Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
iCITCrSOIl™
Jefferson Woman's Medical Specialties Center
University Physicians
T 215.955.5000
F215.923.J089
-'
*
Thank you for choosing Jefferson Center for Women's Medical Specialties, Division of Urogynecology for your care. Our
office is located at:
834 Chestnut St.
3rd Floor; Suite 300
Philadelphia, PA 19107
(215)955-5000
Please note: The entrance to the building is on 9th street between Chestnut and Sansom streets.
What to Expect During Your Office Visit
Dr. Joseph Montella is a board certified gynecologist, who is fellowship trained in Urogynecology, the specialty which
treats illnesses related to female urinary incontinence and pelvic relaxation problems.
Since your office visit is related to a Urogynecologic concern, a pelvic and rectal exam will be performed.
What to Bring to Your Office Visit
In order to provide you with the best possible care, we ask your cooperation in completing several forms prior to your first
visit. Enclosed you will find a patient registration form and medical history questionnaire; please do not mail these forms
to the office.
Please bring the following information with you to your first appointment:
1. Completed registration form
2. Completed medical history questionnaire
3. Completed voiding diary
4.
Any records that you have related to Urogynecology especially any reports
from surgery
5. A list of your current medications
6. Arrive with a full bladder. If you are uncomfortable when you arrive, please
inform our Front Desk Staff.
Date of Appointment:
Time of Appointment:
Please arrive at least 15 minutes prior to your appointment's scheduled time to allow yourself time to complete additional
paperwork. If you are not able to keep your appointment, we ask that you call our office to cancel so that we may offer
this appointment to another patient. If you arrive more than 20 minutes after your scheduled appointment time, you will
be asked to reschedule your appointment
Thank you,
Joseph M. Montella, M.D.
Director, Division of Urogynecology
Department of Obstetrics & Gynecology
• 834 Chestnut Street, Ben Franklin House, Suite 300, Philadelphia, PA 19107-5127
THOMAS JEFFERSON UNIVERSITY
Directions to Jefferson Center for Women's Medical Specialties
From the Pennsylvania Turnpike
Exit at Valley Forge. Take Rt. 76 East to 1-676 East to the 8th Street/Chinatown Exist. Take 8th
Street to Walnut Street, then make another right onto 9th Street. The Benjamin Franklin House
will be on your right, about 11A blocks. Parking is on the left across from the building.
From 1-95 North of Wilmington
Take Exit 22 Independence Hall/Callowhill Street, following signs for Callowhill Street.
Proceed on Callowhill to 8th Street (south). Turn left onto 8 Street and follow it to Walnut
Street. Turn right onto Walnut Street, then make another right onto 9th Street. The Benjamin
Franklin House will be on your right, about 11A blocks. Parking is on the left^ across from the
building.
From 1-95 South (from Bucks County)
Take Exit 22 Independence Hall/Callowhill Street, following signs for Callowhill Street.
Proceed on Callowhill to 8th Street (south). Turn left onto 8 Street and follow it to Walnut
Street. Turn right onto Walnut Street, then make another right onto 9th Street. The Benjamin
Franklin House will be on your right, about 11A blocks. Parking is on the left, across from the
building.
From New Jersey Shore Points
Take the Atlantic City Expressway North to Rt. 42 North. Follow signs for the Benjamin
Franklin Bridge (toll). Get into the extreme LEFT lane and follow signs for 8th Street/Chinatown
Turn left into 8th Street and follow it to Walnut Street. Turn right onto Walnut Street, then make
another right onto 9th Street. The Benjamin Franklin House will be on your right, about 11A
blocks. Parking is on the left, across from the building.
From Central New Jersey
Routes 70 West and 38 West will take you to the Benjamin Franklin Bridge. Cross over the
Benjamin Franklin Bridge (toll). Get into the extreme LEFT lane and follow signs for 8th
Street/Chinatown Turn left into 8th Street and follow it to Walnut Street. Turn right onto Walnut
Street, then make another right onto 9th Street. The Benjamin Franklin House will be on your
right, about 11A blocks. Parking is on the left, across from the building.
