Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
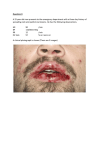
self-study course 2014 course four The Ohio State University College of Dentistry is a recognized provider for ADA, CERP, and AGD Fellowship, Mastership and Maintenance credit. ADA CERP is a service of the American Dental Association to assist dental professionals in identifying quality providers of continuing dental education. ADA CERP does not approve or endorse individual courses or instructors, nor does it imply acceptance of credit hours by boards of dentistry. Concerns or complaints about a CE provider may be directed to the provider or to ADA CERP at www.ada.org/goto/cerp. The Ohio State University College of Dentistry is approved by the Ohio State Dental Board as a permanent sponsor of continuing dental education ABOUT this COURSE… contact us phone 614-292-6737 READ the MATERIALS. Read and review the course materials. COMPLETE the TEST. Answer the eight question test. A total of 6/8 questions must be answered correctly for credit. SUBMIT the ANSWER FORM ONLINE. You MUST submit your answers ONLINE at: Who can earn FREE CE credits? A: EVERYONE - All dental professionals in your office may earn free CE credits. Each person must read the course materials and submit an online answer form independently. Q: What if I did not receive a confirmation ID? A: Once you have fully completed your answer form and click “submit” you will be directed to a page with a unique confirmation ID. RECORD or PRINT THE CONFIRMATION ID This unique ID is displayed upon successful submission of your answer form. Q: Where can I find my SMS number? A: Your SMS number can be found in the upper right hand corner of your monthly reports, or, imprinted on the back of your test envelopes. The SMS number is the account number for your office only, and is the same for everyone in the office. Q: How often are these courses available? A: FOUR TIMES PER YEAR (8 CE credits). ABOUT your FREE CE… fax 614-292-8752 web www.dent.osu.edu/ sterilization Q: http://dent.osu.edu/sterilization/ce toll free 1-888-476-7678 e-mail [email protected] FREQUENTLY asked QUESTIONS… TWO CREDIT HOURS are issued for successful completion of this selfstudy course for the OSDB 2014-2015 biennium totals. CERTIFICATE of COMPLETION is used to document your CE credit and is mailed to your office. ALLOW 2 WEEKS for processing and mailing of your certificate. Page 1 2014 course four WHITE LESIONS OF THE ORAL CAVITY This course will help dental professionals familiarize themselves with common white lesions of the oral cavity and derive a differential diagnosis for various white lesions. INTRODUCTION White lesions of the oral cavity are one of the leading reasons for which patients seek professional treatment. These lesions can have a wide spectrum of diagnoses including infectious, reactive, immune-mediated, premalignant, and malignant conditions. Patient history, clinical presentation, and location can be very helpful in narrowing down the differential diagnosis of these various white lesions. INFECTIOUS WHITE LESIONS CANDIDIASIS written by neetha santosh, dds edited by rachel a. flad, bs karen k. daw, mba, cecm evan miller Candidiasis is the most prevalent oral fungal infection in humans. Candida Albicans, part of the normal oral micro flora, is the causative organism. A complex interaction of immune status and mucosal environment of the host and strain of C. Albicans controls the presence of candidal infection. Various predisposing factors for oral candidiasis include use of dentures, xerostomia, recent broad-spectrum antibiotic therapy, corticosteroid use (aerosolized inhalants or topical creams/gel), and immunodeficiency (HIV infection or leukemia). Clinical Features: The clinical features of candidiasis can vary from superficial involvement of oral mucosa in Pseudomembranous Candidiasis Dr. Carl Allen, The Ohio State University College of Dentistry immunocompetent individuals to disseminated infection in immunosuppressed patients. A variety of clinical forms of oral candidiasis exist, including: Pseudomembranous Erythematous Hyperplastic Mucocutaneous Among these, the two clinical forms which appear white are pseudomembranous and hyperplastic candidiasis. Pseudomembranous candidiasis appears clinically as creamy, white plaque (similar to cottage