Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
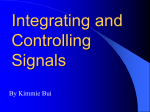
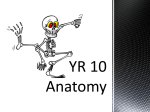
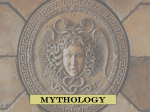
NAUSEA MANAGEMENT Assessment: Conceptualize Underlying Causes: 13 "M's" of Emesis Above Neck 1. Masses 2. Meningeal Irritation 3. Migraine / other headaches 4. Movement Causes Above Neck 1. Masses 2. Meningeal Irritation Below Neck 5. 6. 7. 8. 9. Motility Mucositis Mechanical obstruction Myocardial infarction Maternity Systemic 10. 11. 12. 13. Mentation Medication Microbes Metabolic Treat Underlying Cause Treat Nausea • Dexamethasone to inflammation / edema • If tumor, treat to mass effect • If fluid collection, drain fluid CTZ: 1. Dexamethasone 2. DA antagonist 3. H1 antagonist • Dexamethasone to inflammation / edema • If a tumor, treat to mass effect CTZ: 1. Dexamethasone 2. DA antagonist 3. H1 antagonist 3. Migraine or other headache Treat headache to pain, associated symptoms CTZ: 1. DA antagonist 2. H1 antagonist 4. MovementVestibular stimulation • motion • Treat inner ear infections • or stop offending medications CTZ: 1. DA antagonist 2. H1 antagonist Management 1. Treat underlying cause 2. Treat experience of nausea Conceptualize likely neurotransmitters. Dopamine antagonists are first choice. Titrate to effect using tCmax. Add medications from different classes. Do not overlap mechanisms of action. Causes Below Neck 5. Motility Treat Underlying Cause Treat Nausea If due to medications: • or stop responsible medications • motility with prokinetic medication • opioid inhibition of bowel function with methylnaltrexone CTZ: 1. DA antagonist 2. H1 antagonist If due to gastroparesis, e.g., Diabetes: motility with prokinetic medication CTZ: 1. DA antagonist 2. H1 antagonist Adapted from Emanuel LL, Ferris FD, von Gunten CF, Von Roenn J. EPEC-O: Education in Palliative and End-of-life Care for Oncology. © The EPEC Project,™ Chicago, IL, 2005. Open Access at www. IPCRC.net. Wood GJ, Shega JW, Lynch B, Von Roenn JH. Management of Intractable Nausea and Vomiting in Patients at the End of Life. JAMA 2007; 298(10): 1196-1207. NB: These are guidelines only and do not replace careful clinical judgment specific to each patient / family situation. © Palliative Care & Hospice Programs, OhioHealth, 2013, 2014. Permission to reproduce material is granted for non-commercial educational purposes only, provided that the attribution statement and copyright are displayed. To reproduce for all other purposes, contact the Palliative Care & Hospice Programs at 1-888-278-6615 or visit IPCRC.net. S1A NAUSEA MANAGEMENT Causes Below Neck Treat Underlying Cause Treat Nausea If due to gastric H+; gastric pH with: • Liquid antacid • H2 blocker • Proton Pump Inhibitor 6. Mucositis If due to ASA or NSAIDs ( Prostaglandin E relative ischemia mucous production): • Ensure well hydrated • Misoprostol (Prostaglandin E analogue) to perfusion • Proton Pump Inhibitor to gastric pH CTZ: 1. DA antagonist 2. H1 antagonist Causes Below Neck Treat Underlying Cause Treat Nausea 7. Mechanical obstruction (continued) If extraluminal compression, e.g., adhesions, tumor: • Dexamethasone to inflammation / edema • If tumor, treat to mass effect • Surgery to stent or bypass • Octreotide to intestinal volume CTZ: 1. DA antagonist 2. H1 antagonist 8. Myocardial Infarction • Nitrates to angina • Optimize oxygenation / cardiac perfusion • Opioid analgesics to intractable pain CTZ: 1. DA antagonist 2. H1 antagonist If due to infection, e.g., H. Pylori, Candida, CMV, Herpetic gastric erosions: • Treat infection • gastric pH with H2 blocker or Proton Pump Inhibitor 7. Mechanical obstruction If intraluminal obstruction, e.g., constipation obstipation: • Relieve impaction with enemas, disimpaction • constipation with stimulant ± osmotic laxatives If 1st trimester, estrogen / progesterone gastric emptying: • Eat small, frequent low-fat meals 9. Maternity CTZ: 1. DA antagonist 2. H1 antagonist If 3rd trimester, mass effect mechanical obstruction of bowel: • Reposition • Keep stool soft / moving with stimulant ± osmotic laxatives —————— Adapted from Emanuel LL, Ferris FD, von Gunten CF, Von Roenn J. EPEC-O: Education in Palliative and End-of-life Care for Oncology. © The EPEC Project,™ Chicago, IL, 2005. Open Access at www. IPCRC.net. Wood GJ, Shega JW, Lynch B, Von Roenn JH. Management of Intractable Nausea and Vomiting in Patients at the End of Life. JAMA 2007; 298(10): 1196-1207. NB: These are guidelines only and do not replace careful clinical judgment specific to each patient / family situation. © Palliative