From New York
Take the New Jersey Turnpike South to Exit 4 / Rt. 73 North. Take Rt. 73 North to Rt. 38 West.
Follow Rt. 38 West to the Benjamin Franklin Bridge. Cross over the Benjamin Franklin Bridge
(toll). Get into the extreme LEFT lane and follow signs for 8th Street/Chinatown Turn left into
8* Street and follow it to Walnut Street. Turn right onto Walnut Street, then make another right
onto 9th Street. The Benjamin Franklin House will be on your right, about 11A blocks. Parking is
on the left, across from the building.
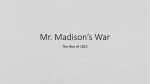
University Physicians
»-filt>«t Strctt
j^j SEPTA Market East Station
-*»- Madcet ftntt
Street Direction
Emergency Entrance
Valet Parking
Parking Garages/Lots
tnmcesNoteiO
. 10thflcGhes^MitSt.Garage
JBatrances on 10th St and on
SansomSt
Central Parking System
Open lot between llth and 12th
Ccnttal Paridng System (Eglin)
'i2tfa~*l»d SansoniSt.
Alright Paricing Garage
12th Sfc between Sanwra
£. Girard Square Parking
1120 aover St, between Chestoat
and Ludlow Sts.
E Tic Auto Park at GaUeiy Mall
10th St between Arch and Filbert Sts.
G. Philadelphia Parking Authority Garage
10th and Ludlow Sts.
H. Wills Ef e Hospital-Walnut
Towers Garage
L Jefferson Hospital for
Ncuroscience Garage
8th and 9th Sts, between Locust
and Walnut Sts.
J. Walnut Street Theater Lot
819 Walnut St
K- Central Parking System
Open lot between 8th and 9th Streets
on Market St
8th and 9th Sts. between Locust
and Walnut Sts.
JQ 09022)
Patient Demographics Form
University Physicians
Patient Name:
(Please Print)
'
Date of Birth: __
Jefferson University Physia'ans ("JUP") is participating in the Medicare and Medicaid Electronic Health Record
Incentive Program ("Program"). The federal government requires us to record specific demographic information
about ail of our patients. We are asking you to provide the demographic information below for Program purposes.
Please check the appropriate boxes below. Only one entry in each section can be chosen.
1. Language:
D English
D Other (Please List)
2. Race:
D African American or Black
D American Indian or Alaska Native
D Asian
D Caucasian or White
D Native Hawaiian or Other Pacific Islander
D Unknown
D Declined
3. Ethnicity:
D Hispanic or Latino
D Non-Hispanic or Non-Latino
D Unknown
D Declined
OflM 84747 (HEVt 03/12) JQ 12-1200
.
'.
Jefferson.University Physicians
JUP Patient Registration Form
Please complete this form in order to ensure proper hilling of your s^rvir^s Ptea<:<> PrinfPatient's Last Name
Patients First Name
i
DOB
Sex
/
Soc ial Security Number
Race
/
DM DF
D African American or Black
O American Indian or Alaska Native
Ethnicity
D Hispanic or Latino
ilarital Status
DSingte
O Non-Hispanic or Non-Latino
DMarried
D Widowed
Ml
Language
n English H Other
D Native Hawaiian or Other Pacific Islander
D Unknown
D Declined
D Asian
D Caucasian or White
D Separated
Address Line 1
Today's Date:
D Unknown
D Declined
D Divorced
D Other
Address Line 2
fty
State
ome Phone
Daytime Phone
Zip
Cell Phone
ame E-mail
np Status
D Employed Full Time
D Active Military
D Employed Part Time
n Disabled
D Setf-Employed
riHomsmaksr
iployer
•plover's Address Line 1
Q Unemployed
H Student
nOttwr
WorkPhone
Employer's Address Line 2
f
State
Zip
Please complete if guarantor is other than self. (Guarantor is the person financially responsible for this patient's bill.)