cheese or curdled milk) and is usually present on the buccal mucosa, tongue, and palate. This plaque can be removed by scraping or wiping, which leaves an intact normal or reddened underlying mucosa. Diagnosis of alternative white lesions such as lichen planus should be considered if the mucosa bleeds while scraping the p l aqu e . T he pa t i e nt s w i t h pseudomembranous candidiasis usually complain of mild burning sensation or bad taste. The diagnosis is usually established by Page 2 the relevant history of predisposing factors and typical clinical appearance. Isolation and identification of candidal hyphae or yeasts by exfoliative cytology (smear), or, culture on Sabouraud’s agar slant (swab) can confirm the diagnosis. Hyperplastic candidiasis presents as a white plaque that cannot be removed by scraping or wiping. It is most often present on the anterior buccal mucosa near the commissures, as well as on the tongue and lips. Hyperplastic candidiasis cannot be clinically distinguished from routine leukoplakia. The diagnosis is established by the identification of candida by a cytologic smear or culture and by total disappearance of plaque following antifungal treatment. A biopsy of the area will be prudent if any white plaque has remained in order to rule out the presence of true leukoplakia. Care should be taken to avoid confusing coated/hairy tongue with candidiasis. Coated tongue is due to accumulation of keratin and bacteria on the dorsal surface of the tongue, resulting in a white and thickened appearance. Hairy tongue has a typical hair-like appearance due to elongation of and the keratin accumulation on the filiform papillae of the dorsal tongue. The diagnosis of coated/hairy tongue is distinguished by its characteristic clinical appearance. Scraping the tongue and improving oral hygiene is the recommended treatment. treatment regimen of patients with dentures. If there is no improvement post-treatment, biopsy of the area is recommended to exclude other possible conditions. A referral to the physician is also prudent to rule out underlying systemic disorders. ORAL HAIRY LEUKOPLAKIA Oral hairy leukoplakia is a lesion that occurs mainly in immunocompromised individuals, especially in AIDS patients. This lesion has also been described in patients experiencing extended corticosteroid therapy after organ transplantation or other systemic conditions. Epstein-Barr virus is the main causative organism of oral hairy leukoplakia. Clinical Features: Oral hairy leukoplakia typically presents as white vertical streaks or corrugated plaques on the lateral border of the tongue. This lesion is usually bilateral and can extend to the dorsal and lateral surfaces of the tongue, and can also rarely involve the buccal mucosa, soft palate, pharynx, and esophagus. Oral hairy leukoplakia does not rub off; differential diagnoses include hyperplastic candidiasis, true leukoplakia, proliferative verrucous leukoplakia, morsicatio linguarum (tongue chewing), and lichen planus. A definite diagnosis can be established by identification of Epstein-Barr virus within the lesion using in situ hybridization or by histopathological examination of the biopsied area. Treatment: Treatment: A variety of topical and systemic antifungal agents are available to treat oral candidiasis. Most of the patients respond well to the topical treatment which include Nystatin and Clotrimazole. The systemic drugs available are Ketoconazole, Fluconazole, and Itraconazole and are used usually for chronic or disseminated candidiasis. The recommended dosage of Clotrimazole is to dissolve 1 troche (10 mg) slowly in the mouth 5 times per day for 10 days. Nystatin oral suspension can be used by swishing 2-5 mL for tw o minu tes and sw allow ing the reafter . Disinfection of dentures by soaking them in 10% household bleach (complete dentures) or in Nystatin oral suspension (removable dentures with metal parts) should be included in the Usually, it is not necessary to treat oral hairy leukoplakia. There can be resolution of the lesion if the patient is on Highly Active Antiretroviral Therapy (HAART) for HIV infection. HIV patients diagnosed with oral hairy leukoplakia have higher chances of disease progression to AIDS. Since oral hairy leukoplakia is mostly seen in immunocompromised individuals, its occurrence in the absence of a