Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
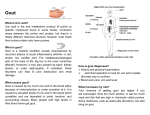
AD_ 0 2 1 _ _ _ AUG2 8 _ 0 9 . p d f Pa ge 2 1 2 0 / 8 / 0 9 , 2 : 5 1 PM HowtoTreat www.australiandoctor.com.au PULL-OUT SECTION inside COMPLETE HOW TO TREAT QUIZZES ONLINE (www.australiandoctor.com.au/cpd) to earn CPD or PDP points. Special considerations in the management of gout Pathophysiology of pseudogout Clinical presentation of pseudogout Diagnosis and treatment of pseudogout Authors’ case studies GOUT and other crystal arthropathies — Part 2 The authors DR CHANDI PERERA, consultant rheumatologist, Inflammatory Diseases Research Unit, school of medicine, University of NSW, and Sydney Adventist Hospital, Wahroonga, NSW. Last week, Part 1 of this series looked at the pathogenesis, clinical features, diagnosis and treatment of gout. This week, Part 2 concludes with a discussion of special considerations in the management of gout, and an overview of the pathophysiology, clinical presentation, diagnosis and treatment of calcium pyrophosphate dihydrate deposition disease (pseudogout). Special considerations in the management of gout Specialist referral for gout AN often-asked question is when to refer a patient with gout. Our opinion is that it is best to consider specialist referral in complex gout, poorly controlled disease, younger patients requiring further investigation, when there is doubt about the diagnosis, to reinforce lifestyle advice and, where required, to review ongoing management of uncomplicated gout. Special considerations Nephropathy Acute uric acid nephropathy is the single acute presentation of urate crystal deposition that needs urgent intervention. All other initial manifestations of renal crystal deposition disease are readily treatable. In patients with hyperuricaemia and renal disease who have bland urine sediment it is important to consider the possibility of lead toxicity as an alternative aetiology especially if hyperuricaemia is out of proportion to the degree of renal disease. Urolithiasis Increasing rates of urinary uric acid excretion are associated with a higher risk of uric acid and calcium oxalate stone formation. Uric acid calculi form about 20% of renal stones with approximately 80% of the stones occurring in males and a peak incidence in the sixth decade in both sexes. Most patients with urate stones do not have gout or hyperuricosuria. Fifty per cent of stone formers have diabetes or impaired glucose tolerance. Diagnosis is made by non-contrast helical computerised tomography. Pure uric acid calculi are radiolucent and often missed on conventional X-rays although stone analysis shows that some uric acid stones are partially composed of calcium oxalate. Treatment involves increasing alkalinisation of urinary pH usually using sodium bicarbonate and increasing urinary volume together with allopurinol to reduce excretion as recommended in the CARI (Caring for Australasians 12 with Renal Impairment) guidelines. Therapeutic failure in gout Non-compliance is an important but remediable cause of failure. It is a relatively common clinical problem due to a combination of factors including a natural history of self-limiting recurrences, therapeutic intolerance, its potential curability and lack of patient understanding of disease pathophysiology or appreciation of the need for www.australiandoctor.com.au long-term treatment. Usually the patient will have discontinued treatment due to lack of symptoms and over the years will have presented to several primary care physicians for treatment of acute episodes; and subsequently will have failed to follow up. Patient education at disease onset is arguably the single most important factor determining therapeutic success. Alcohol ingestion is an important part of the problem and needs to be clearly identified and broached at the time of instituting therapy. DR ANDREW BROOK, consultant rheumatologist and visiting medical officer, department of rheumatology, Canberra Hospital; and Canberra Rheumatology, Canberra, ACT. Emerging therapies for gout Febuxostat Febuxostat, a newer selective xanthine oxidase inhibitor (inhibiting both oxidised and reduced forms) represents an alternative to allopurinol for cont’d next page DR KATHIE TYMMS, consultant rheumatologist and visiting medical officer, department of rheumatology, Canberra Hospital; and Canberra Rheumatology, Canberra, ACT. 28 August 2009 | Australian Doctor | 21 AD_ 0 2 2 _ _ _ AUG2 8 _ 0 9 . p d f Pa ge 2 2 2 0 / 8 / 0 9 , 2 : 5 6 PM HOW TO TREAT Gout and other crystal arthropathies – Part 2 from previous page patients with gout. It is metabolised via hepatic conjugation and oxidation with less than 5% excreted unchanged by the kidney. No dose adjustment is required in patients with mild to moderate renal impairment. No clinically significant drug interactions were observed with colchicine, hydrochlorothiazide, indomethacin or warfarin. The Febuxostat versus Allopurinol Controlled Trial (FACT) demonstrated it was more efficacious at both 80mg and 120mg doses than the commonly used dose of allopurinol 300mg in meeting the primary endpoint (serum uric acid level of 13 <0.36mmol/L). While rates of flares on treatment after 52 weeks in all groups were similar, it remains unclear as to what the optimal dose of febuxostat is and if higher doses of allopurinol would be more effective than the doses of febuxostat used. Further safety and efficacy data, especially with respect to cardiovascular events and its usefulness in meta- bolic syndrome and hepatic and renal impairment, are needed. However, at first glance it offers a promising alternative to allopurinol-hypersensitivity patients on azathioprine or 6-mercaptopurine and a possible solution to the perennial problem of co-existing renal impairment. The long-term cost of treatment is likely to be a factor in uptake. Rasburicase Rasburicase is a recombinant preparation of urate-oxidase (uric- ase) synthesised from Aspergillus flavus that acts by converting uric acid to allantoin, an inactive and soluble uric acid metabolite with no effect on formation of uric acid. Currently rasburicase is used to prevent acute urate nephropathy precipitated by chemotherapy-induced tumour lysis in patients with leukaemia and lymphoma. It is of limited value in treating chronic gout largely due to a short half-life (approximately 18 hours), mode of administration (infusion) and potential immunogenicity. Pegloticase A pegylated mammalian recombinant uricase currently in phase III clinical trials, pegloticase has demonstrated rapid reduction of urate levels and in several cases tophus size during phase II development. It is likely to have a niche role in tophaceous gout, particularly when patients are intolerant or resistant to allopurinol. However further clinical studies need to confirm its efficacy across different