Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
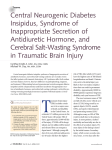
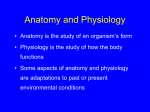
This material is protected by U.S. copyright law. Unauthorized reproduction is prohibited. To purchase quantity reprints, please e-mail [email protected] or to request permission to reproduce multiple copies, please e-mail [email protected]. ONLINE EXCLUSIVE • CONTINUING EDUCATION Syndrome of Inappropriate Antidiuretic Hormone Jo Ann Flounders, MSN, CRNP, OCN®, CHPN yndrome of inappropriate antidiuretic hormone (SIADH) is a disorder of water intoxication (Haapoja, 1997; Moses & Scheinman, 1991). SIADH describes the inappropriate production and secretion of antidiuretic hormone (ADH), also known as arginine vasopressin, that causes increased water reabsorption in the renal tubules and leads to increased water retention and dilutional hyponatremia (Finley, 1998; Keenan, 1999). S Etiology SIADH can occur as a result of an endocrine paraneoplastic syndrome, which implies that the syndrome is caused indirectly by a malignancy and not the direct result of invasion and damage by malignant cells (Haapoja, 1997; Keenan, 1999). An endocrine paraneoplastic syndrome occurs when a tumor secretes excessive amounts of hormones that interfere with normal homeostasis. Although normal hormone production occurs in response to a stimulus to maintain homeostasis, ectopic production of hormones by tumors is not normal and does not occur to maintain homeostasis. Tumor cells are able to produce many hormones and hormone-releasing factors, causing different paraneoplastic syndromes that affect body systems (Haapoja). The paraneoplastic syndrome of SIADH is caused by two mechanisms: the production of ADH by malignant tumor cells or the inappropriate production and release of ADH from the posterior pituitary gland (Finley, 1998; Haapoja; Keenan). Both mechanisms cause inappropriate and excessive secretion of ADH, which causes disruption of fluid balance (Bunn & Ridgway, 1993; Ezzone, 1999; Keenan). The most common etiology of SIADH is malignancy, although many other nonmalignant causes exist (Jones, 1999). The most frequent malignant cause of SIADH is small cell lung cancer (Flombaum, 2000; Keenan, 1999; List et al., 1986). Other malignant etiologic causes of SIADH include non-small cell lung cancer; head and neck, prostate, pancreatic, breast, ovarian, duodenal, and esophageal cancers; lymphoma and leukemia; and thymoma, neuroblastoma, and carcinoid tumors (Finley, 1998; Frizzell, 2000; Keenan; Schafer, 1997; Smeltzer & Bare, 1996). SIADH also may be caused by central nervous system metastases, such as meningeal carcinomatosis (Haapoja, 1997). Treatment of a malignancy with cytotoxic chemotherapy can cause SIADH. The most commonly implicated chemo- therapeutic agents that cause SIADH and impaired excretion of water are cyclophosphamide, ifosfamide, vincristine, vinblastine, cisplatin, and melphalan (Flombaum, 2000; Keenan, 1999; Schafer, 1997). Administration of high-dose cyclophosphamide may be especially problematic in patients at risk for SIADH because aggressive hydration is used to prevent hemorrhagic cystitis, creating the potential for water retention and severe hyponatremia (Bunn & Ridgway, 1993; Flombaum; Haapoja, 1997). Combination chemotherapy often includes cisplatin administration, which usually is administered with large volumes of fluids to prevent nephrotoxicity. If hypotonic fluids (e.g., 0.45% normal saline) are used, hyponatremia and water retention may occur (Flombaum; Ritch, 1988). In addition, chemotherapy-induced nausea can stimulate the release of ADH (Haapoja). However, use of effective antiemetics has decreased the incidence of nausea as a cause of SIADH (Flombaum). Pharmacologic interventions used to treat patients with cancer may contribute to the development of SIADH. Analgesics, such as opioids, in addition to antidepressants, such as tricyclics and selective serotonin reuptake inhibitors, have been known to cause increased ADH production (Frizzell, 2000; Keenan, 1999). In addition to stimulating abnormal production of ADH, Goal for CE Enrollees: To further enhance nurses’ knowledge about syndrome of inappropriate antidiuretic hormone (SIADH). Objectives for CE Enrollees: On completion of this CE, the participant will be able to 1. Describe the etiology of SIADH. 2. Discuss the clinical manifestations and medical management of patients with SIADH. 