known reason of immunosuppression warrants referral to a physician for a complete physical evaluation. Page 3 REACTIVE WHITE LESIONS LINEA ALBA appearance. Isolated lesions on the lateral border of the tongue without history of tongue chewing should be thoroughly evaluated to rule out HIVassociated oral hairy leukoplakia. Linea alba means “white line” in Latin and is one of the most common variations of the buccal mucosa. Pressure, frictional irritation, or sucking trauma from adjacent facial surfaces of the teeth are usually linked to this alteration. No treatment is usually required for morsicatio lesions. An oral acrylic shield may be fabricated to protect buccal and labial mucosa from chewing habits. Clinical Features: CHEMICAL INJURIES OF THE ORAL MUCOSA Linea alba typically presents as a bilateral white line on the buccal mucosa at the level of the occlusal plane. It can have a scalloped appearance and extend from the commissure to the posterior teeth. Prolonged periods of contact between various drugs and chemicals and the oral mucosa can cause temporary white lesions. Aspirin, hydrogen peroxide, silver nitrate, phenol, eugenol, formacresol, sodium hypochlorite, dental cavity varnishes, and acid etch materials are some of the most common drugs and chemicals that cause oral mucosa. These white lesions are due to epithelial necrosis and fibrinopurulent exudate from the chemical injury. Treatment: Diagnosis of linea alba is made by the characteristic clinical location and appearance, with biopsy not usually being necessary. Linea alba requires no treatment and it may disappear on its own in some individuals. MORSICATIO BUCCARUM (CHRONIC CHEEK CHEWING) White lesions can appear on the oral mucosa due to chronic cheek biting or sucking. These are most common on bilateral buccal mucosa (morsicatio buccarum) and are also present on the tongue (morsicatio linguarum) and lips (morsicatio labiorum). Clinical Features: Morsicatio lesions are often seen in people who have psychologic conditions or in those who are under stress. Women are twice as likely to be affected by these lesions. The lesions are frequently seen bilaterally on the anterior buccal mucosa along the occlusal plane and have a distinctive irregular and ragged appearance due to constant nibbling. Similar lesions can be present on the labial mucosa or lateral borders of the tongue. Treatment: Morsicatio lesions are diagnosed by the history of chewing habits and the typical ragged clinical Clinical Features: A brief exposure with chemicals causes the oral mucosa to appear white and wrinkled; prolonged exposure leads to epithelial necrosis and desquamation. Necrotic epithelium can be removed, which exposes erythematous underlying connective tissue and is later covered by a yellowish-white fibrinopurulent membrane. The injury to the mucosa can be very extensive depending upon the duration of exposure and concentration of the chemical. The attached mucosa is more resilient to the chemical injury compared to the unattached mucosa. Treatment: The ideal treatment of chemical injuries is carried out by preventing exposure of oral mucosa to potential caustic medications. If such medications have to be used, care should be taken to swallow the drug immediately to avoid any prolonged contact with oral mucosa. Children should be monitored as well. Healing occurs in superficial lesions within 1-2 weeks. Deep and extensive lesions may require surgical debridement and antibiotic therapy to quicken healing and prevent infection. Page 4 CONTACT STOMATITIS Treatment: A wide variety of agents including food, food additives, chewing gum, candy, oral hygiene products such as toothpaste and mouth washes, and dental treatment materials such as gloves and rubber dam materials, topical anesthetics, restorative materials, acrylic denture materials, dental impression materials, and denture adhesive preparations can cause allergic reactions in the oral cavity. If the patient stops the use of cinnamon flavored product or tartar-control toothpaste, lesions should resolve within a week. The lesions will reoccur within 24 hours if the patient reuses the product. A topical corticosteroid can provide faster recovery in some patients. Biopsy of the area will be prudent to rule out other conditions if contact stomatitis still persists after two weeks of