Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
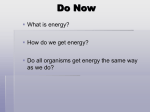
PRODUCT INFORMATION Diacol® Tablets WARNING: Life threatening dehydration and/or electrolyte disturbances may occur in 'at risk' groups - see Contraindications and Precautions. NAME OF MEDICINE Diacol® Tablets Active: Sodium phosphate monobasic USP, Sodium phosphate dibasic USP • Sodium phosphate monobasic USP Molecular formula: NaH2PO4 ⋅ H2O MW: 137.99 CAS: 10049-21-5. • H2 O • Sodium phosphate dibasic USP Molecular formula: Na2HPO4 MW: 141.96 CAS: 7558-79-4. DESCRIPTION Sodium phosphate monobasic is a white, colourless, slightly hygroscopic crystal or granule, which is freely soluble in water and practically insoluble in alcohol. Sodium phosphate dibasic is a white odourless, hygroscopic powder, which is soluble in approximately eight parts of water and is much more soluble in hot water. Apart from the active ingredient, Diacol® Tablets also contain Polyethylene Glycol 8000 (PEG) and magnesium stearate. Page 1 of 8 PHARMACOLOGY Pharmacological actions Diacol® is a bowel evacuant used to clean the colon prior to diagnostic procedures such as colonoscopy. ® Diacol , a dosing regime containing 48 grams of sodium phosphate (32 tablets), induces a diarrhoea, which rapidly and effectively cleanses the entire colon. Each administration has a purgative effect for approximately 1 to 3 hours. The primary mode of action is thought to be through osmotic action of sodium, causing large amounts of water to be drawn into the bowel. The influx of water stimulates bowel evacuation, rapidly and effectively cleansing the entire colon. Pharmacokinetics Approximately 60-65% of ingested dietary phosphate is absorbed from the gastrointestinal tract via an active energy-dependant process. Phosphate distributes into plasma and extracellular fluid, cell membranes and intracellular fluids. More than 90% of plasma phosphate is filtered and 80% of the filtered phosphate is actively reabsorbed in the steady state. Twenty-three normal healthy volunteer subjects participated in an open-label pharmacokinetic study of sodium phosphate tablets designed to generate concentration-time curves for serum inorganic phosphorous levels after administration of the sodium phosphate tablets. Subjects were administered sodium phosphate tablets consistently with the prescribed labeling for colon cleansing. A 30 gram dose (20 tablets given as three tablets every 15 minutes with clear liquids) was given beginning at 6 PM in the evening. The 30 gram dose (20 tablets given as three tablets every 15 minutes with clear liquids) was repeated the following morning beginning at 6 AM. The serum phosphorous level rose to a maximum mean (± standard deviation) peak of 3.7 ± 1.63 mg/dL above baseline, at a median of 3 hours after the first administration of sodium phosphate tablets. Following the second administration of sodium phosphate tablets the serum phosphorous level rose to a maximum mean (± standard deviation) peak of 4.4 ± 1.86 mg/dL above baseline, at a median of 4 hours. Figure 1. Mean (± standard deviation) serum phosphorus concentrations Solid bars ( ) represent the lower (2.6 mg/dL) and upper (4.5 mg/dL) limits of the reference range for the clinical laboratory. The serum phosphorous level remained above baseline for a median of 24 hours after the initial dose of sodium phosphate tablets (range 16 to 48 hours), with a maximum mean decrease of 18 hours in serum calcium of 0.3 mg/dL ± 0.03 mg/dL. Page 2 of 8 Special populations: ® Renal insufficiency. The effect of renal dysfunction on Diacol pharmacokinetics has not been studied. Since the ionised, inorganic form of phosphate in the circulating plasma is excreted almost entirely by the kidneys, patients with renal disease may have difficulty excreting a large phosphate ® load. Thus, Diacol should be used with caution in patients with impaired renal function. Hepatic insufficiency. Diacol® has not been investigated in patients with hepatic failure. The ionised, inorganic form of phosphate in the circulating plasma is excreted almost entirely by the kidneys. ® Diacol is not expected to be metabolised in the liver. Geriatric. Both AUC and Cmax values of serum phosphate were less than half in subjects >70 years of age compared to subjects < 70 years of age, based on the results of a single pharmacokinetic study, which included 6 elderly volunteers. Plasma half-life increased two-fold in subjects > 70 years of age compared to subjects < 50 years of age (3 subjects and 5 subjects, respectively). Gender. No difference in serum phosphate AUC values were observed in the single