Guarantor's Last Name
Guarantor's First Name
DOB
Sex
/
/
DM
Guarantor's Address Line 1
Social Security Number
Patient^ Relationship to the Guarantor
Ml
Home Phone
OF
Guarantor's Address Line 2
City
State
GuarantorTs Employer
Guarantor Employer's Address Line 1
Zip
Guarantor Employer's Address Une 2
Cfty
State
Zip
Emergency Contact Information
Emergency Contact's Last Name
Emergency Contact's First Name
Patient's Relationship to the Emergency Contact
Daytime Phone
Ml
Cell Phone
Please select the source in which you heard of our practice
O Billboard D Brochure
OPatient
D Health Fair
D Health Plan
DPhoneBook DPhys-OffTER DRelatrve
D Internet
D JEFF NOW® D Mass Mailing
DRadio
DTV
D Newspaper/Mag.
D Ongoing Care
DWordofMouth DOther
nsurance Information A separate form is required for workers' compensation, automobtte liability, or legal services.
'rimary Insurance Company Name
Subscriber's Last Name
Subscriber's Last 4 digits of SS*
Subscriber's First Name
Subscriber^ DOB
Patient's Relationship to the Subscriber
Subscriber's DOB
Patient's Relationship to the Subscriber
Subscriber's Employer
econdary Insurance Company Name
ubspriber's Last Name
jbscrfber-s Last 4 digits of SS#
*) 4734-00 (REVC 03/12$ ,SG 12-1572
Subscriber's First Name
Subscriber's Employer
Jefferson.
JUP Communication of Protected Health Information
University Physicians
Patient Name:.
(Please Print)
Date of Birth:.
MRN:.
PartA
You have informed Jefferson University Physicians (JUP) that in certain circumstances, you would like us to
share your medical information with specified individuals (e.g., your spouse, mother, etc.).
JUP agrees to communicate with persons whom you designate regarding your protected health information.
This agreement will remain in effect unless you provide us with written notice to terminate this consent.
PartB
I hereby grant Jefferson University Physician's department/division of
permission to communicate my protected health information to the following individuals:
Name:
Relationship:
Address:
Telephone #:
Name:
Relationship:
Address:
Telephone #:
Name:
Relationship:
Address:
Telephone #:
Name:
Relationship:
Address:
Telephone #:
Patient Signature:.
Date:
Witness:
Date:
FORM 76M7 pEtt ItVKDJG 11-0070
Lafjfiarcrwi
JUP PATIENT SIGNATURE ON FILE FORM
JdLd dl/lle
University Physicians
Patient Name:
L_
Date of Birth:
(Please Print)
IDX Account #:
Medicare
I request that payment of authorized Medicare benefits be made either to me or on my behatf to Jefferson University Physicians and/or to the individual
Attending Physician, for any services furnished to me by that Physician. I authorize any holder of medical information about me to release to the Centers for
Medicare & Medicaid Services and its agents any information needed to determine these benefits or the benefits payable for related services. I permit a copy
of this authorization to be used in place of the original, and request payment of medical insurance benefits to myself or the party who accepts assignment.
In order to comply with Medicare regulations, please answer the following questions:
• Are you or your spouse employed?.
DY DN
• Has treatment been authorized by the V.A.?
• Do you or your spouse have other insurance?
DY.DN
• Are you covered under the Black Lung Program?
• Are you disabled or have end stage renal disease?
DY ON
• Is there Medigap coverage secondary to Medicare?
• Is illness/injury the result of an auto accident?
DY DN
• Is there insurance coverage primary to Medicare?
• Did illness/injury occur at work?
DY DN
• Is there employer supplemental coverage
secondary to Medicare?
...DY QN
DY DN
DY D N
D Y ON
DY D N
Medigap (Medicare Secondary Insurance)
I request that payment of authorized Medigap benefits be made either to me or on my behalf to Jefferson University Physicians for any services
furnished to me by that physician. I authorize any holder of Medicare information about me to release to my Medigap Coverage any information
needed to determine these benefits payable for related services.