populations. Pseudogout or CPPD-deposition disease PSEUDOGOUT is a crystal arthropathy associated with ageing. The term pseudogout describes an acute arthritis with characteristic calcifications in cartilage (chondrocalcinosis) and calcium pyrophosphate dihydrate (CPPD) crystals in the synovial fluid. The acute attacks of pseudogout, which are similar to those of gout, are followed by spontaneous resolution. Over time, recurrent episodes can result in chronic arthritis with degeneration of cartilage and bone. Joints commonly involved 22 The acute attacks of pseudogout, which are similar to those of gout, are followed by spontaneous resolution. | Australian Doctor | 28 August 2009 include the knees, wrists, shoulders, hips and ankles. Hyperparathyroidism, hereditary haemochromatosis, hypothyroidism and hypomagnesaemia are recognised metabolic associations. The diagnosis of pseudogout is established clinically and by demonstrating weakly positive bi-refringent crystals on polarised light microscopy with supporting radiographic features, which include chondrocalcinosis and the usual characteristic degenerative changes seen in osteoarthritis (including cartilage loss, subchondral cyst formation and osteophyte formation). Radiological features of pyrophosphate arthropathy overlap those of osteoarthritis; however, the pattern of joint involvement may help to discriminate it from primary osteoarthritis. Both conditions are common in the elderly and the role of each process in the pathogenesis of the other is uncertain, and it is important to consider both processes together rather than in isolation. The differential diagnosis for pseudogout includes gout, septic arthritis, inflammatory osteoarthritis, www.australiandoctor.com.au rheumatoid arthritis and, occasionally, spondyloarthropathy. Terminology Before further discussion there are a number of terms used that require clarification: • Pseudogout describes the clinical syndrome of acute arthritis associated with CPPD deposition in articular cartilage. • Chondrocalcinosis simply describes calcification of articular cartilage. • The term pyrophosphate arthropathy indicates structural abnormality of cartilage and bone associated with CPPD deposition. • CPPD-deposition disease is a term that seems to encompass both pseudogout and pyrophosphate arthropathy, although it is often loosely used as a synonym implying either or both of these conditions. Often confusion surrounding these terms stems from a combination of factors, including the coexistence of CPPD crystals in asymptomatic osteoarthritis, incidental chondrocalcinosis in osteoarthritis and loose use of terminology. AD_ 0 2 3 _ _ _ AUG2 8 _ 0 9 . p d f Pa ge 2 3 2 0 / 8 / 0 9 , 2 : 5 7 PM Epidemiology and aetiology of pseudogout Prevalence CPPD crystals formed induce an intra-articular acute inflammatory response, with neutrophil degranulation and release of reactive oxygen species, resulting in acute pseudogout. Recent findings suggest a crucial role for interleukin-1 in pseudogout, and may explain the success of treatment with anakinra, the interleukin-1 inhibitor, in resistant cases. WHILE the prevalence of CPPD-deposition disease is unclear and depends on the definition used, about 35% of patients presenting for total knee replacement for osteoarthritis have evidence of CPPD deposition. Framingham sub-cohort analysis showed an overall prevalence of 8% for chondrocalcinosis in the 6393 year age group, with the greatest prevalence in those 14 over 85 years. Increasing age seems to be the main risk factor for sporadic chondrocalcinosis. Genetics Scanning electron micrograph of calcium phosphate crystals on the surface of cartilage in a knee joint. Pathophysiology CPPD-deposition disease is a disorder of articular cartilage, associated with overproduction of inorganic pyrophosphates by chondrocytes. CPPD crystals and basic calcium phosphate ([BCP] carbonated-substituted hydroxyapatite, tricalcium phosphate and octacalcium phosphate) crystals are associated with CPPD-deposition disease. Both CPPD and BCP crystals increase in vitro chondrocyte mitogenesis, metalloproteinase elaboration and prostaglandin E2 production. Worsening osteoarthritis has been demonstrated after introduction of CPPD crystals in animal models, suggesting these crystals probably play a role in causing or accelerating degeneration of cartilage. BCP crystals have been demonstrated in patients with primary osteoarthritis. While BCP crystals seen in osteoarthritic joints lack clear radiological associations and are difficult to find in synovial fluid, these crystals are thought to be markers of severe osteoarthritis and have been proposed as potential therapeutic targets. However, symptomatic arthritis associated with BCP crystals, such as Milwaukee shoulder syndrome, is uncommon in patients under 60. While deposition of calcium-containing crystals can occur in most tissues, deposition is frequently intra-articu- lar and peri-articular. The exact mechanism of cartilage calcification is uncertain; it is thought to depend on concentrations of extracellular inorganic phosphate, pyrophosphate and calcium and soluble factors such as transforming growth factor-ß which modulate extracellular pyrophosphate. Excess extracellular pyrophosphate results in CPPD crystal deposition, a phenomenon that probably increases with ageing. While chondrocalcinosis may be sporadic, and uncommonly associated with some metabolic disorders, a rare familial predisposition has also been reported. No studies to date have quantified the different aetiologies and cases attributed to familial predisposition. Historically, scientific attention to a genetic link to calcium-crystal-related arthritis was first raised in a series of cases in the late 1950s; patients in this cohort presented by Sit’aj and Zitnan belonged to 15 five families. Familial inheritance is largely autosomal dominant and seems to have a relatively early initial clinical presentation. Using linkage analysis studies in families with CPPD arthropathy, loci have been identified on chromosome eight (CCAL1) and five, with that on 5p (CCAL2) considered to be particularly important, as it has been linked to disease phenotype in apparently unrelated families. However not all familial inheritance can be explained by these two genes, suggesting genetic loci heterogeneity even in so-called familial CPPD-deposition disease. A mutation of the ANKH gene (a transmembrane protein involved in inorganic phosphate transport) responsible for familial CPPD-deposition disease has been described 16 by Williams, et al. Patients with familial CPPD-deposition disease are likely to develop early and more aggressive disease. CPPD-deposition disease linked with metabolic associations tends to present at an earlier age. A familial form of chondrocalcinosis associated with diffuse idiopathic skeletal