pharmacokinetic study conducted in 13 male and 10 female healthy volunteers. CLINICAL TRIALS A total of 957 adult patients were enrolled and treated in controlled clinical trials of sodium phosphate tablets. Sodium phosphate tablets were found to be comparable in cleansing efficacy to the comparison drug, a commercially available polyethylene glycol-salt (PEG-salt solution) solution ® (Cherry flavour NuLYTELY ). Two identical, single (investigator) blind, randomised, multi-centre trials were conducted comparing the efficacy and safety of sodium phosphate tablets and the PEG-salt solution comparator as a colon cleansing agent in patients undergoing routine diagnostic colonoscopy. The efficacy of overall colonic cleansing with the sodium phosphate tablets was comparable to the PEG-salt solution. In addition, the incidence of “Inadequate” colon cleansing ratings due to poor purgative preparation was similar between sodium phosphate tablets and the PEG-salt solution comparator. Also, cleansing efficacy in the ascending colon with sodium phosphate tablets was comparable to the PEG-salt solution. A total of 1055 patients were enrolled and treated in controlled clinical trials of sodium phosphate ® tablets that included Diacol as the test drug. In a Phase III clinical study 816 patients were enrolled ® and treated studying the colon-cleansing efficacy and safety of Diacol compared to another sodium phosphate tablet studied previously (see above). In the Phase 3 trial (INKP-102-04-01), patients were randomised into one of the following three sodium phosphate treatment groups: 1) Sodium phosphate tablets containing 60 grams of sodium phosphate given in split doses (30 grams in the evening before the colonoscopy and 30 grams on the next day) with at least 3.5L of clear liquids; ® 2) Diacol containing 60 grams of sodium phosphate given in split doses (30 grams in the evening before the colonoscopy and 30 grams on the next day) with 2.5L of clear liquids; and 3) Diacol® containing 48 grams of sodium phosphate (30 grams in the evening before the colonoscopy and 18 grams on the next day) with 2L of clear liquids. The primary efficacy endpoint was the overall colon cleansing response rate in the 4-point Colonic Contents Scale. Response was defined as a rating of “excellent” or “good” on the 4-point scale as determined by the blinded colonoscopist. This phase 3 study was planned to assess the non® inferiority of the two Diacol groups compared to the Sodium phosphate tablet group. Patients ranged in age from 21 to 89 years old (mean age 56 years old) with 55% female and 45% ® male patients. The Diacol 60 gram and 48-gram treatment groups demonstrated non-inferiority compared to sodium phosphate tablets. See Table 1 for the results Page 3 of 8 Treatment arm (grams of sodium phosphate) Diacol® 32 tabs (48g) n=236 Diacol® 40 tabs (60g) n=233 Sodium phosphate tablets 40 tabs (60g) n=235 Table 1: Phase 3 Study – Overall Colon Content Cleansing Rates1 No of tablets taken No of tablets Excellent Good Fair at 6pm on the day taken the next prior to day2 colonoscopy Inadequate Overall response rate (excellent or good) 20 12 76% 19% 3% 2% 95% 20 20 73% 24% 2% 1% 97% 20 20 51% 43% 6% 0% 94% 1 Colon-cleansing efficacy was based on response rate to treatment. A patient was considered to be a responder if overall colon cleansing was rated as “excellent” or “good” on a 4-point scale based on the amount of retained “colonic contents.” Excellent was defined as >90% of mucosa seen, mostly liquid stool, minimal suctioning needed for adequate visualization. Good was defined as >90% of mucosa seen, mostly liquid stool, significant suctioning needed for adequate visualization. Fair was defined as >90% of mucosa seen, mixture of liquid and semisolid stool, could be suctioned and/or washed. Inadequate was defined as <90% of mucosa seen, mixture of semisolid and solid stool which could not be suctioned or washed. 2 On the day of the colonoscopy, study medication was taken 3 to 5 hours before the start of the colonoscopy. INDICATIONS Diacol® is indicated for cleansing of the bowel when required as a preparation for certain diagnostic procedures such as colonoscopy. CONTRAINDICATIONS Diacol® is not to be used in patients with renal insufficiency, potentially pre-existing fluid/electrolyte disturbance, congestive heart failure, ascites, unstable angina pectoris, gastric retention, ileus or acute obstruction or pseudo-obstruction, severe chronic constipation, bowel perforation, acute colitis, toxic megacolon, or hypomotility syndrome (associated with, e.g., scleroderma, inadequately treated hypothyroidism). Other contraindications