction T his booklet will answer some of your questions about your surgery. Due to your particular problem, your surgeon will remove or bypass a part of your large bowel. This will result in a colostomy. Learning to live with a colostomy is a major change for you. With time you can resume your normal way of living. Your surgeon and his team and your nurses will be happy to answer all of your questions. You will also meet the Enterostomal Therapy (ET) Nurse. This nurse is specialized in the care of patients with a stoma and will help the team members involved in your care and assist you with discharge planning. Please bring your booklet to the hospitall as the healthcare team members will refer to these instructions throughout your hospital stay. The meaning of the words in italic is in the section Words You May Be Hearing For The First Time. The Clinical Pathway – Bowel Resection With Colostomy The health team has put together a Clinical Pathway to help plan your care. A Clinical Pathway outlines the usual day-to-day care during your hospital stay. This includes tests, treatments, activities and teaching. The outline of the Clinical Pathway for your post-operative care is on the next 5 pages. It is important for you to review it so you can participate actively in your recovery. If needed, this plan of care can be adjusted based on your condition. Bowel Resection with Colostomy 1 Clinical Pathway Booklet Clinical Pathway – Bowel Resection With Colostomy Post-op Day 1 Open Surgery Minimally Invasive Surgery Consult • ET Nurse • Dietitian • ET Nurse • Dietitian Tests • Blood test • Blood test Medication • IV PCA or Epidural infusion for pain management • Antibiotic (if ordered) • Anti-nausea medication • Anticoagulant (prevents blood clots) • Patient’s own medications if required • IV PCA for pain management • Antibiotic (if ordered) • Anti-nausea medication • Anticoagulant (prevents blood clots) • Patient’s own medications if required Assessment & Treatment • Vital signs (Blood pressure, Heart & Respiratory rate, Temperature, Bowel & Breath sounds) • Oxygen if needed • Intravenous • Abdominal dressing • Drain/ drainage • Elastic (TED) stockings • Stoma and appliance • Vital signs • Oxygen if needed • Intravenous • Abdominal incisions • Drain / drainage (if present) • Elastic (TED) stockings • Stoma and appliance Activity • Walk in hall once and sit up in chair 2 times • Walk in hall once and sit up in chair 2 times Nutrition • Surgery diet • Eat what you feel you can manage • Surgery diet • Eat what you feel you can manage • Urinary catheter • Stoma output (passing gas in bag) • Urinary catheter removed (unless otherwise ordered) • If no urinary catheter, up to void in bathroom • Stoma output (passing gas in bag) • Deep breathing and coughing exercises • Ankle exercises • Pain management • Activity • Deep breathing and coughing exercises • Ankle exercises • Pain management • Activity • Review how to open / close tail closure on ostomy bag Elimination Patient Teaching/ 2 Bowel Resection with Colostomy Clinical Pathway Booklet Clinical Pathway – Bowel Resection With Colostomy Post-op Day 2 Open Surgery Minimally Invasive Surgery Consult • ET Nurse if required • ET Nurse if required Tests • Blood test • Blood test Medication • IV PCA or Epidural infusion for pain management • Anti-nausea medication • Anticoagulant (prevents blood clots) • Patient’s own medications if required • IV PCA discontinued and pain medication started by mouth • Anti-nausea medication • Anticoagulant (prevents blood clots) • Patient’s own medications if required Assessment & Treatment • Vital signs • Oxygen if needed • Intravenous • Abdominal dressing removed, incision left open to air • Drain may be removed (if present) • Stoma and appliance • Vital signs • Oxygen if needed • Intravenous discontinued if drinking well • Abdominal incisions • Drain may be removed (if present) • Stoma and appliance Activity • Walk in hall at least 3 times • Walk in hall at least 3 times Nutrition • Surgery diet • Surgery diet Elimination • Urinary catheter removed (unless otherwise ordered) • If no urinary catheter, up to void in bathroom • Stoma output (passing gas in bag) • Urinary catheter as ordered • If no urinary catheter, up to void in bathroom • Stoma output (passing gas in bag) Patient Teaching/ • Deep breathing and coughing exercises • Ankle exercises • Pain management • Activity • Review how to open/close tail closure on ostomy bag • Deep breathing and coughing exercises • Ankle exercises • Pain management • Activity • Empty and rinse ostomy bag in toilet with supervision Bowel Resection with Colostomy 3 Clinical Pathway Booklet Clinical Pathway – Bowel Resection With Colostomy Post-op Day 3 Open Surgery Minimally Invasive Surgery • Home Care • ET Nurse if required • Home Care • ET Nurse performs stoma assessment, changes the appliance and provides supplies for discharge Tests • Blood test if required • Blood test if required Medication • Epidural weaning protocol or IV PCA discontinued and pain medication started by mouth • Anti-nausea medication • Patient’s own medications if required • Oral pain medication • Anti-nausea medication • Patient’s own medications if required Assessment & Treatment • Vital signs • Oxygen if needed • Abdominal incision • Elastic (TED) stockings • Stoma and appliance • Vital signs • Oxygen if needed • Abdominal incisions • Elastic (TED) stockings • Stoma and appliance Activity • Walk in hall at least 3 times • Walk in hall at least 3 times Nutrition • Surgery diet • Surgery diet Elimination • Urinary catheter as ordered • If no urinary catheter, up to void in bathroom • Stoma output (passing gas in bag) • Urinary catheter as ordered • If no urinary catheter, up to void in bathroom • Stoma output (passing gas in bag) Patient Teaching/ • Deep breathing and coughing exercises • Ankle exercises • Pain management • Activity • Empty and rinse ostomy bag in toilet with supervision • Deep breathing and coughing exercises • Ankle exercises • Pain management • Activity • Empty and rinse ostomy bag in toilet independently Consult Discharge Planning 4 • Confirm plan to be picked up from hospital tomorrow by 10:00 a.m. Bowel Resection with Colostomy Clinical Pathway Booklet Clinical Pathway – Bowel Resection With Colostomy Post-op Day 4 Open Surgery Minimally Invasive Surgery • ET nurse performs stoma assessment, changes the appliance and provides supplies for discharge • ET nurse performs stoma assessment, changes the appliance and provides supplies for discharge (if not done on Day 3) Medication • Pain medication • Anti-nausea medication • Patient’s own medications if required • Pain medication • Anti-nausea medication • Patient’s own medications if required Assessment & Treatment • Vital signs • Abdominal incision • Elastic (TED) stockings • Stoma and appliance • Vital signs • Stoma and appliance Activity • Activity as tolerated • Activity as tolerated Nutrition • Surgery diet • Surgery diet Elimination • Urinary catheter as ordered • If no urinary catheter, up to void in bathroom • Stoma output (passing gas in bag) • Urinary catheter as ordered • If no urinary catheter, up to void in bathroom • Stoma output (passing gas in bag) Patient Teaching/ • Deep breathing and coughing exercises • Ankle exercises • Pain management • Activity • Empty and rinse ostomy bag in toilet independently • Review post-op instructions with the nurse • Activity • Medications • Wound care • Diet • When to call the doctor/ET Nurse • Follow-up visit • Stoma care – able to empty and rinse ostomy bag in toilet independently • Urinary catheter care (if present) Discharge Planning • Confirm plan to be picked up from hospital tomorrow by 10:00 a.m. • Discharge Consult Tests Bowel Resection with Colostomy 5 Clinical Pathway Booklet Clinical Pathway – Bowel Resection With Colostomy Post-op Day 5 Open Surgery Consult • ET nurse performs stoma assessment, changes the appliance and provides supplies for discharge (if not done on Day 4) Tests Medication • Pain medication • Anti-nausea medication • Patient’s own medications if required Assessment & Treatment • Vital signs • Stoma and appliance Activity • Activity as tolerated Nutrition • Surgery diet Elimination • Urinary catheter as ordered • If no urinary catheter, up to void in bathroom • Stoma output (passing gas in bag) Patient Teaching/ • Review post-op instructions with the nurse • Activity • Medications • Wound care • Diet • When to call the doctor/ET Nurse • Follow-up visit • Stoma care – able to empty and rinse ostomy bag in toilet independently • Urinary catheter care (if present) Discharge Planning • Discharge 6 Bowel Resection with Colostomy Clinical Pathway Booklet The Bowel: How it Works When you eat, the food you swallow remains in your stomach for a short time. It then passes into the intestine (bowel). This organ is a tube-like structure that has two major parts, the small and the large bowel. You have twenty (20) feet of small bowel loosely coiled in your abdomen. The small bowel has three sections: 1 – duodenum, 2 – jejunum, 3 – ileum. You also have six (6) feet of large bowel, also called the colon that frames the small bowel. The large bowel has six sections: 1 – the ascending colon, 2 – the transverse colon, 3 – the descending colon, 4 – the sigmoid colon, 5 – the rectum, 6 – the anus. The small bowel does all the work to digest the food you eat. The large bowel acts like a sponge and removes water from your stool. It also serves as a storage area until you are ready to go to the bathroom. Though your doctor removes or by-passes part of your large bowel, you will still have all of your small bowel. You also will have a part of your large bowel to absorb the water and store your stool. Surgical Procedures That Result in a Colostomy Many bowel operations may result in a colostomy. The most common are the Hartman’s procedure where the sigmoid colon is removed or bypassed or the abdominal perineal resection (APR) where the rectum is removed and sutured closed. Bowel Resection with Colostomy 7 Clinical Pathway Booklet What is a Colostomy? A colostomy is an opening on the abdomen created at the time of your surgery. The doctor brings the end of your large bowel out through the skin and cuffs it back on itself to form a stoma. The location of the stoma will most likely be on the left hand side of your abdomen. Stool and gas from the stoma collect in an appliance secured to your abdomen. You will not feel the urge to go to the bathroom and you will not control your bowel as before. After your operation, your stool will be liquid to oatmeal-like in consistency and you will have a lot of gas. Later your stool will become thicker to resemble normal stool. As you begin to eat and the swelling in your bowel decreases, you will produce less gas. If you have