hyperostosis (DISH) has also been reported. cont’d next page PBS Information: Restricted Benefit. For use in patients that meet the criteria set out in the General Statement for Lipid-lowering Drugs. rosuvastatin DEMAND SUCCESS † †8 out of 10 patients achieve their LDL-C goal with CRESTOR 10 mg, in studies using ATP III goals: high risk <2.6 mmol/L; medium risk <3.4 mmol/L; low risk <4.1 mmol/L,1-6 NHF/CSANZ LDL-C target for high-risk CHD patients is 2.0 mmol/L, target for all other patients is LDL-C, 2.5 mmol/L.7 CRESTOR has a positive effect on HDL-C which is maintained across the dose range.1,8 Please review full Product Information before prescribing. Product Information is available on request from AstraZeneca. CRESTOR® (rosuvastatin calcium). Indications: As an adjunct to diet when the response to diet and exercise is inadequate for the treatment of hypercholesterolaemia (including familial hypercholesterolaemia). Contraindications: Known hypersensitivity to any of the ingredients; patients with active liver disease, or unexplained persistent elevations in serum transaminases; pregnancy and lactation; in women of childbearing potential, unless they are taking adequate contraceptive precautions; CRESTOR 40 mg is contraindicated in patients with pre-disposing factors for myopathy/rhabdomyolysis, including hypothyroidism, personal or family history of hereditary muscular disorders, previous history of muscular toxicity with another HMG-CoA reductase inhibitor or fibrate, alcohol abuse, situations where an increase in rosuvastatin plasma levels may occur, severe renal impairment (CrCl <30 mL/min), Asian patients, concomitant use of fibrates. Precautions: Liver effects; Myopathy/Rhabdomyolysis; Renal insufficiency; Hepatic dysfunction; Asian patients; Pregnancy (Category D); Lactation. Interactions: Warfarin and Other Coumarin Anticoagulants; Cyclosporin; Gemfibrozil; Antacids; Protease inhibitors. Adverse reactions (common): dizziness, constipation, nausea, abdominal pain, myalgia, asthenia, headache. For less common adverse reactions, see full PI. Dosage: The recommended starting dose is 5 mg or 10 mg once per day both in statin naïve patients and in those switched from another HMG-CoA reductase inhibitor. The choice of starting dose should take into account the individual patient’s cholesterol level, special patient populations and future cardiovascular risk as well as the potential risk for adverse reactions. A dose adjustment can be made after 4 weeks of therapy where necessary. The usual maximum dose of rosuvastatin is 20 mg once per day. A dose of 40 mg once per day should only be considered in patients who are still at high cardiovascular risk after their response to a dose of 20 mg once per day is assessed. This may particularly apply to patients with familial hypercholesterolaemia. It is recommended that the 40 mg dose is used only in patients in whom regular follow-up is planned. A dose of 40 mg must not be exceeded in any patient taking rosuvastatin. Specialist supervision should be considered when the dose is titrated to 40 mg. Date of TGA approval: 3 April 2009. PBS Dispensed Price: 5 mg $51.18; 10 mg $69.91; 20 mg $96.43; 40 mg $134.44. References: 1. Jones P, et al. Am J Cardiol 2003;92:152-160. 2. Schuster H, et al. Am Heart J 2004;147:705-712. 3. Davidson M, et al. Am J Cardiol 2002;89:268-275. 4. Olsson A, et al. Am Heart J 2002;144:1044-1051. 5. Shepherd J, et al. Am J Cardiol 2003;91(Suppl):11C-19C. 6. Stalenhoef A, et al. Eur Heart J 2005;26:2664-2672. 7. NHFA/CSANZ Position Statement on Lipid Management 2005. Heart, Lung and Circulation 2005;14:275-291. 8. CRESTOR Approved Product Information. AstraZeneca Pty Ltd. ABN 54 009 682 311. Alma Road, North Ryde NSW 2113. CRESTOR is a trademark of the AstraZeneca Group. Licensed from Shionogi & Co. Ltd, Osaka, Japan. 07/09 AZAE0810 CRE000085 AST1966/AD/CJB www.australiandoctor.com.au 28 August 2009 | Australian Doctor | 23 AD_ H0 2 4 _ _ _ AUG2 8 _ 0 9 . p d f Pa ge 2 4 2 0 / 8 / 0 9 , 2 : 5 8 PM HOW TO TREAT Gout and other crystal arthropathies – Part 2 Clinical presentation of pseudogout CPPD-DEPOSITION disease has a wide spectrum of intraarticular and extra-articular clinical manifestations, including monoarticular and polyarticular pseudogout, axial spinal inflammation and tenosynovitis. The knee joints are commonly affected, with the elbows, wrists, shoulders, hips and ankles also affected. Metacarpophalangeal (MCP) joints may also be involved. Direct joint trauma, stress response related to intercurrent illness, surgery and parenteral fluid administration leading to altered fluid-balance states will often precipitate the usually self-limiting acute episodes. A typical acute attack of pseudogout will reach its peak within 24 hours and usually resolve over 1-3 weeks. Clinical features are due to inflammation of the joint and may mimic the intensity of gout, with erythema, swelling, pain, loss of function and exquisite tenderness — hence the name pseudogout. Pseudogout may uncommonly present with systemic features, including fever, leukocytosis and elevated inflammatory markers more commonly seen in gout and infection, and in such cases it is important to exclude pos- sible sepsis. Elderly patients may present with delirium. Atypical presentations include neck pain and headache associated with fevers, and low-grade, diffuse, symmetrical polyarticular inflammation that may be mistaken for meningitis and rheumatoid arthritis, respectively. Occasionally a low-positive rheumatoid factor titre may further add to the confusion. A subgroup of patients presents with proximal inflammatory symptoms not unlike polymyalgia rheumatica. Features suggestive of CPPD arthritis in this group of patients include calcific tendinopathy, tibiofemoral osteoarthritis and ankle involvement. Reported cases of CPPDdeposition disease and hypomagnesaemia in patients with short bowel syndrome mean that primary-care physicians should be alert to this possibility. Chondrocalcinosis associated with metabolic disorders and familial chondrocalcinosis is uncommon but must be considered in patients presenting before age 55 or if there is widespread polyarticular chondrocalcinosis. Diagnosis of pseudogout WHEN there is clinical doubt about the diagnosis, demonstration of crystals by synovial fluid analysis is essential, as is the exclusion of infection. The presence of typical radiographic calcifications supports the diagnosis. Crystals show either no or weakly positive bi-refringence on polarised light microscopy and are often difficult to detect. Where the symptomatic joint distribution overlaps that of typical osteoarthritis, and in the absence of associated chondrocalcinosis and/or demonstrated crystals in synovial fluid, a diagnosis is made more difficult. The possibility of CPPD crystal deposition disease needs to be