discontinuation of the offending products. Clinical Features: FRICTIONAL KERATOSIS Contact stomatitis occurs more frequently in females and can be acute or chronic. Two commonly occurring contact stomatitis in oral mucosa are oral cinnamon reaction and toothpaste related sloughing. Frictional keratosis refers to a white patch on the oral mucosa due to constant mechanical irritation. Sources of mechanical irritation can be numerous including broken tooth cusps, sharp restorations, orthodontic brackets, and rough or ill-fitting dentures. Alveolar ridge keratosis is a form of frictional keratosis occurring on the crest of an edentulous ridge or retromolar pad area and results from chronic friction from dentures or mastication. Linea alba and morsicatio lesions can also be grouped under frictional keratotic conditions. Oral cinnamon reaction occurs due to the artificial cinnamon oil used as a flavoring agent in gum, candy, toothpaste, mouth washes, breath fresheners, soft drinks, processed meat, etc. Patients usually complain of pain and a burning sensation. Clinical presentation of oral cinnamon reaction varies depending upon the medium of delivery. While a diffuse reaction is seen with toothpaste containing artificial cinnamon flavoring, a more localized pattern occurs with chewing gum and candy. The buccal mucosa and the tongue are the frequent locations affected from chewing gum and candy. Oblong patches of reddened areas with overlying white, shaggy hyperkeratosis are observed on buccal mucosa along the occlusal plane. The tongue can also have a similar appearance involving the lateral border and dorsal surface. Diagnosis is often made by the clinical appearance and history of artificial cinnamon use. Differential diagnosis includes morsicatio lesions and oral hairy leukoplakia. Dentifrice sloughing is a reaction to certain ingredients in toothpaste, such as sodium lauryl sulfate, pyrophosphate (tartar-control agent), and artificial flavoring like cinnamon and mint. Diffuse erythema of the oral mucosa along with sloughing of superficial layers of epithelium is seen. Typical clinical appearance of string-like sloughed mucosa along with history of tartar-control or flavored tooth paste use is good enough to make a diagnosis. Clinical Features: Clinically, frictional keratosis can mimic true leukoplakia and is analogous to a callus on the skin. It appears as a rough hyperkeratotic area that usually blends into the adjacent normal mucosa and is seen frequently on the buccal mucosa, lateral borders of the tongue, and retromolar pad area. Treatment: The diagnosis of frictional keratosis is usually made by the clinical examination and evidence of a source of chronic irritation. Malignant transformation has not been reported in this condition. Frictional keratosis is usually treated by removing the offending agent. Smoothing a sharp tooth or restoration and correction of the illfitting denture can reduce the mechanical irritation on the mucosa. Ideally, the condition should disappear in two weeks after removing the irritating factor. If the lesion still persists, biopsy of the area is recommended to rule out true leukoplakia. Page 5 NICOTINE STOMATITIS Clinical Features: Nicotine stomatitis is a white lesion which is typically seen on the palate of pipe or cigar smokers. It is also known as smoker’s palate or nicotine palatinus. This condition has not been associated with malignant transformation and most likely is due to mucosal response to high heat associated with smoking. Interestingly, denture wearers who smoke do not have this condition because the upper denture usually protects the palatal mucosa from heat. People who drink very hot beverages have also reported similar lesions on the palate. Smokeless tobacco keratosis is usually asymptomatic and is identified during routine examination. Duration of the smokeless tobacco habit, brand and type of smokeless tobacco, length of daily use, and amount of tobacco used are some of the factors determining the development of this lesion. The mandibular vestibule is where the tobacco is most often in contact with the mucosa. Gingival recession with alveolar bone destruction in the area of tobacco contact may also be present. The mucosa appears grayish white and has a wrinkled appearance. The absence of tobacco in the mouth during clinical