a “loop colostomy”, this is a little different. The doctor brings out a loop of large bowel through a small incision on your abdomen. He places a plastic bridge under the loop to support the bowel. The doctor then makes a small incision in the exposed bowel and cuffs it back on itself. A loop colostomy is larger and actually has two openings. One opening expels stool and gas and the other produces a jelly-like substance called mucous. The location of this type of colostomy varies and it is usually a temporary stoma. The doctor/ ET Nurse will remove the bridge 7 to 14 days after your operation. Basic Care Common sense is the rule of thumb in stoma care. It is helpful to think of the care given to a baby’s bottom. You would not leave a baby in a soiled diaper for very long. You also would not change a diaper without washing the baby’s bottom thoroughly. Well, the skin on your abdomen deserves the same considerations. 8 Bowel Resection with Colostomy Clinical Pathway Booklet There are many kinds of bags. Whatever appliance you use, certain principles will guide you. • Change your appliance at least once a week. • None of your skin should be in contact with the output from your colostomy. This drainage contains elements that could easily irritate your skin. • You must change your appliance as soon as you feel burning or itchiness beneath it. If you notice some redness or breaking down of the skin around the stoma, act promptly. – Expose the skin to air for 15 to 20 minutes when you change your appliance. – Stop using soap. – Recheck the size of your stoma and change the opening of your appliance as needed. – Sprinkle a small amount of stoma powder on the reddened area. If the problem worsens or persists for more than a week, get help! Your stoma will probably get into a routine and function at regular intervals. Do your appliance change during these “quiet times”. You can choose to remove your appliance to bathe or shower, soap and water will not harm the stoma. How to change your appliance In the hospital, you will use an appliance that has 2 pieces to it. The flange is the part that sticks to your body. The bag snaps on the wafer and collects the output from the stoma. 1. Gather the supplies that you will need. This includes a flange, bag, measuring card, pencil, scissors, stoma paste (if recommended), stoma powder (if recommended), mild soap, soft washcloth and garbage bag. • Use a soap that is mild, without moisturizers or perfume 2. Prepare the flange (if you know the size of your stoma; if you don’t know the size of the stoma, go to # 3). • Trace the stoma size on the backing of the flange. • Cut out the stoma opening. • Smooth the inner edge of the opening by rubbing your finger along it. • Remove the backing on flange. • Apply stoma paste around stoma opening (if recommended). • Set aside to allow the paste to dry. • You can also apply the stoma paste directly on the skin around the stoma. Let the stoma paste dry before applying the flange. 3. Remove the old appliance. Peel back one corner and gently rub with a soapy cloth beneath the flange to loosen it. Measure the stoma to determine or check the size. Bowel Resection with Colostomy 9 Clinical Pathway Booklet • The stoma opening is 1/8 of an inch (3 mm) larger than the actual stoma. The stoma will shrink over the next 4 – 6 weeks after your operation. 4. Wash skin around stoma with warm water and mild soap, rinse soap off and pat dry. • Inspect the skin around the stoma for any redness or opened area. 5. Apply stoma powder to the stitches around the stoma (if recommended). Whisk off excess powder. • Too much powder on the skin will leave a granular surface and prevent the tape around the flange from sticking. 6. Remove paper backing on tape around flange. Center the flange over the stoma and press on the flange to ensure a good seal. Smooth down the tape around flange to the skin. • Do not stretch tape as this will cause you discomfort when you move. 7. Apply bag. Align the plastic ring on the flange to the plastic ring on the bag. Starting at the bottom, apply gentle pressure all the way around flange until bag “snaps” in place. • To help snap bag in place, make your abdomen hard by “straining”. 8. Apply tail closure. 9. Hold in place with gentle pressure for one minute to ensure a good seal. How to empty your bag In the hospital, you will be using a bag that you can empty. The nurses will show you how to empty your bag in the bathroom. Empty your bag when it is 1/3 to 1/2 full. If it overfills, it will feel heavy and pull on your skin. The weight could disrupt the seal and cause leakages. 1. Prepare the rinsing solution of cool water and mouthwash in a squirt bottle, a plastic glass or any other type of container. • You can use any type of mouthwash. 2. Place toilet paper on top of the water in the toilet. This will reduce splashing. 3. Sit as far back on the toilet as you can and spread your legs apart. 4. Remove the tail closure at the bottom of the bag and set it aside. • Your nurse will show you how to open and close the tail closure and will give you one to practice with. 5. Empty the bag between your legs, in the toilet. • If the stool is thick, put some rinsing solution into the bag and swish it around before you empty it. 6. Squirt some of the rinsing solution into the bag to rinse it. 10 0 Bowel Resection with Colostomy Clinical Pathway Booklet 7. Fold over the bottom of the bag and swish the solution around. • Don’t expect the bag to get spotless! 