considered particularly when radiological features of osteoarthritis are evident in joints not commonly affected in primary osteoarthritis. While there is an established radiographic association between chondrocalcinosis and osteoarthritis, the absence of chondrocalcinosis does not exclude a clinical diagnosis of pseudogout. CPPD crystals seen in both pseudogout and asymptomatic osteoarthritic joints can also coexist with uric acid crystals and BCP crystals. The association between calcium crystals and osteoarthritis is complex, and direct correlation between chondrocalcinosis and car17 tilage loss is at best tenuous. Also, the presence of intracellular crystals in synovial fluid from the knee joint is not clearly associated with 18 inflammatory symptoms. The differential diagnosis of acute monoarticular pseudogout includes gout and septic arthritis. As mentioned above, chronic CPPD-deposition disease may be polyarticular or oligoarticular and is often mis- Table 5: Diseases associated with pseudogout • Haemochromatosis • Hypomagnesaemia • Hyperparathyroidism • Hypothyroidism • Wilson’s disease Table 6: Standard investigations Clinical features of pseudogout may include erythema, swelling, pain, loss of function and tenderness of the joint. Exclusion of infection is essential. taken for rheumatoid arthritis or primary generalised osteoarthritis; investigations are tailored to differentiate between pseudogout and these conditions. After a diagnosis of CPPD-deposition disease has been established, screening for associated conditions (table 5) should be undertaken. Investigations include: • Iron studies. • Calcium level. • Magnesium level. • Phosphate level. • Uric acid level. • Thyroid function tests. • Liver function tests. • Parathyroid hormone level. • Caeruloplasmin level (tables 6 and 7). Wilson’s disease and hypophosphatasia are unlikely to be associated with radiological chondrocalcinosis in people over 60. Likewise, manifestations of haemochromatotic iron overload are unlikely in a premenopausal woman. A high degree of clinical suspicion is required to diagnose haemochromatosis. Radiological assessment of pseudogout Most joints with radiological evidence of CPPD crystal deposition are asymptomatic, leading to the assertion that, unlike in gout, the exact role of imaging in CPPD-deposition disease is unclear. However plain radiography and ultrasonography remain important tools and assist in diagnosing these disorders. The typical appearance of CPPD crystal arthropathy on plain radiography is chondrocalcinosis, and is commonly seen in fibrocartilage of the knee, triangular ligament of the wrist and pubic symphysis. Degenerative changes of MCP joints and patellofemoral joints should raise suspicion of an associated CPPD crystal deposition arthropathy and its related metabolic associations. Squaring of bone ends and presence of hook-like osteophytes in MCP joints, particularly if involving the second and third, raises the possibility of haemochromatosis and associated CPPD arthropathy, while severe isolated patellofemoral jointspace degeneration may be seen in • Synovial fluid for crystals, Gram stain, microscopy for cells and culture and sensitivity • FBC • Urea, electrolytes, creatinine; LFTs; calcium, magnesium, phosphate • Uric acid • CRP, ESR • X-ray Table 7: Additional investigations • Iron studies • Parathyroid hormone • Thyroid function tests • Caeruloplasmin • Haemochromatosis gene studies • Blood cultures hyperparathyroidism with or without CPPD crystal deposition. Plain radiographic features of BCP crystal disease are non-specific, although plain X-rays are a useful tool for diagnosing acute calcific tendonitis. A radiological association between osteophyte burden and chondrocalcinosis has been noted. Calcification is often an incidental radiolog- ical feature noted in asymptomatic individuals, with no clear relationship to disease severity. Further evidence of a possible contributory role for CPPD crystals in the causation of degenerative changes of ‘pseudo-osteoarthritis’ accompanying CPPD crystal deposition is suggested by these changes accompanying chondrocalcinosis in joints such as MCP and wrist, and accompanying joints that are unusual sites for classic osteoarthritis. Recent advances in ultrasonography have improved diagnostic utility in CPPD arthropathy. Crystal deposits in articular cartilage, fibrocartilage and tendons produce intracartilage focal hyper-echoic signals on ultrasonography. Advances in resolution have resulted in appreciating differences between the patterns of articular cartilage crystal deposition in gout and CPPD arthropathy. At present, more work is underway to understand the predilection of different crystals for particular sites in articular cartilage. Ultrasound also has a useful role in therapy, to assist local injection in selected cases of calcific shoulder tendonitis. It is also fast emerging as a diagnostic tool to detect CPPD deposits that are too small to be visible on plain radiographs, such as those seen in peri-articular structures (enthesitis). CT imaging has a limited but useful role in assessing atypical presentations related to CPPD deposition, such as cervical canal stenosis and myelopathy caused by a retro-odontoid calcified mass lesion (the so-called ‘crowned dens syndrome’) presenting with acute neck pain. MRI is useful for assessing the uncommon cervical spinal canal compression due to CPPD deposition in the axial skeleton. Treatment of pseudogout NO available treatment is known to halt progression of CPPD-deposition disease. Treatment of acute pseudogout is similar to that of acute gout, with NSAIDs, glucocorticoids and colchicine. The principles governing use of NSAIDs and intraarticular and oral steroids are similar to those of gout management. In the event that NSAIDs are contraindicated, treatment with ACTH is an option used with variable success. Simple joint 24 aspiration has been shown to improve symptoms and, when feasible, should be undertaken for both diagnostic and therapeutic reasons. Treatment of any underlying metabolic condition is important and may reduce frequency of pseudogout attacks, but does not usually result in resolution of cartilage calcification. There is no equivalent to uricosuric therapy used in gout, and the difficulty is treating recurrent or chronic pseudogout. | Australian Doctor | 28 August 2009 For recurrent pseudogout, studies show that colchicine at a dose of 0.5mg twice daily has varying success as prophylactic treatment. Although the long-term safety of this approach is untested, the usual precautions relating to the use of colchicine apply. When gastrointestinal side effects prevail, particularly in elderly patients, a dose of 0.5mg orally once daily is proposed, although the value of lowdose therapy is uncertain. NSAIDs, are the usual pre- ferred option but