Pennsylvania Medical Assistance
I understand that payment for service(s) or items received will be from Federal and State funds, and that any false claims, statements, or documents,
or concealment of material may be prosecuted under applicable Federal and State laws.
Commercial
Assignment of Insurance Benefits
I hereby authorize payment directly to Jefferson University Physicians for medical benefits including any Major Medical benefits otherwise payable to me
under the terms of my policy but not to exceed the balance due to the physicians. In making this agreement, I understand and agree that I am financially
responsible to-the above party for charges not paid under this insurance policy. I permit a copy of this authorization to be used in place of the original.
General
Release of Information
I hereby authorize Jefferson University Physicians to disclose to my insurance company(s) copies of my medical records(s) to obtain payment for services or
as part of a payment review of medical services, or in the case of Workers Compensation claims, to my present or past employees). Additionally, I authorize
Jefferson University Physicians to release copies of my medical record(s) to other health care providers serving as consultants to my physician, including
referrals for treatment. I recognize that the information disclosed may be protected by federal and/or state law, and I specifically consent to disclose of such
information. I understand that this authorization may be revoked at any time, except to the extent that action has been taken in reliance upon it.
Use of Photograph
The undersigned agrees that any patient photographs taken in connection with medical treatment will be considered a part of the patient's medical
record and may be used by the patient's health care provider solely for purposes of patient identification.
Financial Agreement
In consideration of the services rendered to the below named patient, the undersigned agrees to pay Jefferson University Physicians in accordance
with its regular charges and terms and, if this account is referred to an attorney or agency for collection, to pay attorney(s) fees, court costs, and
collection expenses. I also agree to beresponsiblefor charges not covered by insurance. I understand that my obligation to pay Jefferson University
Physicians may not be deferred for any reason, including pending legal action against other parties, to recover medical costs.
Fhe undersigned certifies that each has read and understands the above terms and conditions.
'atient Signature
Date
atient's Agent Representative and Guarantor Signature
Date
RM »1 1«7 PEV. Oi/tO) JO 1 1-05SO
Jefferson™
University Physicians
Jefferson Center for Women's Medical Specialties - Urogynecology
Medical History Questionnaire
Date
Name
Blrthdate
Marital Status
a s DM ao aw a sep
Sodal Security
Please state your problem in your own words
Who referred you to our practice?
Name
Address
Phone Number
Who is your Gynecologist?
Name
Addres
Phone Number
Pregnancy History
Year of Pregnancy
TamSOHIi HM.OM4
Birth Weight
Sex
Vaginal or Cesarean?
If Cesarean, reason?
Complications
JGOUMCO
JeffersorL
University Physicians
Medical History Questionnaire
JToday's Date:_
Provider you are seeing today:_
Date of Birth:
Patient's Name:
Why are you here today?.
Did a physician request that you see one of our providers today?
Q Yes Q No
If yes, name of physician:.
Past Medical History (check all that apply):
Q No Past Medical History
I] Acute Myocardial Infarction (Heart Attack)
Q Kidney Problems
Anemia (Low Blood Count)
Lower Back Pain
_ Arthritis
Mitral Valve Disorder
. LL Asthma
Murmues
>.
_ Autoimmune Disorder (Lupus/Sderoderma/RA)
_ Obesity
_ Bleeding Disorder
r Obstructive Sleep Apnea Blood Transfusion Complications
_ Osteoporosis
Cancer - list type(s):
_ Peripheral Vascular Disease (Poor Circulation)
Pneumonia
Pulmonary Disease (Lung Diseasej
U Chest Pain (Angina)
1
3 Chronic Liver Disease
Recent Methicillin-resistant Staph aureus (MRSA)
] COPD (Chronic Obstructive Pulmonary Disease)
Rheumatic Fever
Diabetes Mellitus
fj Seizure Disorder
Emotional Disturbance
C Sinusitis
:
Gastric/Duodenal Ulcer
Stroke Syndrome
?