8. Empty the rinsing solution in the toilet. 9. Use toilet paper to wipe the inside and outside of the bottom of the bag. Depending on the type of colostomy you have, you can try to regulate the function of your bowel with irrigations (enemas). Please ask your doctor /nurse/ET Nurse for more information on this topic. Diet Information It is very important for you to eat slowly and chew your food well. Only eat what you feel you can manage. It is better, at first to eat smaller amounts but more often. This will help reduce the strain on your bowel. Fluids should be taken in small amounts (sips) and juices can be diluted with water if the acidity is a problem for you. In the hospital, you will be given many different foods to choose from. You may wish at first to try one new food at a time. This will help you identify those foods that cause a change in your bowel. However, a bowel upset can have many other causes. Should you notice a change in your bowel after eating a certain food, try this food again in a week or two. Remember, foods that have caused you pa bowel upset before surgery will probably continue to do so now. After your recovery period, be sure to eat regularly, three meals per day. Try to eat in a calm atmosphere. Skipping meals won’t reduce your bowel function but it may cause a lot of gas. Some foods also may increase gas or odour formation (see What More Should I Know?). ? The dietician will meet with you before you go home to discuss your “diet” with you. What More Should I Know? The following pages list the most common problems experienced by people who have a colostomy. Your doctor/nurse/ET nurse will gladly answer your questions or provide additional information. Bowel Resection with Colostomy 11 Clinical Pathway Booklet Constipation Constipation occurs if you do not have a bowel movement regularly. This also can happen to people who have a colostomy. Your chances of becoming constipated increase if: • your diet is too low in residue (fiber). • you limit activities. • you have a change in your normal habit. • you do not drink enough fluid. • you take pills such as aspirin, codeine or iron. Here are some suggestions that may help. You should adjust your diet to include more foods high in residue such as bran, cooked fruits or vegetables. You should drink more fluids. You can take natural laxatives such as prune juice or lemon juice in warm water. If the constipation persists for more that 2 – 3 days, call your doctor/ET nurse for advice. Diarrhea Diarrhea is watery, loose stool. This means that you will have to empty /change your bag more often. You can have diarrhea if: • you eat certain spicy foods such as pizza. • you take certain medication such as an antibiotic, an antihypertensive (high blood pressure pill) and / or a diuretic (water pill). • you drink certain fluids in large quantities such as beer, wine, alcohol, milk and fruit juices. • you have a viral infection that affects your bowel. • you experience an emotional upset or get overexcited. • you have a change in water source. • you eat certain foods such as broccoli, spinach, fresh fruit and baked beans. Here are suggestions that may help you. Increase your fluid intake by drinking small amounts often (about 4 ounces at a time). The following fluids will help replace fluid loss: tea, coffee, cola and bouillon. The following foods will help thicken your stool: boiled rice, pasta, cheese, peanut butter (creamy, not chunky), soda crackers, marshmallows and pretzels. You also can eat pureed bananas, applesauce, tapioca or rice pudding, yogurt or drink boiled milk. If the diarrhea persists for more than 48 hours, call your doctor/ET nurse for advice. Odours Odours can result from: • lack of personal and bag hygiene. 12 2 Bowel Resection with Colostomy Clinical Pathway Booklet • eating foods such as eggs, fish/shellfish, cheese, asparagus, broccoli, vegetables from the cabbage family, onions, garlic or baked beans. • taking certain pills or vitamin preparations. If your appliance is secure, the odour will only be noticeable when you empty or change it. You can use in-bag deoderant products that reduce odour. You also can drink cranberry juice, buttermilk or eat yogurt or parsley. Gas Gas production can increase if you: • use a straw • eat foods such as vegetables from the cabbage family, broccoli, spinach, peas, corn, onions, garlic, baked beans, cucumber and radishes. • chew gum or swallow air while you eat. • snore or breathe through your mouth. • drink carbonated drinks or beer. Here are some suggestions that may help. Eat slowly and chew your food well with your mouth closed. Pour carbonated drinks in a glass before drinking. Refrain from using a straw to drink. If you wish, avoid the gas-producing foods and drinks as listed. Effects of medication Most medication you take will have the same effect even though you now have a colostomy. Some medications may change the color, odor and consistency of your stool. If you have questions about any medications you are taking, ask your doctor or pharmacist. After You Leave the Hospital Your own attitude towards your colostomy will be the most important one. If you have a positive attitude, others will too. Very few people need to know about your colostomy. You can decide who to tell and when to tell them. Resuming activities