should not be prescribed lightly, given known risks and usual comorbidities found in elderly patients with pseudogout. Resistant pseudogout is an uncommon entity and, as a general principle, in such cases it is important to revisit and review the diagnosis. In established resistant cases, systemic steroids are used for lack of a better option. Probenecid inhibits transforming growth factor-ßinduced extracellular www.australiandoctor.com.au pyrophosphate upregulation; this effect is independent of cell membrane injury or phosphodiesterase inhibition, suggesting a potential therapeutic role in CPPD disease. However, welldesigned randomised controlled trials are needed before probenecid becomes a mainstream therapeutic tool for managing particularly resistant pseudogout. A small study recommends 19 using methotrexate. Although a two-month lag between initiation of therapy and response was evident, this may be preferable to long-term steroid use. A case study has demonstrated a good response in a patient with resistant pseudogout and steroid-related side effects using anakinra, the 20 interleukin-1 inhibitor. The judicious principles used to determine individually tailored suitability for surgical intervention including joint replacement in osteoarthritis remain the same in pseudogout-related joint degeneration. AD_ 0 2 5 _ _ _ AUG2 8 _ 0 9 . p d f Pa ge 2 5 2 0 / 8 / 0 9 , 2 : 5 9 PM Haemochromatosis and CPPD-deposition arthropathy HAEMOCHROMATOSIS is a condition associated with CPPD-depositionrelated arthritis. While almost any joint can be involved and the entire spectrum of radiographic findings of CPPD-deposition disease may be seen in haemochromatosis, osteoarthritic changes of the second and third MCP joints are characteristic, and their presence should raise the possibility of haemochromatosis and associated CPPD-deposition disease. Stiffness, pain and bony swelling are more prominent than ‘boggy synovitis’. Osteophyte formation at MCP joints and chondrocalcinosis are notable radiological features. Late clinical features of iron overload include diabetes and other endocrine manifestations, liver disease, cardiomyopathy and increased skin pigmentation. Investigations include iron studies and relevant gene testing after counselling. Carefully monitored NSAID therapy for symptomatic arthritis remains the mainstay of treatment. The use of Investigations include iron studies and relevant gene testing after counselling. intra-articular and systemic steroids has a role, particularly if NSAIDs are unsuitable and in monoarticular presentations. Monitoring for and treating osteoporosis in haemochromatosis and iron overload is important and should not be overlooked. The two common genetic mutations found in haemochromatosis are C282Y and H63D. C282Y is more common in the Caucasian population, with about 11% carrying the gene, although H63D is seen in about 23% of the population worldwide. Summary The relationship between haemochromatosis variants and arthritic manifestations is inconsistent. Some studies have found no relationship between C282Y and selfreported rheumatological symptoms or chondrocalcinosis, while others report an association between C282Y and late-onset osteoarthritis and chondrocalcinosis. Heterozygosity for the C282Y gene mutation may be associated with an increased risk of late-onset osteoarthritis in patients over 65 years, but this finding needs substantiation by better-designed studies, as there are implications for directed therapy in such subgroups at risk for osteoarthritis. Younger individuals (under 65) homozygous for H63D present with polyarthralgia, chondrocalcinosis of the hips and knees and osteophytic joints of the hands with joint-space narrowing, while older compound heterozygotes (over 65) have more arthralgia, chondrocalcinosis of the hip and increased osteophyte burden in knee joints. CPPD-DEPOSITION disease and associated clinical manifestations encompassing pseudogout and pyrophosphate arthropathy should be considered in patients presenting with clinical features mimicking gout, inflammatory osteoarthritis, septic arthritis and rheumatoid arthritis, especially in the elderly. Chondrocalcinosis associated with a metabolic disorder tends to present at an earlier age. cont’d next page Nasal and ocular symptom relief for patients suffering from allergic rhinitis1,2 Please Review Product Information before prescribing Indications: Treatment of seasonal allergic rhinitis and perennial allergic rhinitis in adults and children aged 2 years and older. Contraindications: Hypersensitivity. Precautions: Avamys should hould be used with caution in patients with seve severe liver disease. Infection of nasal airways should be treated and healing following nasal surgery should have occurred before use. Class effect: rare instances of glaucoma, increased intra-ocular pressure and nasopharyngeal candidiasis. Special care should be taken with patients who may be susceptible to candida infections (e.g. diabetics). Excessive dosing may cause suppression of the HPA axis, reduction in bone density and growth retardation in adolescents and children. Children receiving prolonged treatment should have their height regularly monitored. Other precautions: pregnancy (category B3), lactation. For more details, refer to full PI. Interactions: There is no theoretical basis for anticipating interactions between Avamys and the cytochrome P450 mediated metabolism of other compounds at clinically relevant intranasal doses of Avamys. Based on data with another glucocorticoid metabolised by CYP3A4, co-administration with ritonavir is not recommended because of the potential risk of increased systemic exposure to Avamys. Adverse reactions:Very common: epistaxis, generally mild to moderate in intensity. Common: nasal ulceration. Post-marketing data; Rare: immune system disorders, hypersensitivity reactions including anaphylaxis, angioedema, rash, and urticaria.