to this class of treatment are faecal impaction, Hirschsprung’s disease (congenital megacolon), imperforate anus, and patients at risk of dehydration due to altered senses and/or poor fluid intake. ® Diacol is contraindicated in patients with known allergy or hypersensitivity to sodium phosphate salts or any of its ingredients. WARNINGS Life threatening dehydration and/or electrolyte disturbances may occur in 'at risk' groups (see Contraindications and Precautions). Nephrocalcinosis associated with transient renal insufficiency and renal failure has been very rarely reported in patients using sodium phosphates for bowel cleansing; the majority of these reports occurred in elderly female patients taking drugs to treat hypertension or other drug products, such as diuretics or NSAIDs that may result in dehydration. Patients with conditions that may predispose to dehydration or those taking medications which may decrease glomerular filtration rate, such as diuretics, angiotensin converting enzyme inhibitors (ACE-Is), angiotensin receptor blockers (ARBs), or non steroidal anti-inflammatory drugs (NSAIDs) should be assessed for hydration status prior to use of purgative preparations and managed appropriately. Care should be taken to prescribe Diacol® per recommendations with particular attention to know contraindications and adequate hydration. Page 4 of 8 PRECAUTIONS Administration of the sodium phosphate-containing products, such as enemas or non-prescription liquid purgatives has resulted in fatalities due to significant fluid shifts, severe electrolyte abnormalities, and cardiac arrhythmias. These have been observed in patients with renal insufficiency or bowel perforation, and with misuse or overdose of these products. Use with caution in diabetic patients as the recommended liquid diet during the period of administration prior to the procedure may affect blood glucose levels, requiring adjustment of antidiabetic medication or insulin. Also use with caution in patients taking drugs that may affect electrolyte levels. Patients with electrolyte abnormalities such as hypernatraemia, hyperphosphataemia, hypokalaemia or ® hypocalcaemia should have them corrected before treatment with Diacol . Patients should be instructed to drink sufficient quantities of clear liquids or water with administration of Diacol®. Inadequate fluid intake, as with any effective purgative, may lead to excessive fluid loss and hypovolaemia. Undigested or partially digested tablets may be seen in the watery diarrhoea stool or during colonoscopy. In addition, undigested tablets from other medications may be seen. Patients should be instructed not to administer additional agents, particularly additional sodium phosphate-based purgative or enema products. ® Prolongation of the QT interval has been observed in some patients who were dosed with Diacol . ® QT prolongation with Diacol has been associated with electrolyte imbalances, such as hypokalaemia and hypocalcaemia. Diacol® should be used with caution in patients who are taking medications known to prolong the QT interval, since serious complications may occur. In these studies, prolongation of the QT interval was also observed in some patients treated with PEG-salt solution. There have been reports of generalised tonic-clonic seizures and/or loss of consciousness associated with Diacol® use in patients with no prior history of seizures. Cases of seizure were associated with electrolyte abnormalities (e.g. hyponatraemia, hypokalaemia, hypochloraemia, hypocalcaemia, hypomagnesaemia) and low serum osmolality. Neurologic abnormalities resolved with correction of fluid and electrolyte abnormalities. Other purgatives, including sodium phosphates solution and PEG3350 containing products, have also been associated with seizures and alterations of consciousness in patients with and without a prior history of seizures. Most patients with hyponatraemia associated ® with Diacol use had one or more pre-existing risk factors for hyponatraemia, including chronic use of other medications associated with hyponatraemia or seizures (i.e. tricyclic antidepressants such as nortriptyline or a PEG laxative), prior history of hyponatraemia associated with purgation, or excessive ® ingestion of fluids. Diacol should be used with caution in patients with risk factors of hyponatraemia e.g. SIADH, a history of electrolyte abnormalities, inadequately treated hypothyroidism, use of other drugs associated with hyponatraemia e.g. thiazide diuretics, or adrenal insufficiency, or with risk factors for development of tonic-clonic seizures e.g. a history of seizures, use of drugs