Thromboembolic Disease (Blood Clot Disorder)
Heart Disease
Thrombophlebitis
Heartburn
Thyroid Disorder
Hepatic (Liver) Disease
Transient Ischemic Attack (Mini Stroke)
4epatitis
Tuberculosis
HIV Infection
Hypercholesterolemia
Other (specify):
Hypertension
|
D Im'table Bowel Syndrome
|
ff
r
r
r
"
Suraerv:
L7I No Surgical History
Date:
Familv History (check all that apply):
Q No Family Medical History
Family Member*:
O Anemia (Low Blood Count)
Hypercholesterolemia
l~l ~ - - -,er - list type(s):
Hypertension
Osteoporosis
Pulmonary Disease
Renal Disease
D
tes Mellitus
Stroke Syndrome
ysema
Thromboembolic Disease
Disease
I] Unattainable-Patient Adopted
ic (Liver) Disease
H Other:
I LJ i-amny Health Status of Father - Deceased
Age:
Cause:
Age:
Cause:
C Family Health Status of Mother - Deceased
§
Family Member*:
n
*Please indicate thefamily member affected: mother, father, brother, sister, maternal or paternalgrandmother/grandfather, etc.
Jefferson»
University Physicians
Medical History Questionnaire
Social History:
Marital Status:
D Married
(check all that apply):
D Alcohol Use
Q Drug Use (Recreational)
Q Using Intravenous Drugs
Q Single D Widowed D Separated Q Divorced D Life Partner
Weekly:
Explain:
Explain:
] Previous History of Smoking
Date Quit:
Packs Per Day:
Years of Smoking:
Attempts to Quit:
Methods Used to Quit
o History of Smoking
Q Wishing to Stop Smoking
J Chewing Tdbaceo
Q Smoking/Nicotine Substances QCigarettesQ Cigars
Years:
Packs/Times Per Day:
I Current Diet
Explain:
Exercise Habits
Times per week:
| Being Sedentary (Do not exercise)
I Sexually Active
| Occupation
List All:
Travel
If recently out of the country, where?
Q Pipe
Do you have an advanced directive? tU Yes O No
Allergies
Reaction
Allergy
Medications Include vitamins, herbal supplements and over the counter medications:
Reason for Taking
Medications
Frequency
Dosage
Have you participated in any clinical trials or used experimental drugs? f~l Yes l~1 No Explain:
Are you pregnant?
CD Yes O No
Last Menstrual Period Date:
Is there anything else about your medical history that we should know?
Patient Signature:
Date:
I certify that I have reviewed the above information with the patient.
Physician Signature:
Date:
Jefferson*
University Physicians
voiding, and begin your reeordwith the first voiding upon arising as in the sample below.
1. Record fime of aMvoidings, leakage, intake of Squids.
-
2,. M|asu£4ft|j^^
s
3. r^^T*acth%:youw«rej«lf^ingat
record whetheryouwere sitting, standing, or lying down.
4T^mateithe^nlb^
:
1 = dampi few drops only
,
-• 2° wet underwear or pad
,
•'_ 3 -soakedor emptied bladder
. 5. .If ^^«Mt^:a§eo!tpjtenfed (orprec^ted) the urine leakage, write YES. If you felt no urge when the|eakage occurred, writ? NO.
• 6. Reii^thearnoirtand^
-;
:
Voiding Diary (continued)
Time
Form S07ft*S (tev. 02V4)
| Amount Voided
Activity
Leak Volume
Urge Present
Amount/Type of Intake
Jefferson™
University Physicians
of Life and Symptoms Distress inventory
Date
Name
Please^answer each'question bycheddngHhebest response between 0 (not at all) and 3 (greatly).
Incontinence Impact Questionnaire
0 = not at all
Has urinary leakage and/or prolapse affected youn
1= slightly
2 = moderately
3 = greatly
1. Ability to ^household chores (cooking.
housedeanTng; laundry)?
