Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
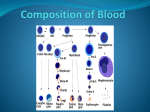
Differentiation of Anemia KY STOLTZFUS, MD ASSISTANT PROFESSOR, INTERNAL MEDICINE UNIVERSITY OF KANSAS MEDICAL CENTER JANUARY 23, 2013 Differentiating Anemia Anemia is a sign of a disease process or problem But anemia has consequences if left untreated… When you have a sign Look further and investigate cause Chronic affects of anemia Anemia, physiological impairments, and clinical outcomes. Anemia has been linked to a number of physiological impairments and clinical outcomes in community-dwelling older populations. RBCs Red Blood Cell Adults have approx. 20-30 trillion RBCs in circulation Each having over 200 million molecules of hemoglobin Each hemoglobin molecule has 4 heme molecules that carry oxygen molecule Flexible so can fit through tiny capillary spaces to offload oxygen. RBC production RBCs Life cycle of RBC 50,000 reticulocytes produced daily Reticulocyte circulates for about 1 day RBC survives approx. 110-120 days Removed by reticuloendothelial system Iron recycled to make new RBCs Under normal conditions about 1% of RBC’s removed daily Anemia Anemia Reduction in red blood cell mass NOT just a drop in Hgb lab value Definition World Health Organization <13 g/dL males <12 g/dL females Prevalence of anemia: 3.6 million people in US Differential Diagnosis of Anemia Signs/symptoms – how is anemia found? Depends on: severity rate of onset etiology patient’s overall health & oxygen demand Differential Diagnosis of Anemia Diagnosis Past medical history Family history Physical exam Lab History Patient’s age Ethnic background Females: Menstrual history (duration, frequency, flow, pregnancy) Jaundice? GI problems – blood in stool Fatigue, hx of anemia, previous transfusions History continued Medications Rx OTC Vitamins & supplements Dietary restrictions Physical exam Physical exam Pallor Conjunctiva Oral mucosa Nail beds Palmar creases Orthostatic BP changes Intravascular volume shifts Physical findings Differential Diagnosis Ways to classify anemia Etiology Reticulocyte response Lab value description morphology of RBCs Differential Diagnosis Classification of anemia Etiology Blood loss Acute Chronic Deficient erythropoiesis (Nonproduction) Excessive RBC destruction Defects extrinsic to RBC Defects intrinsic to RBC Differential Diagnosis Classification of anemia Lab value description of RBC MCV (Mean Corpuscular Volume) Microcytic Normocytic Macrocytic Differential Diagnosis Microcytic Iron deficiency Anemia of chronic disease Thalassemias Sideroblastic anemia Differential Diagnosis Normocytic Hemolytic (extrinsic) Alloimmune Autoimmune Nonimmune Hypersplenism Infections Physical trauma Hemolytic (intrinsic) Enzyme deficiencies (G6PD) Hemoglobinopathies (sickle cell disease) Membrane defects (spherocytosis) Nonhemolytic Acute blood loss Anemia of chronic disease Aplastic anemia Chronic renal insufficiency Differential Diagnosis of Anemia Macrocytic Megaloblastic Drug Related Folic acid deficiency Nonmegaloblastic Alcoholism Hypothyroidism Liver disease Myelodysplastic syndromes Reticulocytosis Spherocytosis Anemia Algorithm Establishment of anemia based on history, exam, Hgb/Hct Mean corpuscular volume (MCV) <80 fL 80 to 100 fL Microcytic pathway >100 fL Normocytic pathway Macrocytic pathway Differential Diagnosis of Anemia CASE 1 JL – 42 y/o female c/o