after surgery is of some concern to most people. Your colostomy is in no way a restriction on your previous activities. You are free to enjoy all the activities that you enjoyed before your surgery. Rough contact sports such as football, wrestling or boxing might result in stoma bruising. Discuss it with your doctor should you want to participate in these sports. Bowel Resection with Colostomy 13 Clinical Pathway Booklet You can continue to wear whatever clothing you wore before your surgery. The appliance is flat and inconspicuous. However, consider loose clothing right after your operation, as your abdomen will be swollen. Resuming sexual activities takes time after any type of surgery. Honest and open communication with your partner is very important in finding or returning to a satisfying sexual relationship. In time, the presence of the colostomy will make little difference to you and your partner. Your particular surgery may result in physical changes that could interfere with your sexual activities. If you have concerns, discuss these with your doctor/ET nurse. Where Can I Get Help When I Go Home? While in the hospital, you will meet many people who will help you understand your colostomy care. The key person is your doctor. He will gladly answer your questions or refer you to another member of the team, the ET Nurse. This nurse is a specialist in ostomy care. Your doctor’s office telephone number is: _________________________________________ To contact the ET Nurse call: ____________________________________________________ Each campus of The Ottawa Hospital also has a STOMA CLINIC. To make an appointment call: ___________________________________________________ Private stoma clinics are also available. Your doctor might wish to send a nurse to visit you at home. This service is free of charge in most instances. The CCAC (Community Care Access Centre – Ontario) or the CLSC (Centre local des services communautaires – Québec) will provide this home care service. The nurse will make sure you are managing well at home and will give your doctor regular reports on your condition. People with an ostomy have an association for themselves. They get together once a month and discuss all sorts of topics that may interest you. The UNITED OSTOMY SUPPORT GROUP, OTTAWA, INC. is a non-profit organization to help you. For more information, call: _____________________________________________________ or visit their web site listed in the section For More Information. 14 4 Bowel Resection with Colostomy Clinical Pathway Booklet Where and What to Buy Before you leave the hospital, you will be given ostomy supplies. The home care services will later provide you with a complete list of supplies you will need to purchase and a list of places where you can buy your supplies. If you have a permanent colostomy, you can apply for a grant to help pay for your supplies. These grants come from the Ministry of Health (Ontario) or the Régie d’assurance maladie du Québec (Quebec). The ET Nurse will give you the form you need. If you have a temporary colostomy, your extended health insurance may pay for supplies. Contact the company to find out. Tips and Timesavers • You should always carry a spare appliance with you in case of leakage and especially when you visit your doctor/ET Nurse. • You should bring your ostomy supplies when you come to the hospital. If you forget, you will have to use whatever brand the hospital has in stock. • When you travel, whether you are going on a camping trip or an excursion around the world, you will need to make plans. 1. Carry a letter from your doctor stating that you have a colostomy and need supplies. 2. Make a complete list of all the supplies you need. 3. Take twice as many appliances as you might expect to use, as supplies may be difficult to get at your destination. Include a supply of baggies and/or plastic bags for disposal purposes. 4. If possible, obtain a list of suppliers along your route. 5. If you are traveling by car, store your supplies in a cool area as heat may affect the seal. If you are traveling by bus, train or plane, store your supplies in your carry-on bag. Remember that scissors will need to be left in the stored luggage if you travel by plane. 6. If traveling by plane, empty your appliance before departure and an hour prior to arrival, in case of delays at customs, etc … Bowel Resection with Colostomy 15 Clinical Pathway Booklet 7. If you need a doctor in a foreign country, contact the Canadian Embassy for referral. 8. If camping or backpacking, store your supplies in a waterproof container. 9. Foreign foods and water can cause problems. Visit your family doctor prior to departure for advice. When Should I Call My Doctor? 1. When for no reason you get cramps that last more than 2 to 3 hours, that progressively increase in intensity and you are not passing gas or stool. 2. When you notice blood mixed in your stool when you empty the bag. 3. Check with your doctor before taking any medication, including over-the-counter drugs. When Should I Call My ET Nurse? 1. If you notice a cut in your stoma. 2. If you notice bleeding at the junction between the stoma and the skin. 3. If you notice a change in the stoma size, color and appearance. 4. If you notice a skin irritation or ulcers that do not get better. 