examination makes the stretched mucosa appear fissured, and a “pouch” (where the tobacco was kept) can be seen. People who chronically put materials such as hard candy, beef jerky, sunflower seeds, etc. in their vestibule can also develop similar mucosal changes. Typically, smokeless tobacco keratosis develops within 1 to 5 years of smokeless tobacco use. With chronic use in some individuals, the mucosa thickens to form a white leathery or nodular appearance. Clinical Features: Nicotine stomatitis is reported in patients above 45 years of age and the palatal mucosa being the characteristic location. The palatal mucosa appears white, while multiple raised papules with red centers are seen. The papules are inflamed salivary glands and the red centers represent inflamed openings of salivary gland ducts. The overall palatal mucosa has a dried mud appearance due to hyperkeratosis. Teeth with black tobacco stains are also evident, most of the time. Treatment: The diagnosis of nicotine stomatitis is established by the characteristic clinical presentation and correlation with the use of pipes or cigars or hot beverages. With smoking cessation, nicotine stomatitis is completely resolvable within 2 weeks. If the condition persists after 2 weeks of smoking cessation, biopsy of the area is mandatory to rule out true leukoplakia. Patients with nicotine stomatitis should also be thoroughly examined for tobacco-related changes such as true leukoplakia in the entire oral mucosa. Tobacco Pouch Keratosis Dr. Kristin McNamara, The Ohio State University College of Dentistry Treatment: SMOKELESS TOBACCO KERATOSIS Smokeless tobacco keratosis is a white fissured plaque seen on the oral mucosa in the area of direct contact with smokeless tobacco. It is also known as snuff pouch, snuff dipper’s lesion, tobacco pouch keratosis, and spit tobacco keratosis. Chewing tobacco, moist snuff, and dry snuff are the various types of smokeless tobacco prevalent in the United States. The history of placing smokeless tobacco in the altered mucosal site and the characteristic clinical presentation are all that is required to make the diagnosis. Mucosal alteration associated with chronic smokeless tobacco use should completely disappear within two weeks of habit cessation or alteration of the original site. Any lesions which persist after 6 weeks without smokeless tobacco Page 6 contact should be biopsied to rule out a true leukoplakia. Biopsy is also indicated for more severe lesions, which have leathery white plaques, verrucous appearance, ulceration, or hemorrhage. IMMUNE-MEDIATED WHITE LESIONS LICHEN PLANUS Lichen planus is one of the very common mucocutaneous disorders. Cutaneous lesions usually involve skin, nailS, and scalp, while mucosal lesions affect oral and genital mucosa. Cutaneous lesions are seen in 25-30% of individuals with oral lesions. The exact cause of this lesion is presently unknown and is most likely due to an autoimmune process. Clinical Features: Lichen planus is seen more commonly in middleaged women. Skin lesions are characterized by purple, pruritic, polygonal papules on the flexor surface of extremities. Fine, white interlacing lines called Wickham’s Striae are seen on the skin papules. Orally, the lesions are seen on bilateral buccal mucosa. Other sites such as the tongue, labial mucosa, gingiva, and palate can also be affected. The two forms of lichen planus seen in oral mucosa are reticular and erosive. Reticular lichen planus is more commonly presented than the erosive type. It is asymptomatic and usually affects the posterior buccal mucosa. It gets its name because of the typical pattern of interlacing white lines. These lesions may wax and wane very often. Lichen planus on the dorsal surface of the tongue does not have characteristic reticular white lines and instead manifests itself as smooth, white plaque with atrophy of papillae. Erosive lichen planus is a painful condition compared to the reticular type, causing patients to seek medical care frequently. The lesions usually present as reddened areas with ulceration on the bilateral buccal mucosa. The margins of the reddened area usually have white lace-like striae; the tongue and gingiva also can be affected. When only gingival mucosa is involved, the presentation is known as desquamative gingivitis and biopsy should be done to rule out