3. Discuss the nursing implications in the care of patients with SIADH. Jo Ann Flounders, MSN, CRNP, OCN®, CHPN, is a nurse practitioner at Consultants in Medical Oncology and Hematology in Drexel Hill, PA. Digital Object Identifier: 10.1188/03.ONF.E63-E70 FLOUNDERS – VOL 30, NO 3, 2003 E63 medications may potentiate the effects of ADH on the renal tubules. Nonsteroidal anti-inflammatory drugs, thiazide diuretics, barbiturates, and anesthetic agents can increase the effects of ADH on the renal tubules (Dietz & Flaherty, 1993; Frizzell; Jones, 1999; Rohaly-Davis & Johnston, 1996). Many nonmalignant causes of SIADH exist. Injury to the cells of the central nervous system as a result of infection, brain abscess, brain herniation, hemorrhage, or head trauma may result in increased ADH production. Pulmonary disorders, such as infection caused by virus, bacteria, or fungus, also can stimulate ectopic production of ADH. Other pulmonary complications that can produce and release ADH are pneumonia, tuberculosis, and lung abscess (Dietz & Flaherty, 1993; Ezzone, 1999; Frizzell, 2000; Keenan, 1999; Schafer, 1997). Patients with malignant disease commonly experience pain and stress, which also can increase ADH production. Cigarette smoking can contribute to the development of SIADH because nicotine can induce ADH production (Dietz & Flaherty; Haapoja, 1997; Poe & Taylor, 1989). Physiology To understand the pathophysiology of SIADH, understanding the normal physiology of fluid and electrolyte balance in body compartments is necessary. Body fluids, which contain electrolytes, proteins, and water, are separated into intracellular and extracellular compartments by cell membranes and capillaries (Mulvey & Bullock, 2000). Intracellular fluid is located in trillions of cells that are separated from one another by cell membranes (Martini, 1998). Extracellular fluid consists of interstitial fluid, or fluid between the cells, and intravascular fluid, which is fluid or plasma circulating in the blood vessels (Mulvey & Bullock). Total body water is estimated to be two-thirds intracellular fluid and one-third extracellular fluid (Keenan, 1999; Martini). Intracellular and extracellular fluids exist as solutions, and the electrolyte composition of each compartment is different. The main ions in intracellular fluid are potassium, magnesium, and phosphate, and the main ions in extracellular fluid are sodium, chloride, and bicarbonate (Martini, 1998). The substances that are dissolved in the solution of intracellular and extracellular fluid are called solutes. The total concentration of solutes in the solution is defined as osmolality, which is stated as the number of milliosmols per liter (mOsm/l) or milliosmols per kilogram (mOsm/kg) (Keenan, 1999). Homeostasis demands that a balance exist in the fluid and electrolyte composition of the intracellular and extracellular compartments. Movement of solutes and water across cell membranes maintains equilibrium between intracellular and extracellular fluid. The semipermeable cell membranes only allow selective ions to cross the membrane to enter or exit cells, but the movement of water is not restricted (Martini, 1998). Water moves freely across the membranes toward the solution that contains the higher solute concentration in an effort to equalize the concentration in both compartments (Mulvey & Bullock, 2000). The process that allows free movement of water across a membrane in response to a difference in concentration is called osmosis (Martini). Osmosis maintains homeostasis by eliminating the differences in concentration of extracellular and intracellular fluids almost immediately. Therefore, despite the different chemical composition of each compartment, the osmolality, or concentration, is identical (Martini). Osmotic pressure is a force that influences the exchange of fluids and electrolytes between the compartments at the capillary level. Osmotic pressure acts as an inward pulling force that moves solutes and water into the capillaries (Mulvey & Bullock). Several basic concepts about regulation of fluids and electrolytes are important. The mechanisms that monitor and adjust the composition and volume of body fluids to maintain homeostasis respond to changes in extracellular fluid, not intracellular fluid. Because intracellular fluid is located in trillions of isolated cells separated by cell membranes, a change in one cell in the body will not directly affect other cells. In contrast, a change in extracellular fluid will occur throughout the extracellular compartment and affect all the cells in the body. Therefore, the concentration of extracellular fluid is the stimulus that triggers fluid movement (Martini, 1998). Another important concept pertaining to fluid and electrolyte regulation is that water must move across cell membranes in response to osmotic gradients, or changes in concentration between compartments, and not by active transport by cells (Martini, 1998). These concentration gradients are determined by the concentration of ions, such as sodium, the main regulator of osmotic pressure (Mulvey & Bullock, 2000). Just as water flows from an area with lesser solute concentration to an area of greater solute