increasing fatigue, having to take nap when getting home from work. ROS – heavy menstrual flow Xs several years, no change in bowel habits PMH – no illnesses, hx anemia, transfusions FH – no history of blood problems Meds – Occasional NSAID for joint pain Differential Diagnosis of Anemia Case 1 cont’d Exam: BP 116/74, P 74, R 22 general – mild pallor, sclera & mucosal membranes pale. CV, Resp – WNL Abd/GI – no masses, stool heme neg. GU – enlarged uterus with palpable masses Differential Diagnosis of Anemia Case 1 cont’d RBC count 3.1x1012/L (3.9-5.2x1012/L) Hgb 7.8 g/dL (12-15.6 g/dL) Hct 23.1% (35-46%) MCV 73 fL (78-102 fL) MCH 20 pg/cell (27-33 pg/cell) Reticulocyte count 1.5% (0.5-2.3%) Differential Diagnosis of Anemia Case 1 cont’d Iron 35 mcg/dL (25-170 mcg/dL) Ferritin 12 ng/mL (12-156 ng/mL) TIBC 550 mcg/dL (200-450 mcg/dL) % transferrin sat. 11% (12-57%) What does she have? http://strategicleaders.wordpress.com/2011/05/19/what-if-my-good-leader-isbad-for-you/ Microcytic anemia Differential Diagnosis of Anemia Microcytic anemia – Iron deficiency Most common cause of anemia 10-30% world population In US: 11% women, 4% men Differential Diagnosis of Anemia Microcytic anemia – Iron Deficiency Average adult has 2-4 gm stored iron Most located in RBCs Usual loss of 1-2 mg/day replaced in diet Blood loss most common cause Women lose additional 1mg daily compared to men Menses 15 mg/mo loss Pregnancy 900 mg loss Deficiency results from excessive loss or poor intake Differential Diagnosis of Anemia Microcytic anemia - Iron deficiency Serum Iron Serum ferritin Total iron binding capacity (TIBC) % transferrin saturation Differential Diagnosis of Anemia Case 2 KR is 78 y/o female with history of HTN, DM, rheumatoid arthritis and COPD. First office visit reveals no significant abnormal exam findings. Her DM and HTN have been fairly well controlled with insulin and ACE inhibitors. Differential Diagnosis of Anemia Case 2 cont’d RBC count 3.45x1012/L (3.9-5.2x1012/L) Hgb 10.2 g/dL (12-15.6 g/dL) Hct 30.3% (35-46%) MCV 76 fL (78-102 fL) Differential Diagnosis of Anemia Case 2 cont’d Iron 85 mcg/dL (25-170 mcg/dL) Ferritin 260 ng/dL (12-156 ng/dL) TIBC 220 mcg/dL (200-450 mcg/dL) % transferrin sat 60% (12-57%) How about her? http://beesmusings.blogspot.com /2009_10_01_archive.html Differential Diagnosis of Anemia Microcytic anemia – Anemia of Chronic Disease Occurs in patients with chronic diseases – cancer, collagen vascular disease, chronic infections, DM, CAD Decreased RBC survival AND decreased production Fe stores trapped in RE system – unavailable Decreased erythropoietin production Bone marrow less responsive to erythropoietin Differential Diagnosis of Anemia Microcytic anemia – Anemia of Chronic Disease Can be difficult to differentiate from iron deficiency anemia MCV – low or normal Serum iron levels low or normal Ferritin levels high or normal Target cells Differential Diagnosis of Anemia Microcytic anemia - Thallasemias Low Hgb and elevated RBC count Inherited condition of abnormal alpha or beta Hgb chain Named for abnormal Hgb chain Spectum of mild to life threatening Thallassemia traits more common in individuals of African, Mediterranean and South Asian descent Microcytic Anemia Iron Deficiency Anemia Anemia of Chronic Disease Thalassemia Ferritin Low High Normal or high Iron Low High Normal or high TIBC High Low Normal % transferrin sat Low High Normal