mucous membrane pemphigoid and pemphigus vulgaris, since they have similar clinical features. Treatment: Diagnosis of reticular lichen planus is based on the clinical presentation. The classic lace-like pattern of reticular lichen planus can be obscured if there is co-infection with candidiasis. Treatment with antifungal therapy in such proven cases can reveal the classic reticular pattern following therapy. Once the diagnosis of reticular lichen planus is established, there is no need for any treatment, as it is asymptomatic. Reassuring the patient and periodic follow-up to monitor any clinical changes are all that is required. Erosive lichen planus is usually biopsied to get a histopathologic and immunofluorescent diagnosis in order to rule out chronic ulcerative stomatitis and systemic lupus erythematosus. Corticosteroids are used to provide relief to the patients. One of the recommended corticosteroids is Diprolene gel (betamethasone dipropionate gel 0.05%). The patient should apply a thin film to the affected area 4-6 times a day until the issue is resolved. It is important to exclude other lichenoid mucositis conditions such as lichenoid drug reaction, lichenoid amalgam reaction, and graftversus-host disease. LICHENOID MUCOSITIS Certain drugs, dental restorative materials such as amalgam, and artificial food flavoring can present similar histopathologic pattern as lichen planus. These immune-mediated reactions are classified as lichenoid drug reaction, lichenoid amalgam reaction, or oral cinnamon reaction, depending on the causative agent. These conditions should be separated from lichen planus as they are linked to a specific cause; they will be resolved if the causative agent is eliminated, whereas in lichen planus no specific causative factor has yet been identified. Page 7 Clinical Features: Lichenoid drug reaction usually presents as irregular erosions on the posterior buccal mucosa and lateral borders of the tongue. Clinically, these may resemble erosive lichen planus. There have been numerous prescription and over-the-counter drugs linked to lichenoid reaction. NSAIDs such as Ibuprofen, Naproxen and Fenclofenac, antihypertensives such as ACE inhibitors, Chlorothiazide and Propranolol, oral hypoglycemic agents such as chloropropamide and tolbutamide, antimicrobials such as amphotericin, ketoconazole, chloroquine, pencillamine, streptomycin, and tetracycline are few among the extensive list of medications which can cause lichenoid drug reaction. Lichenoid amalgam reaction affects the oral mucosa which comes in contact with amalgam restoration. White patches with radiating borders is the common clinical presentation. The altered mucosa will always be in contact with amalgam restoration of adjacent teeth. Buccal mucosa and lateral borders of the tongue are typical sites of occurrence. PREMALIGNANT WHITE LESIONS LEUKOPLAKIA Leukoplakia means “white patch” and is described by the World Health Organization (WHO) as “a white patch or plaque that cannot be characterized clinically or histopathologically as any other disease”. It is the most common precancerous lesion in the oral cavity. The term leukoplakia is a clinical description, and histopathologically it can include atypical oral epithelium, mild epithelial dysplasia, moderate epithelial dysplasia, severe epithelial dysplasia, and carcinoma-in-situ. Clinical diagnosis of leukoplakia should be rendered only after white lesions such as lichen planus, morsicatio lesions, frictional keratosis, tobacco pouch keratosis, nicotine stomatitis, leukoedema, and white sponge nevus are excluded by history, location, and clinical appearance. If in doubt, biopsy of the area is necessary to evaluate if there is any evidence of precancerous changes. Treatment: The diagnosis of lichenoid drug reaction is usually made by the history of offending drug usage and clinical presentation. Elimination of the suspected medication should result in complete disappearance of the lesion; however, reoccurrence can happen if the drug is consumed again. Temporary relief can be provided by application of corticosteroids on the affected area until the medication is completely eliminated from the body. Biopsy of the area is prudent if lesions persist after cessation of the suspected medication. Lichenoid amalgam reaction is diagnosed by the presence of an