that lower the seizure threshold such as tricyclic antidepressants, or withdrawal from alcohol or benzodiazepines. Administration of Diacol® may induce colonic mucosal aphthous ulcerations, an endoscopic finding observed with other sodium phosphate cathartic preparations. This colonscopic finding should be considered in patients with known or suspect inflammatory bowel disease. Because published data suggest that sodium phosphate absorption may be enhanced in patients experiencing an acute exacerbation of chronic inflammatory bowel disease, Diacol® should be used with caution in such patients. Diacol® was not studied in patients within 3 months of an acute myocardial infarction or cardiac surgery, including coronary artery bypass graft surgery, and therefore should be used with caution in such patients. Diacol® has not been investigated in patients with hepatic failure. The ionised, inorganic form of phosphate in the circulating plasma is excreted almost entirely by the kidneys. Diacol® is not expected to be metabolised in the liver. Page 5 of 8 Effects on fertility ® Studies to evaluate the effect of Diacol on fertility or its mutagenic potential have not been performed. Use in pregnancy and lactation ® ® No animal reproductive studies have been conducted with Diacol . It is not known whether Diacol can cause harm to the unborn foetus if administered to a pregnant woman, or interfere with reproductive capacity. Diacol® should only be given to pregnant or breastfeeding women if the benefits clearly outweigh the possible risks. Paediatric use Safety and efficacy of Diacol® have not been demonstrated for patients less than 18 years of age. Use in the elderly Of the total number of subjects in controlled Phase II and III clinical studies (INKP-102-04-01 & INKP102-03-01) of Diacol®, 19.6% were over 65, while 5.2% were over 75. No overall differences in safety or effectiveness were observed between these subjects and younger subjects. However, greater ® sensitivity of some older individuals cannot be ruled out. Diacol should be used with caution in elderly patients. Sodium phosphate is known to be substantially excreted by the kidney, and the risk of adverse reactions with sodium phosphate may be greater in patients with impaired renal function. Elderly patients are more likely to have impaired renal function, and it may be useful to assess renal function. Carcinogenicity Long term studies in animals have not been performed to evaluate the carcinogenic potential of Diacol®. Genotoxicity ® Studies to evaluate the effect of Diacol on fertility or its mutagenic potential have not been performed. Drug abuse and dependence ® Under the direction of a physician, Diacol is indicated for cleansing of the bowel when required as a preparation for diagnostic procedures such as colonoscopy, in adults aged 18 years or older. Laxatives and purgatives as a group have the potential for abuse by persons with eating disorders who ‘binge’ and ‘purge’. Preparative diet Because of the mechanism of action of Diacol®, patients should be advised to take only clear liquids by the mouth for at least 12 hours prior to starting the purgative regimen. Effects on ability to drive and use machines Diacol® may cause dizziness and drowsiness affecting the ability to drive or operate machinery Interactions with other medicines No drug interaction studies have been conducted for Diacol®. As with other purgatives the absorption of other orally administered medicines (e.g. oral contraceptives, antibiotics, and antidiabetics) may be delayed or completely prevented. Care should be taken with patients taking calcium channel blockers, diuretics, angiotensin converting enzyme inhibitors (ACE-Is), angiotensin receptor blockers (ARBs), non steroidal anti-inflammatory drugs (NSAIDs) and lithium preparations or other medications that might affect electrolyte levels as hyperphosphataemia, hypocalcaemia, hypernatraemic dehydration and acidosis may occur. ® Concurrent administration of polyethylene glycol bowel cleansing preparations and Diacol may be dangerous and is not recommended (see Adverse Effects). Page 6 of 8 ADVERSE EFFECTS ® Although these reactions have not been observed to date with Diacol , there have been reports to the Australian Adverse Drug Reactions Advisory Committee of severe adverse events and fatalities in ‘at risk’ groups with other sodium phosphate-based purgatives. The most commonly observed adverse reactions (incidence ≥ 1%, all treated patients) occurring with ® the use of Diacol are related to the desired purgative effect. Nausea, vomiting, abdominal bloating, abdominal pain, dizziness, and headache