Care & Hospice Programs, OhioHealth, 2013, 2014. Permission to reproduce material is granted for non-commercial educational purposes only, provided that the attribution statement and copyright are displayed. To reproduce for all other purposes, contact the Palliative Care & Hospice Programs at 1-888-278-6615 or visit IPCRC.net. S1B NAUSEA MANAGEMENT Systemic Causes 10. Mentation, e.g., anxiety, stress 11. Medications/ Treatments 12. Microbes Treat Underlying Cause Treat Nausea Supportive care to reduce anxiety, underlying stress: • Behavior modification • Guided imagery • Hypnosis Diffuse effect: Centrally acting medications If during chemotherapy • Prophylactic antinauseants • Modify dose of chemotherapy See Chemotherapy Emetogenicity Table If during radiation therapy • Prophylactic antinauseants • Modify dose of chemotherapy See Radiation Emetogenicity Table If other medications, e.g., opioids, anticholinergics • Prophylactic anti-nauseants • or stop responsible medications CTZ: 1. DA antagonist 2. H1 antagonist If due to systemic infections / sepsis: • Treat underlying infection • Reduce fever Systemic Causes Treat Underlying Cause Treat Nausea If hypercalcemia due to metastases: • Rehydrate with NaCl; diurese with furosemide • Dexamethasone • Bisphosphonates, e.g., pamidronate, zoledronic acid; if caused treatable 13. Metabolic If hyponatremia due to dehydration: • Stop diuretics, including alcohol and caffeine, e.g., coffee, tea • Rehydrate with NaCl containing fluids: - Orally: soups, sport drinks, red vegetable juices - Parenterally: 0.9% NaCl CTZ: 1. DA antagonist 2. H1 antagonist If liver failure, reduce toxins with lactulose, rifaximin, neomycin If renal failure, dialyze to reduce toxins CTZ: 1. DA antagonist 2. H1 antagonist Adapted from Emanuel LL, Ferris FD, von Gunten CF, Von Roenn J. EPEC-O: Education in Palliative and End-of-life Care for Oncology. © The EPEC Project,™ Chicago, IL, 2005. Open Access at www. IPCRC.net. Wood GJ, Shega JW, Lynch B, Von Roenn JH. Management of Intractable Nausea and Vomiting in Patients at the End of Life. JAMA 2007; 298(10): 1196-1207. NB: These are guidelines only and do not replace careful clinical judgment specific to each patient / family situation. © Palliative Care & Hospice Programs, OhioHealth, 2013, 2014. Permission to reproduce material is granted for non-commercial educational purposes only, provided that the attribution statement and copyright are displayed. To reproduce for all other purposes, contact the Palliative Care & Hospice Programs at 1-888-278-6615 or visit IPCRC.net. S1C NAUSEA MANAGEMENT Non-Pharmacological Management: Acupuncture, behavior modification, hypnosis, imagery, modification of eating habits / odors Pharmacological Management Dopamine Antagonists Haloperidol 0.5-2 mg PO / SC / IV q 12-24 hrs Metoclopramide 10-20 mg PO / SC / IV q 6 hrs Prochlorperazine 10-20 mg PO q 6 hrs Prochlorperazine 25 mg PR q 12 hrs Olanzapine 5-10 mg PO daily Serotonin Antagonists Ondansetron 4-8 mg PO / SC / IV q 6 hrs Granisetron 1 mg PO / IV daily or q 12 hrs Dolasetron 200 mg PO / IV daily Palonosetron 0.25 mg PO / IV daily Histamine Antagonists Diphenhydramine 25-50 mg PO / SC / IV Meclizine 25-50 mg PO q 6 hrs Hydroxyzine 25-50 mg PO q 6 hrs Promethazine 25 mg PO / PR q 6 hrs Promethazine 12.5-25 mg IV q 6 hrs Acetylcholine Antagonists Scopolamine patch 1-3 TD q 72 hrs Scopolamine 0.1-0.4 mg SC / IV q 4 hrs Central Action Dexamethasone 2-20 mg PO / SC / IV daily Dronabinol 5-25 mg PO/24 hrs div q 2-4 hrs Lorazepam 0.5-2 mg PO / SC / IV q 8 hrs Inoperable Obstruction Octreotide 100-400 mcg or more SC / IV q 8 hrs or 10-80+ mcg/hr SC infusion Scopolamine 0.1-1.0+ mg/hr SC infusion Glycopyrolate 0.1-1.0+ mg/hr SC infusion div = In divided doses Adapted from Emanuel LL, Ferris FD, von Gunten CF, Von Roenn J. EPEC-O: Education in Palliative and End-of-life Care for Oncology. © The EPEC Project,™ Chicago, IL, 2005. Open Access at www. IPCRC.net. Wood GJ, Shega JW, Lynch B, Von Roenn JH. Management of Intractable Nausea and Vomiting in Patients at the End of Life. JAMA 2007; 298(10): 1196-1207. NB: These are guidelines only and do not replace careful clinical judgment specific to each patient / family situation. © Palliative Care & Hospice Programs, OhioHealth, 2013, 2014. Permission to reproduce material is granted for non-commercial educational purposes only, provided that the attribution statement and copyright are displayed. To reproduce for all other purposes, contact the Palliative Care & Hospice Programs at 1-888-278-6615 or visit IPCRC.net. S1D