amalgam restoration in contact with altered mucosa. Removal of the adjacent amalgam and replacement of the filling by nonmetallic restorative materials can provide a complete resolution in two weeks. If the condition does not improve, biopsy of the area should be performed to exclude other possible conditions, such as true leukoplakia. Leukoplakia Dr. Kristin McNamara, The Ohio State University College of Dentistry Clinical Features: Leukoplakia tends to affect people above 40 years and has a stronger male predilection. Tobacco usage is the most common cause of leukoplakia. Alcohol use with tobacco and sanguinaria are among the other causative factors. Although most leukoplakic lesions are seen on buccal mucosa, lips, and gingiva, the lesions on the tongue and floor of the mouth often have precancerous or cancerous changes. Clinical presentations can Page 8 vary from person to person, along with time. The white patches may appear translucent or thin, homogenous or thick, granular or nodular, and verrucous. One of the most important features to look for is the sharply demarcated borders from the normal mucosa. Proliferative verrucous leukoplakia (PVL) is a type of leukoplakic lesion which is more aggressive than leukoplakia and has multiple leukoplakic patches in the oral cavity. PVL is more prevalent in women compared to men and they usually do not have a history of tobacco use. The mean age of occurrence of PVL for men is 50 years of age, and 65 years for women. The buccal mucosa (in women), the hard and soft palate, the alveolar mucosa, the tongue (in men), and the floor of the mouth are the common sites of occurrence. The process starts as a hyperkeratotic area and, with time, enlarges to form warty lesions and become multifocal. Treatment: Biopsy of leukoplakia is mandatory to obtain a histopathologic diagnosis because the treatment depends on the diagnosis. Small lesions can be removed completely by surgical excision and should be sent for histopathological analysis. Biopsy of multiple sites should be performed if the lesion is large. If there is epithelial dysplasia (especially moderate or severe) in a large lesion, complete removal should be done by surgical excision, cryosurgery, electrosurgery, or laser excision. The patient should be followed up periodically and should be biopsied if there is any clinical change or recurrence, as 35% of completely excised lesions can reoccur. PVL lesions should be monitored more vigorously as they have higher chances of having epithelial dysplasia and transformation into verrucous or squamous cell carcinoma. ACTINIC CHEILITIS Actinic cheilitis is a premalignant white lesion on lips due to prolonged sun exposure. A similar type of lesion that affects the sun exposed skin is called actinic keratosis. affected area of actinic cheilitis. It is seen usually in fair-skinned individuals older than 40 years old and who have a history of chronic skin exposure. Actinic cheilitis is normally presented as white patches on lips with loss of normal dermatoglyphics. Presence of scales and fissures are also common. Treatment: The main treatment for actinic cheilitis is surgical excision and submitting the tissue for histopathological diagnosis. The patient should be followed up periodically and should be rebiopsied if there is any clinical change or reoccurrence, as 35% of the lesions can undergo malignant transformation to squamous cell carcinoma. MALIGNANT WHITE LESIONS SQUAMOUS CELL CARCINOMA Over 90% of oral malignancies are squamous cell carcinoma. Tobacco smoking (with or without alcohol usage) is the causative factor associated with 75-80% of oral squamous cell carcinoma. The other 20-25% typically occurs on the lateral tongue of younger people and gingiva of older women, and are not linked with any risk factor. Clinical Features: Squamous cell carcinoma usually occurs in older adults and more commonly affects men. The lateral border and ventral surface of the tongue and floor of the mouth are the most frequently affected sites. It can be seen clinically in several forms such as exophytic fungating mass, endophytic ulceration, or as mixed red and white patches (early presentation). Surface ulceration, induration on palpation, and rolled borders are some of the common features of squamous cell carcinoma. This condition is asymptomatic in the