5. If you notice a severe odour lasting more than a week. 16 6 Bowel Resection with Colostomy Clinical Pathway Booklet Words You May Be Hearing For The First Time Appliance: the flange and bag you wear to collect the drainage from your colostomy. Colostomy: the type of stoma created in the colon. ET Nurse: a nurse who has taken additional training in the care of patients with a stoma. Output: stool and gas expelled from the stoma. Stoma: the actual opening of the bowel onto the abdomen. For More Information • • • • United Ostomy Association of Canada – www.ostomycanada.ca United Ostomy Support Group, Ottawa, Inc. – www.ostomyottawa.ca Colorectal Cancer Association of Canada – www.ccac-accc.ca Crohn’s and Colitis Foundation of Canada – www.ccfc.ca This booklet was prepared by the Enterostomal Therapy (ET) Nurses of The Ottawa Hospital December 2005 Bowel Resection with Colostomy 17 Clinical Pathway Booklet Notes _______________________________________________________________________________________ _______________________________________________________________________________________ _______________________________________________________________________________________ _______________________________________________________________________________________ _______________________________________________________________________________________ _______________________________________________________________________________________ _______________________________________________________________________________________ _______________________________________________________________________________________ _______________________________________________________________________________________ _______________________________________________________________________________________ _______________________________________________________________________________________ _______________________________________________________________________________________ _______________________________________________________________________________________ _______________________________________________________________________________________ _______________________________________________________________________________________ _______________________________________________________________________________________ _______________________________________________________________________________________ _______________________________________________________________________________________ _______________________________________________________________________________________ _______________________________________________________________________________________ _______________________________________________________________________________________ _______________________________________________________________________________________ _______________________________________________________________________________________ _______________________________________________________________________________________ _______________________________________________________________________________________ Bowel Resection with Colostomy 19 _______________________________________________________________________________________ _______________________________________________________________________________________ _______________________________________________________________________________________ _______________________________________________________________________________________ _______________________________________________________________________________________ _______________________________________________________________________________________ _______________________________________________________________________________________ _______________________________________________________________________________________ _______________________________________________________________________________________ _______________________________________________________________________________________ _______________________________________________________________________________________ _______________________________________________________________________________________ _______________________________________________________________________________________ _______________________________________________________________________________________ _______________________________________________________________________________________ _______________________________________________________________________________________ _______________________________________________________________________________________ _______________________________________________________________________________________ _______________________________________________________________________________________ _______________________________________________________________________________________ _______________________________________________________________________________________ _______________________________________________________________________________________ _______________________________________________________________________________________ _______________________________________________________________________________________ _______________________________________________________________________________________ _______________________________________________________________________________________ _______________________________________________________________________________________