2. Phys^refreatior>suchasi«alking,svwmmJng,
or other exercise?
PA
'• ; •
—±
PA
.
T
3. Entertainment activities (movies, concerts, etc)?
4. Ability to travel by car or bus more than 30 minutes
fromfwme?
T
SR
5 Participation in social acCvities outside your home?
.
EH
6. Emotional heafth (nervousness, depression, etc)?
EH
7. Feeling frustrated?
- ,
'mMi^a^^^K^m
at all
1= slightly
2 = moderately
"i3^gi»?tiy;;;;;y: :VI: '-•'.
c-l ; " "'"
.v2p93rfeje^^
i"-S
;;£;
i*?*^ip!|
^5e :
:^£-l!J^^
(^OD
5. DjfficS^mp^ingyourtladder?
6: paTi^or4$comf6rtinflieJovver abdominal or
'
-?PP;:V
yc^:;;;
5, Buying oc'pietr(3slooyDO=can5ee mine
'
"
"•
' --••'
$fc '
~
socral/refetioqsfM^Bj
Off =-obstn»ctive/3iscornfort symptoms; 4«irritative:syri^brrB^S
K 08.1959
For* SOW-MS <R«OJ09
Jefferson Woman's Medical Specialties Center
University Physicians
T 215.955.5000
PHARMACY INFORMATION
Patient Name:
Please complete your pharmacy information below.
Retail Pharmacy
Name:
Address:
City, State:
Phone:
Fax:
Mail Order Pharmacy
Name:
Address:
City, State:
Phone:
Fax:
834 Chestnut Street, Ben Franklin House, Suite 300, Philadelphia, PA 19107-5127
THOMAS IEBPPP«r»N ITTNTVniJc
F 215.923.1089
Internal Communications
sP" ^^P^ """y^ —* T ~ <c~'—'—
lSiive*$lty Piiyskiam
Jtaiary22, 2013
Dear Patient,
Please be advised that effective January 1, 2012, Jefferson
University Physicians began charging a fee to patients that
request a copy of their medical records. Hie fees below are
to 20 l:iallowable amounts approved by the
of
Pennsylvania, Please note that Hie fees are updated
annually and are subject to change.
$1.42 per page for the first 20 pages.
$ 1.05 per page for pages 21 -60
$0.35 per page for pages over 61
Actual postage amounts will also be charged for the
mailing of the records.
Just as a reminder, a completed JtIP medical records
release form must be on file.
If you have any questions please contact Jefferson
University Physicians Central Medical Records at
S768.
Thankyou.
Dear Patient:
The state of Jefferson Center for Women's Medical Specialties will be glad to help you with the
completion of various forms, which may be necessary to assist you with your healthcare. Examples of
these forms are:
> Disability Forms
> FMLA Forms
> Insurance Forms
Please be advised: You will be charged a $10.00 fee for each form that is submitted to our office for
completion. This fee is not covered by insurance and is completely separate from any
co-pay or coinsurance. Payment will be expected prior to your receipt of the
completed form(s).
You will have the option to pay with cash or a check.
We appreciate your understanding and thank you in advance for your cooperation.
Sincerely,
Jefferson Center for Women's Medical Specialties
|£3iTT£>'t*O/~y|'J
,
University Physicians
Jefferson Woman's Medical Specialties Center
T 215.955.5000 F 215.923.W89
Discounted Parking is available to our
patients in the Ben Franklin parking lot,
i.L
located on Sansom Street between 8 and
th
9 Streets. The discounted rate is
$14.00/day. Please see our front desk staff
for a stamp to validate your parking
discount.
Discounted parking is also available at the
Central Parking lot on Market Street
between 8th and 9th Streets. Our front desk
staff is happy to provide a discounted
parking coupon.
Thank you
834 Chestnut Street, Ben Franklin House, Suite 300, Philadelphia, PA 19107-5127
THOMAS fEFFERSON UNIVERSITY