concentration, water also follows sodium (Martini). Therefore, when extracellular fluid has a high concentration (i.e., high osmolality) of sodium ions, or hypernatremia, water moves into the blood vessels and out of the cells. When extracellular fluid has a low concentration (i.e., low osmolality) of sodium ions, or hyponatremia, water moves out of the blood vessels and into cells where the concentration is higher (Martini; Mulvey & Bullock). Another concept that is helpful to understand is tonicity, which is used to describe osmolality (Martini, 1998). An isotonic fluid (e.g., normal saline) with the same concentration as plasma does not cause movement of water into or out of cells (Martini). Hypertonic fluids have a higher solute concentration than plasma, and hypotonic fluids have a lower solute concentration than plasma (Stripp, 2000). Therefore, infusion of a hypertonic solution into the blood vessels of extracellular fluid causes movement of water from cells into blood vessels. Infusion of a hypotonic fluid into the blood vessels of extracellular fluid causes movement of fluid from blood into cells (Martini). Figure 1 displays the effect of osmosis across a cell membrane. The volume of total body water is regulated by thirst, hormone secretion, and renal activity. In response to decreased volume of fluid and increased plasma concentration (i.e., osmolality), the hypothalamus activates nervous pathways that cause thirst. In addition, decreased plasma volume causes decreased renal perfusion, which activates the renin-angiotensin-aldosterone system and stimulates the hypothalamus to release substances that cause thirst (Mulvey & Bullock, 2000). This mechanism also causes release of ADH from the posterior pituitary (Tesh, 2000). Therefore, in normal homeostasis, ADH is produced by the hypothalamus and released into the blood by the posterior pituitary in response to increased plasma concentration (i.e., increased osmolality) or decreased plasma volume (Dietz & Flaherty, 1993; Finley, 1998). The physiologic action of ADH is to induce an antidiuretic effect on the kidneys so that water is retained (Jones, 1999). Therefore, renal regulation of fluid balance occurs through reabsorption and ONF – VOL 30, NO 3, 2003 E64 Cell in hypotonic solution Cell in isotonic solution Cell swells; water moves into cell. Normal cell: No movement of water. Cell in hypertonic solution Cell shrinks; water moves out of cell. Figure 1. Effect of Osmosis Across a Cell Membrane excretion of water by the renal tubules (Keenan, 1999; Mulvey & Bullock). In normal homeostasis, a negative feedback mechanism exists so that increased plasma volume and normal or decreased osmolality can inhibit ADH and allow excretion of water (Jones). However, SIADH causes failure of the normal mechanisms of homeostasis. Pathophysiology SIADH of malignancy is the inappropriate, uncontrolled secretion of ADH, which causes increased water reabsorption by the renal tubules that leads to decreased excretion of water (Jones, 1999). The volume of total body water increases and is distributed into the extracellular and intracellular fluid. The concentration of sodium in the extracellular fluid then is low, as a result of dilution, which causes hypoosmolality. However, because only a portion of the total body water is distributed into the extracellular fluid, most of the water diffuses into the intracellular fluid. Therefore, SIADH does not cause signs and symptoms of increased volume of fluid because the fluid is in the cells and not the blood or interstitial fluid (Bunn & Ridgway, 1993; Flombaum, 2000; Keenan, 1999). In addition, the concentration of urine is increased because the kidneys secrete sodium and cannot secrete dilute urine (Jones). The SIADH mechanism that causes thirst causes patients to continue to drink inappropriately despite the fact that in normal homeostasis, thirst is inhibited when hyponatremia is evident (Keenan). In summary, SIADH is caused by ADH secretion by tumor cells or inappropriately by the posterior pituitary and results in water intoxication, hyponatremia, and hypoosmolality (Dietz & Flaherty, 1993; Keenan). Table 1 displays the effects of SIADH. Identification of Patients at Risk for SIADH The risk of SIADH for patients with cancer corresponds to the etiologic factors that cause SIADH. Figure 2 summarizes patients at risk for development of SIADH. Clinical Manifestations Symptoms of SIADH in patients with cancer are influenced by the rate of onset and the severity of hyponatremia (Flombaum, 2000). If SIADH has a rapid (i.e., within 1 to 3 days) onset, or if the serum sodium level is less than 110 mEq/l, acute neurologic symptoms usually occur (Flombaum; Keenan, 1999). Symptoms usually are life threatening and severe when serum sodium is decreased to less than 105 mEq/l. Nonspecific symptoms may