Common patient findings Infant, pregnant, female, elderly Chronic dz, CAD, DM, malignancy African, Mediterranean, South Asian heritage Differential Diagnosis of Anemia Case 4 LR is 18 y/o female of Nigerian descent with multiple hospitalizations in past for abdominal and chest pain. Recurrence of sx’s 2 days. No hx abn or heavy menses. PE: T-101.4, BP-157/82, R-32 Lungs – rales, decreased BS bilat. Abd – diffusely tender, BS ok, enlgd spleen GU - WNL Differential Diagnosis of Anemia Case 4 cont’d RBC count 4.0x1012/L Hgb 9.8 g/dL Hct 32% MCV 84 fL (3.9-5.2x1012/L) (12-15.6 g/dL) (35-46%) (80-100 fL) Okay, you got this! http://www.mancave .co.nz/how-to-wetshave Differential Diagnosis of Anemia Case 4 cont’d Reticulocyte count Peripheral smear Bilirubin total Bilirubin direct Bilirubin indirect 3.7% (<2%) sickled cells present 2.9 mg/dL (<1.3 mg/dL) 0.2 mg/dL (<0.4 mg/dL) 2.7 mg/dL (<0.7 mg/dL) Differential Diagnosis of Anemia Normocytic anemia Hemolytic Increased RBC destruction Inherited Acquired Nonhemolytic Decreased RBC production Differential Diagnosis of Anemia Normocytic anemia Reticulocyte count Hemolytic anemia – increased Nonhemolytic anemia - decreased Differential Diagnosis of Anemia Normocytic anemia – Hemolytic anemia Rapid fall in Hgb Elevated reticulocyte count Abnormally shaped RBC’S Elevated LDH (lactate dehydrogenase) Elevated indirect bilirubin Low serum haptoglobin concentration Differential Diagnosis of Anemia Normocytic anemia – Hemolytic anemia Inherited Abnormal Hgb synthesis (sickle cell disease) Defects in enzyme function (G6PD) Defects in RBC membrane (spherocytosis) Acquired Traumatic destruction of RBC DIC, TTP, HELLP, drugs, abnormal valves Immune mediated Infection Malaria Differential Diagnosis of Anemia Normocytic anemia – Hemolytic anemia Coombs test (direct & indirect) Distinguish between immune & nonimmune causes of hemolysis (extrinsic) Peripheral smear Sickled cells – sickle cell disease ‘Bite’ cells – enzyme defects Spherocytes - spherocytosis Differential Diagnosis of Anemia Normocytic anemia – Nonhemolytic anemia Alcoholism Thyroid disease Liver disease Bone marrow disorders Differential Diagnosis of Anemia Case 5 BD 67 y/o male admitted to ER after assault. Intoxicated, unable to provide PMH PE: Ht-5’9, Wt-143#, T-98.2, BP-140/76, P-94, R20 Gen-intoxicated, skin-mild jaundice, pale Differential Diagnosis of Anemia Case 5 cont’d RBC count 4.0x1012/L (4.4-5.8x1012/L) Hgb 10.3 g/dL (13-17 g/dL) Hct 36% (41-50%) MCV 114 fL (80-100 fL) Periph smear Large, oval RBCs, multinucleated WBCs This gent? http://gawker.com/5525966/how-to-survive-your-next-senate-hearing Macrocytic anemia Differential Diagnosis of Anemia Macrocytic anemia Megaloblastic Large immature RBC precursors Maturation of nucleus & cytoplasm out of synch. Nonmegaloblastic Membrane abnormalities Differential Diagnosis of Anemia Macrocytic anemia – Megaloblastic Deficiencies of Vit. B12 or Folic acid Medications (inhibit folate metabolism) Alcohol Anticonvulsants Antiretroviral medications Oral contraceptives Sulfasalazine Trimethoprim Differential Diagnosis of Anemia Macrocytic anemia – Nonmegaloblastic anemia Alcoholism Thyroid disorders Liver disease Bone marrow disorders Reticulocytosis To Review… Classify based on history Acute vs. chronic Severity Stability of the patient Etiology Loss Lack of production Excessive destruction Thank you! Questions…