* Dosage: Avamys Nasal Spray is for administration by the intranasal route only. For full therapeutic benefit regular usage is recommended. Onset of action has been observed as early as 8 hours after administration. It may take several days of treatment to achieve maximum benefit.Adults/Adolescents (12 years and over):The recommended starting dosage is two sprays (27.5 mcg per spray) in each nostril once daily (total daily dose, 110 mcg). Once adequate control of symptoms is achieved, dose reduction to one spray in each nostril once daily (total daily dose, 55 mcg) may be effective for maintenance. Children (2 to 11 years of age):The recommended starting dosage is one spray (27.5 mcg per spray) in each nostril once daily (total daily dose, 55 mcg). Patients not adequately responding to one spray in each nostril once daily may use two sprays in each nostril once daily (total daily dose, 110 mcg). Once adequate control of symptoms is achieved, dose reduction to one spray in each nostril once daily (total daily dose, 55 mcg) is recommended. *Please note change in Product Information. Full product information is available from GlaxoSmithKline Australia Pty Ltd. 1061 Mountain Hwy, Boronia, Victoria, 3155. ABN 47 100 162 481. Avamys® is a registered trade mark of the GlaxoSmithKline group of companies. References: 1. Avamys Product Information; 2. Vasar M et al. Allergy Asthma Proc 2008; 29:313-321; PC0905044 GSKA 6/09 PBS Information: This product is not listed on the PBS www.australiandoctor.com.au 28 August 2009 | Australian Doctor | 25 AD_ 0 2 6 _ _ _ AUG2 8 _ 0 9 . p d f Pa ge 2 6 2 0 / 8 / 0 9 , 4 : 1 6 PM HOW TO TREAT Gout and other crystal arthropathies – Part 2 Authors’ case studies References and further reading Young man with podagra MR X, a 40-year-old man with a seven-year history of recurrent podagra, presented with three months of persistent pain in his wrists, elbows, knees and ankles with intermittent swelling and associated early morning stiffness lasting for about an hour. He had no recorded fevers, rigors or night sweats, no known nephrolithiasis or renal impairment and no recent diarrhoeal illness. There was a possible past history of connective tissue disorder with Raynaud’s phenomenon and an intermittent pruritic truncal rash. There were no known medication allergies. Family history His uncle may have had gout and his father had a myocardial infarction at age 60. Comorbidities • Gastro-oesophageal reflux disease treated with esomeprazole 40mg daily. • Hypertension treated with perindopril 5mg/indapamide 1.25mg daily. Examination Mr X looked well and was afebrile. His BP was 140/95mmHg, pulse rate 96 beats/minute and SaO2 94% (room air). He had a BMI of 29, with central adiposity. There was synovitis in both wrists, knees and ankles. There were effusions in the left knee and both ankles, with gouty tophi of the right elbow. Examination of the cardiovascular and respiratory systems was unremarkable. Investigations • White cell count (WCC) — 9 15.3 × 10 /L. • ESR — 136mm in 1 hour . • CRP — 221mg/L. • Rheumatoid factor — <10IU/L. • Serum creatinine — 168μmol/L (normal range 60-130μmol/L) (known to be 106μmol/L six months ago). • Serum urate — 628μmol/L (NR 260-440μmol/L). • Microscopy, culture and sensitivity (MCS) of joint aspirates (left knee × 2 and gouty tophus of right elbow aspirated) — WCC 6 >50,000 × 10 /L mainly neutrophils; Gram stain — no organisms seen; culture — no growth seen after one week; crystals — negatively bi-refringent needleshaped crystals seen. Management The diagnosis of gout was confirmed as above and the patient was educated about gout, its precipitants and curability. The possibility of the metabolic syndrome and its implications were raised in the context of his young age. 26 Treatment options were discussed taking into consideration his renal impairment and comorbidities. Further investigations revealed a raised LDL cholesterol, low HDL cholesterol and an elevated BSL. No secondary cause of hyperuricaemia was found. Prednisone was commenced at 10mg daily for three days, 7.5mg daily for five days, 5mg daily for 10 days, 2.5mg daily for one week and then ceased. Allopurinol 50mg daily was commenced while he was on prednisone 5mg daily (a week after symptoms had completely resolved). Serum creatinine was repeated fortnightly and Mr X was reviewed in the outpatient clinic after six weeks and at three-monthly intervals thereafter. Allopurinol was increased to 100mg daily at seven weeks and to 150mg daily at 12 weeks; serum creatinine was monitored at monthly intervals. He was referred to the diabetic clinic for a persistently elevated BSL and to a cardiologist for a cardiac risk assessment and management. Elderly patient with swollen joints • Hypercholesterolaemia (stable on treatment). Patient’s history of gout Crystal diagnosis was established 15 years ago; initially this was mono-articular (podagra), but in the last three years he had had polyarticular episodes. Since worsening of his CCF about two years ago, a concomitant increase and relative persistence of flares had been noted, that is, 3-4 episodes each year with episodes lasting progressively longer. Previously he had been taking allopurinol 300mg daily, but he was now taking 100mg daily due to worsening renal failure. Acute episodes had been treated with colchicine and an NSAID. He was aware of precipitants and abstained from alcohol. Medications • Ramipril 7.5mg mane. • Frusemide 40mg daily. • Aspirin 100mg daily. • Glyceryl trinitrate spray I-II sublingual prn. • Meloxicam 7.5mg daily. • Allopurinol 100mg daily. • Calcium 600mg daily. • Ostelin 1000 IU daily. • Simvastatin 20mg nocte. Mr Y, 80, presented to the emergency department in congestive cardiac failure (CCF), with widespread ischaemic changes on ECG, acute on chronic renal impairment, and a swollen left elbow with tophi and associated cellulitis, sepsis and confusion. There was a history of penicillin allergy (rash), but he had tolerated cephalexin in the past. Premorbidly he was independent and self-caring and lived with his wife of 52 years. His temperature was 38.7°C, BP 90/55mmHg and pulse was 108 beats/minute and regular (low volume). • FBC — Hb 100g/L, WCC — 9 20 × 10 /L with raised neutrophils • ESR — 80mm in 1 hour • CRP — 200mg/L • EUC — Na 134mmol/L, K 3.5mmol/L, HCO 317mmol/L, Cr 270μmol/L and U 24mmol/L • Raised CK and troponin • Cholestatic LFTs, raised serum uric acid • Positive blood cultures — Methicillin-sensitive Staphylococcus aureus • Chest X-ray – cardiomegaly and cardiac failure Past medical history Diagnosis • Ischaemic heart disease, mitral regurgitation and heart failure. • Renal failure and prostate cancer (stable on no treatment). • Gout (stable until two years ago). • Hypertension. Mr Y was diagnosed with polyarticular gout worsening due to renal impairment and increased diuretic therapy. | Australian Doctor | 28 August 2009 Investigations Treatment Mr Y was admitted to the coronary care unit for monitoring and treatment of CCF and acute coronary syndrome; the ACE inhibitor and meloxicam were ceased and frusemide was increased to 80mg mane and 40mg midi; he was rehydrated gently (monitoring fluid balance) and commenced on cephazolin, and infectious disease and renal colleagues were consulted. Progress (day 7) Mr Y was afebrile on cephazolin and his cardiac failure stable. Coronary angiogram revealed triple vessel disease. While the cellulitis had largely resolved, he still had a painful, swollen left elbow and had developed painful, swollen hands and ankles in the last two days. Blood cultures were negative and transthoracic echocardiogram was negative for subacute bacterial endocarditis. He also complained of painful and burning soles and was unable to mobilise. A rheumatology consult