beginning, which prolongs the time before seeking medical treatment. Sometimes the tumor can destroy the underlying bone and cause motheaten radiolucencies. Clinical Features: The lower vermilion zone of the lip is the most Page 9 Treatment: Biopsy is mandatory on all clinically suspicious lesions including non-healing ulcers of the oral cavity. After confirming the diagnosis of squamous cell carcinoma, wide surgical excision and/or radiation therapy are the first choices of treatment. Since most patients are diagnosed at the late stage, survival rates are very bad and metastasis to regional lymph nodes are very common. After treatment, patients should be followed-up periodically and should be re-biopsied if there is any clinical change or reoccurrence. squamous cell carcinoma. Post-treatment, patients should be followed-up regularly and should be re-biopsied if there is any clinical change or reoccurrence. CONCLUSION White lesions can have various clinical presentations, ranging from reactive to malignant conditions. A correct diagnosis of white lesions is very important as it can change previous treatment plans. Biopsy of the lesion and submission of the tissue for histopathological examination is mandatory if clinical diagnosis is in doubt. Patients with premalignant and malignant conditions should be referred to an oral and maxillofacial pathologist as they should be monitored regularly for any clinical change or reoccurrence. REFERENCES 1. Neville B, Damm D, Allen C, Bouqot J. Oral & Maxillofacial Pathology. 3rd ed. Philadelphia, PA: Saunders Company; 2009. Squamous Cell Carcinoma Dr. Neetha Santosh, The Ohio State University College of Dentistry 2. Greenberg M, Glick M, Ship J. Burket’s Oral Medicine. 11th ed. Hamilton, Ontario: BC Decker Inc.; 2008. VERRUCOUS CARCINOMA Verrucous carcinoma is a less aggressive type of squamous cell carcinoma. Smokeless tobacco use has been linked to the development of this carcinoma. Clinical Features: Verrucous carcinoma usually affects older men. The alveolar mucosa, hard palate, and buccal mucosa are the most frequently affected sites. It presents clinically as thick-white or mixed red and white plaques with wart-like surface proliferations. It is usually asymptomatic which prolongs the time before seeking medical treatment. Treatment: Wide surgical excision is the preferred choice of treatment of verrucous carcinoma. One-fourth of verrucous carcinoma can show areas of routine ABOUT THE AUTHOR NEETHA SANTOSH NEETHA SANTOSH GRADUATED SUMMA CUM LAUDE FROM CHRISTIAN DENTAL COLLEGE, INDIA; WHERE SHE FURTHER COMPLETED HER GENERAL PRACTICE RESIDENCY. SHE THEN PURSUED A POSTDOCTORAL FELLOWSHIP IN ORAL BIOLOGY AT INDIANA UNIVERSITY SCHOOL OF DENTISTRY. CURRENTLY, SHE IS DOING HER RESIDENCY IN ORAL AND MAXILLOFACIAL PATHOLOGY AT THE OHIO STATE UNIVERSITY. HER RESEARCH AT OSU PRIMARILY FOCUSES ON IDENTIFYING BIOMARKERS THAT CAN PREDICT THE PROGRESSION OF ORAL PREMALIGNANT LESIONS TO SQUAMOUS CELL CARCINOMA. HER FUTURE CAREER PLAN IS TO JOIN ACADEMICS WHERE SHE CAN TEACH AND PRACTICE ORAL AND MAXILLOFACIAL PATHOLOGY. NEETHA SANTOSH CAN BE CONTACTED AT [email protected]. Page 10 post-test instructions - answer each question ONLINE press “submit” record your confirmation id deadline is November 16, 2014 1 T F Erosive lichen planus is more painful than reticular lichen planus and often requires treatment. 2 T F The exact cause of lichenoid mucositis, like lichen planus, is unknown. F Oral hairy leukoplakia can be removed by scraping or wiping which leaves a normal or reddened underlying mucosa. SUBMIT ONLINE SUBMIT ONLINE 3 T 4 T F Proliferative verrucous leukoplakia is a more aggressive form of leukoplakia and needs to be monitored closely for malignant transformation. 5 T F Frictional keratosis has been observed to exhibit malignant transformation. 6 T F Actinic cheilitis is a premalignant lesion due to excessive tobacco use. F Smokeless tobacco keratosis should completely disappear within two weeks of habit cessation or alteration of the original site. F The ventral surface and lateral border of the tongue are the most common locations for oral squamous cell carcinoma. 7 8 T T director john r. kalmar, dmd, phd [email protected] assistant director karen k. daw, mba, cecm [email protected] channel coordinator rachel a. flad, bs [email protected] Page 11