occur, and are generally transient and self-limited, requiring no specific treatment. All of these adverse events also occurred in patients who took the PEG-salt solution comparator. Small superficial mucosal ulcerations, typical of those previously reported from the use of liquid preparations of sodium phosphate, and instances of mucosal bleeding have been observed on colonoscopy. One patient, with no history of heart disease, developed an initial episode of atrial fibrillation after ® severe vomiting immediately after taking Diacol . Another patient, with known arteriosclerotic heart disease, who took the PEG-salt solution comparator developed atrial fibrillation and also vomited. No patient in the clinical studies developed predefined postural changes in vital signs with concomitant symptoms of lightheadedness or syncope. Electrolyte changes Serum electrolyte changes have been observed in patients taking Diacol® primarily affecting calcium, phosphate and potassium. These changes essentially corrected within 48 to 72 hours after dosing, were not associated with any clinical adverse events and did not require treatment. No patient developed clinically significant hypocalcaemia; among patients receiving Diacol® 60 grams (n=481) the mean decrease from baseline in calcium level was 0.5 mg/dL. No patient developed a calcium level below 7.1 mg/dL. No clinical adverse events suggestive of hypocalcaemia were observed. Mean serum phosphorous levels increased by approximately 3.6 mg/dL transiently after taking Diacol® with no apparent clinical significance. A reactive decrease in serum phosphorous 2-3 days after dosing was observed; the mean decrease from baseline at that time was 0.7 mg/dL. The mean ® decrease in serum potassium after taking Diacol was 0.5 mEq/L. DOSAGE AND ADMINISTRATION ® Patients are required to drink only clear fluids for 12 hours before taking the first dose of Diacol . The usual dosage of Diacol® for colon cleansing is 32 tablets taken orally in the following manner: Adults (over 18 years of age): The evening before the procedure, 4 tablets should be taken with at least 250mL of water or clear liquids every 15 minutes for a total of 20 tablets. The day of the procedure (starting 3-5 hours before the procedure), 4 tablets should be taken with at least 250mL of clear liquids or water every 15 minutes) for a total of 12 tablets. Clear liquids include strained fruit juice without pulp (apples, white grape, orange), water, clear broth, coffee or tea (without milk or non-dairy creamer) and all of the following that are not coloured red or purple: non-carbonated soft drinks, fruit flavoured cordials, clear ice blocks. Patients are not to repeat this purgative agent within seven days of a previous administration. No additional enema or laxative is required, and patients should be advised NOT to take additional agents, particularly those containing sodium phosphate. Renal insufficiency. Diacol® should be used with caution in patients with impaired renal function (see Pharmacokinetics and Precautions). ® Hepatic insufficiency. Diacol has not been investigated in patients with hepatic failure (see Pharmacokinetics and Precautions). Page 7 of 8 OVERDOSAGE ® There have been no reported cases of overdosage with Diacol . Purposeful or accidental ingestion of ® more than the recommended dosage of Diacol may result in severe electrolyte disturbances, including hyperphosphataemia, hypocalcaemia, hypernatraemia or hypokalaemia, as well as dehydration and hypovolaemia, with attendant signs and symptoms of these disturbances. Certain severe electrolyte disturbances may lead to cardiac arrhythmias and death. The patient who has taken an overdosage should be monitored carefully, and treated symptomatically for complications until stable. PRESENTATION AND STORAGE CONDITIONS Each tablet contains 1.102 grams of sodium phosphate monobasic and 0.398 grams of sodium phosphate dibasic for a total of 1.5 grams of sodium phosphate. Diacol® Tablets are oval, white to off-white, “SLX” bisect “102” on one side, plain on the other side. Diacol® is supplied in child-resistant bottles containing 32 tablets. Each bottle contains two silica desiccant packets, which are not to be ingested. The bottle is in a carton along with the Consumer Medicine Information leaflet. Store below 25°C. Keep container tightly closed. Discard any unused portion. NAME AND ADDRESS OF THE SPONSOR Fresenius Kabi Australia Pty Limited 964 Pacific Highway Pymble NSW 2073 Australia POISON SCHEDULE OF THE MEDICINE S3. AUST R 149914 DATE OF APPROVAL 16 January 2008. Date of most recent amendment: 4 June 2010 Page 8 of 8