occur when the serum sodium level is 115–120 mEq/l. In contrast, if SIADH has a slow, more chronic onset, patients may be asymptomatic (Flombaum). Most patients are asymptomatic and do not develop the severe neurologic signs and symptoms associated with extreme hyponatremia (Haapoja, 1997; Keenan). Despite the water intoxication of SIADH, signs and symptoms of fluid overload usually do not appear with SIADH. Therefore, peripheral edema, ascites, and heart failure usually are not noted because only a portion of excess water is retained in the intravascular or interstitial fluid and most is distributed to the cells (Flombaum, 2000; Haapoja, 1997; Jones, 1999; Keenan, 1999). According to the principles that regulate fluid shifts between extracellular and intracellular fluids, hypotonic fluid in blood vessels shifts into cells to equalize the concentration between extracellular and intracellular fluids. Consequently, the cells of the brain swell. Because the inflexible skull confines brain cells, this cerebral edema causes increased intracranial pressure and decreased cerebral blood flow, leading to neurologic dysfunction (Bunn & Ridgway, 1993; Flombaum; Keenan). Therefore, symptoms of hyponatremia primarily are related to neurologic dysfunction Table 1. Effects of SIADH Mechanism Effect Increased water reabsorption by the renal tubule Decreased serum osmolality, hyponatremia Decreased excretion of water by the renal tubule Increased urine osmolality Increased total body water in intracellular fluid and extracellular fluid Decreased serum osmolality Decreased sodium concentration in the plasma because of dilution by excess water Hyponatremia Increased concentration of urine Increased urine osmolality Increased secretion of sodium by the kidney Increased urinary sodium FLOUNDERS – VOL 30, NO 3, 2003 E65 Patients with malignant neoplasms such as • Small cell lung cancer (most common) • Non-small cell lung cancer, head and neck, prostate, pancreatic, duodenal, esophageal, lymphoma, leukemia, breast, ovary, thymoma, neuroblastoma, and carcinoid tumors (less common) Patients receiving cytotoxic chemotherapy including • Cyclophosphamide, vincristine, vinblastine, cisplatin, and melphalan Patients who experience chemotherapy-induced nausea Patients receiving pharmacologic intervention including • Analgesics, such as opioids • Antidepressants, such as tricyclics and selective serotonin reuptake inhibitors • Non-steroidal anti-inflammatory drugs, thiazide diuretics, barbiturates, and anesthetic agents Patients with nonmalignant causes such as • Central nervous system disorders: infections, brain abscesses, brain herniation, hemorrhage, and head trauma • Pulmonary disorders: infection caused by virus, bacteria, or fungus; pneumonia; tuberculosis; and lung abscess • Pain, stress, and nicotine Figure 2. Patients at Risk for Development of SIADH Note. Based on information from Dietz & Flaherty, 1993; Ezzone, 1999; Finley, 1998; Frizzell, 2000; Haapoja, 1997; Keenan, 1999; Schafer, 1997. volume depletion or fluid overload. Restriction of water is the main treatment (Flombaum). Therefore, although a routine blood chemistry evaluation may reveal hyponatremia in asymptomatic patients, the presence of hyponatremia alone is not sufficient to diagnose SIADH. Multiple diagnostic laboratory tests must be completed and evaluated in addition to physical examination. Diagnostic Studies Laboratory studies that are diagnostic of SIADH include serum sodium, plasma osmolality, urine sodium, and urine osmolality. The normal range for serum sodium is 135–147 mEq/l. However, SIADH cannot be diagnosed on the basis of hyponatremia alone because other disorders can cause hyponatremia. Confirming a hypoosmolar state (i.e., water excess) by testing osmolality is critical. Serum osmolality usually is decreased with SIADH, whereas urine osmolality usually is increased. Electrolytes, blood urea nitrogen, creatinine, albumin, and uric acid also should be evaluated because these values usually decrease with SIADH as a result of dilution (Finley, 1998; Haapoja, 1997; Jones, 1999; Keenan, 1999; Smeltzer & Bare, 1996). Other studies to rule out cardiac, hepatic, adrenal, renal, and thyroid causes of hyponatremia should be completed (Haapoja). Serum vasopressin levels usually are not ordered because vasopressin may be elevated in most patients with hyponatremia; therefore, elevation is not specific to SIADH Table 2. Symptoms and Signs of SIADH secondary to water intoxication that leads to swelling of brain cells (Flombaum). Table 2 contains a summary of signs and symptoms of SIADH. System Signs General Weakness, fatigue, malaise Neurologic Altered mental status Headache Lethargy, irritability Delirium Psychosis Personality changes Ataxia Tremors Focal neurologic signs Seizures Coma, obtundation Confusion, disorientation