was requested. Treatment of gout He was commenced on 10mg prednisone daily for three days, reducing to 7.5mg daily for one week and 5mg daily for one week with clear improvement of symptoms noted within 48 hours; prednisone was continued at a dose of 2.5 mg daily for a further three weeks without complications. His left elbow joint was aspirated for symptomatic relief (uric acid crystals seen on microscopy). Three months later Mr Y had completed six weeks (total) of antibiotics and while on 2.5mg prednisone daily his allopurinol was increased to 150mg daily following discussion with his renal physician. His prednisone was stopped a month later with no immediate flare. Older man with painful hands MR H, a 65-year-old retiree, presented for further management of his osteoarthritis, which was interfering www.australiandoctor.com.au with his golf, tennis and jogging. He had had painful hands for the past five years, with bilateral involvement of the first carpometacarpal (CMC) joints at onset and gradual swelling of the second, third and fourth MCP joints, second and fourth distal interphalangeal (DIP) joints and both wrists, which occasionally became very painful with swelling lasting for three days. He also had had mechanical knee pain and mild loss in range of movement of the knee joint, with more recent self-limiting episodes of pain and swelling. Mr H was an active and fit man who lived with his partner. He was a nonsmoker and consumed 10g of alcohol every second day. He had no known medication allergies. Mr H’s past history was of rheumatic fever at age seven years, hypertension and a duodenal ulcer. There was a strong family history of ischaemic heart disease and diabetes mellitus. Examination revealed osteoarthritic changes of the joints of the hands, with prominent second and third MCP joints, due to bony swelling, but no active synovitis. X-rays of the knees in 1989, 1994 and 2003 showed tri-compartmental osteoarthritis with chondrocalcinosis. X-rays of the hands and wrists in 2000 showed a calcified triangular ligament and bilateral degenerative changes of the first, second and third MCP joints with hook-osteophyte formation. FBC and inflammatory markers were normal, as were urea, electrolytes, creatinine, LFTs, blood glucose level, calcium, magnesium, phosphate, uric acid, TSH and parathyroid hormone levels. However, iron studies showed a transferrin saturation of 70% and an elevated ferritin level of 600μg/L. Mr H’s diagnosis was haemochromatosis with chondrocalcinosis and pseudogout. Subsequent gene studies demonstrated that he was homozygous for C282Y. Management consisted of venesection and monitoring iron studies. Arthritic flares were treated with NSAID, proton-pump inhibitor therapy and intra-articular and systemic steroids. Mr H also received physiotherapy for patellofemoral symptoms. He was screened for osteoporosis because treatment for this — particularly in advanced haemochromatosis — is important, but no intervention was required. His family were counselled and genetic screening of children was advised. Available on request from julian.mcallan@reedbusiness .com.au Online resources Australian Rheumatology Association: www.rheumatology.org.au cont’d page 28 AD_ 0 2 8 _ _ _ AUG2 8 _ 0 9 . p d f Pa ge 2 8 2 0 / 8 / 0 9 , 3 : 0 1 PM HOW TO TREAT Gout and other crystal arthropathies – Part 2 GP’s contribution DR MARG TAIT Picnic Point, NSW Case study A 67-YEAR-old man presented with painful swelling of his left hand consistent with synovitis. He had a background of gastro-oesophageal reflux disease, ischaemic heart disease, hypertension, L5 decompression surgery and bilateral knee replacements. He was commenced on meloxicam 7.5mg daily. Two days later the hand was worse and he reported that he had sustained a penetrating injury to his hand shortly after the initial consultation. Cephalexin 1g qid was commenced but after 48 hours there was little change and he was referred to ambu- latory care for IV antibiotics. A few days later he was admitted for management of possible septic arthritis of his right hand following an infection associated with the cannulation. The infection settled but bilateral synovitis persisted in the wrists and MCP joints. He was tried on a COX-2 inhibitor with no effect. Seven weeks after his presentation and when the ESR and CRP had returned to normal, prednisone 5mg bd was commenced with good effect, as well as colchicine 0.5mg bd. X-ray of the left wrist demonstrated marked changes of osteoarthritis in CMC and MCP joints as well as chondrocalcinosis of the triradiate cartilage. There was no erosive arthropathy. Other X-rays showed widespread and advanced osteoarthritis complicating underlying chondrocalcinosis. Serum calcium and parathyroid hormone levels were normal. Serum uric acid was 0.45mmol/L and rheumatoid ration unless there is unstable coagulopathy, overlying skin infection (cellulitic) or a prosthetic joint. It is reasonable to perform joint aspiration to confirm the diagnosis and inject steroid for symptomatic relief. factor was mildly positive. Iron studies were normal as was a TSH level. Steroids were withdrawn and colchicine ceased with time. There has been no recurrence for three years. Questions for the authors This patient is now warfarinised. If he developed painful acute swelling of his knee, would you aspirate his knee joint to exclude infection, confirm diagnosis and inject steroids? Anticoagulation is not a contraindication to joint aspi- How to Treat Quiz How often is the synovitis bilateral? In pseudogout bilateral synovitis is not uncommon, especially of the wrists although a relapsing pattern, that is, one wrist followed by the other is also commonly seen, as is monoarthritis. Symmetrical synovitis of the MCP joints of the hands is unusual and seronegative rheumatoid arthritis needs to be considered. General questions for the authors How is the diagnosis of pseudogout affecting the Achilles tendon made and how does the treatment differ from that of a joint affected by pseudogout? Calcaneal tendon calcifications are frequently seen in asymptomatic chondrocalcinosis. Ultrasound scanning and power Doppler studies correlate well with conventional radiography in depicting calcifications. Ultrasound scanning is useful at detecting early calcification which may have a normal appearance on conventional X-ray. Inflammatory changes of calcaneal soft tissues are frequently demonstrated by ultrasound and power Doppler studies in patients with CPPD-deposition-related tendonitis and in this setting ultrasound and power Doppler studies may 1 be more useful. The diagnosis of enthesopathy associated with CPPDdeposition disease in a younger age group should also include consideration of an associated metabolic disorder and requires appropriate investigation if clinically indicated. The treatment of CPPDrelated enthesopathy is diffi- cult. NSAIDs, corticosteroid injections and rarely colchicine have been used to treat acute presentations. Should all patients with X-ray changes be investigated further for the disorders associated with chondrocalcinosis, or only those under 55 years or with polyarticular chondrocalcinosis? I think it is reasonable to investigate confirmed or suspected cases of pseudogout for metabolic associations especially in a younger age group and polyarticular presentations; however extensive investigation of age-appropriate sporadic monoarticular presentations with no other clinical findings is less likely to yield similar associations. In acute presentations of either scenario one should aim to establish a crystal-based diagnosis of pseudogout. Reference 1. Journal of Rheumatology 2004; 31:2242-50. INSTRUCTIONS Complete this quiz online and fill in the GP evaluation form to earn 2 CPD or PDP points. We no longer accept quizzes by post or fax. The mark required to obtain points is 80%. Please note that some questions have more than one correct answer. Gout and other crystal arthropathies — Part 2 — 28 August 2009 1. Which THREE statements about the terminology surrounding calcium pyrophosphate dihydrate (CPPD) deposition disease are correct? a) Chondrocalcinosis describes deposition of CPPD crystals in articular cartilage b) Pseudogout describes the clinical syndrome of acute arthritis associated with CPPD deposition in articular cartilage c) Pyrophosphate arthropathy indicates structural abnormality of cartilage and bone associated with CPPD deposition d) CPPD-deposition disease is often used as a synonym for pseudogout 2. Which TWO statements about the epidemiology and aetiology of CPPDdeposition disease are correct? a) A rare familial predisposition to CPPDdeposition disease has been reported, however most cases are sporadic b) Familial inheritance of CPPD-deposition disease is largely autosomal recessive c) Patients with familial CPPD-deposition disease are likely to have milder disease d) CPPD-deposition disease linked with metabolic associations tends to present at an earlier age 3. Which THREE statements about the pathophysiology of CPPD-deposition disease are correct? a) CPPD-deposition disease is associated with overproduction of inorganic pyrophosphates by chondrocytes b) Excess extracellular pyrophosphate resulting in CPPD crystal deposition probably increases with ageing c) There is no association between basic calcium phosphate (BCP) crystals and CPPD-deposition disease d) CPPD crystals induce an intra-articular acute inflammatory response, resulting in acute pseudogout 4. Which TWO statements about clinical features of CPPD-deposition disease are correct? a) CPPD-deposition disease has a wide spectrum of intra-articular and extraarticular clinical manifestations b) An acute attack of pseudogout will typically resolve over 1-3 weeks c) Episodes of pseudogout can be distinguished from acute gout by the absence of erythema d) Polyarticular inflammation excludes a diagnosis of pseudogout 5. Which TWO statements about presentation of CPPD-deposition disease are correct? a) CPPD-deposition disease commonly affects the knee joints b) Wrists, elbows, shoulders, hips and ankles are rarely affected in CPPD-deposition disease c) Elderly patients with pseudogout may present with delirium d) Pseudogout does not produce an increase ONLINE ONLY www.australiandoctor.com.au/cpd/ for immediate feedback in the white blood cell count or inflammatory markers 6. Which TWO of the following conditions may be associated with CPPD-deposition disease? a) Haemochromatosis b) Hyperparathyroidism c) Hyperthyroidism d) Hypermagnesaemia 7. Which TWO statements about diagnosis of CPPD-deposition disease are correct? a) The diagnosis of pseudogout is established clinically and by demonstrating CPPD crystals on synovial fluid analysis with supporting radiographic features b) In CPPD-deposition disease, crystals are negatively bi-refringent on polarised light microscopy c) In pseudogout, crystals are very easy to detect on synovial fluid analysis d) In pseudogout, CPPD crystals can coexist with uric acid crystals 8. Which THREE statements about the radiological assessment of CPPDdeposition disease are correct? a) The typical appearance of CPPD crystal arthropathy on plain radiography is chondrocalcinosis b) Chondrocalcinosis is commonly seen in fibrocartilage of the knee, triangular ligament of the wrist and the pubic symphysis c) Radiological features of pyrophosphate arthropathy overlap those of osteoarthritis d) There is no role for ultrasound in CPPDdeposition disease 9. Which TWO statements about treatment of CPPD-deposition disease are correct? a) Treatment of acute pseudogout is similar to that of acute gout b) For recurrent pseudogout, prophylaxis with low-dose colchicine may be tried, however the long-term safety of this approach is uncertain c) Pseudogout that is resistant to therapy is common d) Treatment of any underlying metabolic condition does not have any effect on the frequency of pseudogout attacks 10. Which THREE statements about haemochromatosis and CPPD-deposition arthropathy are correct? a) Osteoarthritic changes of the second and third MCP joints should prompt consideration of haemochromatosis and associated CPPD arthropathy b) In CPPD arthropathy associated with haemochromatosis, stiffness, pain and bony swelling are more prominent than ‘boggy synovitis’ c) Patients with confirmed haemochromatosis should be monitored for osteoporosis d) Studies have shown consistent relationships between haemochromatosis variants and arthritic manifestations CPD QUIZ UPDATE The RACGP now requires that a brief GP evaluation form be completed with every quiz to obtain category 2 CPD or PDP points for the 2008-10 triennium. You can complete this online along with the quiz at www.australiandoctor.com.au. Because this is a requirement, we are no longer able to accept the quiz by post or fax. However, we have included the quiz questions here for those who like to prepare the answers before completing the quiz online. HOW TO TREAT Editor: Dr Wendy Morgan Co-ordinator: Julian McAllan Quiz: Dr Wendy Morgan NEXT WEEK Thyroid nodules are a very common finding in Australian adults. While most thyroid nodules are benign, about 5% of nodules coming to operation will be thyroid cancer. The next How to Treat gives an up-to-date account of the aetiology, assessment, diagnosis and treatment of thyroid nodules. The author is Professor Leigh Delbridge, professor of surgery, University of Sydney; visiting surgeon, Royal North Shore, Hornsby, Mater and North Shore Private Hospitals; honorary thyroid surgeon, The Children’s Hospital at Westmead, NSW; and president-elect of the International Association of Endocrine Surgeons. 28 | Australian Doctor | 28 August 2009 www.australiandoctor.com.au