Cardiovascular – Usually normal blood pressure Usually normal pulse Normal skin turgor No edema Gastrointestinal Anorexia Nausea, vomiting Diarrhea Thirst Abdominal cramping Moist mucous membranes – Oliguria (< 400 cc/24 hours) Weight gain Incontinence Physical Examination After consideration of risk factors and review of symptoms indicative of SIADH, attention to history is critical because other conditions can cause hyponatremia without the associated water excess of SIADH (Flombaum, 2000; Haapoja, 1997). Conditions to be considered in the differential diagnosis include dehydration, fluid retention, cardiac disease, hepatic dysfunction, adrenal insufficiency, renal disorders, and thyroid disease (Keenan, 1999). Review of current medications is necessary to determine if SIADH may be medication induced. Evaluating patients for signs and symptoms of dehydration or fluid overload as potential causes of hyponatremia is critical. If dehydration or fluid overload is causing hyponatremia, SIADH can be excluded as a diagnosis. Hypovolemia and hypervolemia may cause decreased sodium concentration. However, the clinical manifestations and physiologic mechanisms of hypervolemia, hypovolemia, and SIADH are different. Accurate diagnosis is critical because treatment will vary greatly (Bunn & Ridgway, 1993; Flombaum, 2000; Keenan, 1999). For example, patients with decreased volume caused by dehydration will manifest symptoms of orthostatic hypotension, poor skin turgor, dry mucous membranes, and tachycardia. The appropriate treatment is rehydration. Patients with increased volume caused by fluid overload will manifest symptoms of edema, increased jugular distention, and changes in breath sounds (i.e., rales). The treatment is restriction of sodium and water. Although both of these clinical conditions can cause hyponatremia, they require different treatment to correct the hyponatremia. In comparison, SIADH usually does not cause Symptoms Renal Musculoskeletal Muscle cramps – Hypoactive reflexes Myoclonus Note. Based on information from DeMichele & Glick, 2001; Dietz & Flaherty, 1993; Ezzone, 1999; Finley, 1998; Haapoja, 1997; Keenan, 1999; Schafer, 1997. ONF – VOL 30, NO 3, 2003 E66 (Haapoja; Keenan). A chest x-ray may be ordered to determine the presence of pulmonary disease. A computed tomography scan of the head can help determine the presence of cerebral edema, brain tumor, or brain herniation (Ezzone, 1999). Table 3 summarizes the critical laboratory values diagnostic of SIADH. Medical Management Table 3. Laboratory Values in SIADH Laboratory Test Serum sodium Nursing Management Recognition of early clinical manifestations of SIADH allows early treatment to prevent life-threatening complications. Nurses frequently are able to perceive subtle changes in patient status and should complete accurate and thorough ongoing assessment to identify early abnormal changes. Continued assessment of neuromuscular, cardiac, gastrointestinal, and renal systems is warranted. Constant evaluation of fluid and electrolyte status is necessary with ongo- < 130 mEq/L Serum osmolality < 280 mOsm/kg Urine osmolality > 500 mOsm/kg Urine sodium Medical management of SIADH must be directed at treating the underlying pathology (Finley, 1998). SIADH usually resolves when the etiologic factors that are stimulating inappropriate ADH secretion are eliminated (DeMichele & Glick, 2001). Treatment of malignant neoplasms with antineoplastic chemotherapy causes regression of chemosensitive tumors and usually results in resolution of SIADH (Keenan, 1999). If SIADH is caused by metastasis to the brain, corticosteroids and radiation therapy may be effective treatment (DeMichele & Glick). Treatment of nonmalignant causes of SIADH, including discontinuation of offending medications, is necessary. Treatment of hyponatremia is related to the severity of symptoms and the rapidity of onset (Bunn & Ridgway, 1993; Flombaum, 2000; Keenan, 1999). Treatment for mild hyponatremia in SIADH (i.e., a sodium level greater than 125 mEq/l) includes fluid restriction of 800–1000 ml/day (Finley, 1998). Fluid restriction usually allows the sodium level to correct over 3–10 days. If fluid restriction is not effective, demeclocycline can be administered. Demeclocycline allows excretion of water because it inhibits the effect of ADH on the renal tubules. Side effects of this drug include nausea, photosensitivity, and azotemia. Treatment with demeclocycline usually increases the sodium level within three to four days, and fluid restriction is not necessary (DeMichele & Glick, 2001; Finley; Keenan). Aggressive treatment may be indicated if severe neurologic symptoms, such as coma or seizures, occur with severe hyponatremia (Keenan). Administration of hypertonic 3% saline infusion over two to three hours is indicated to correct life-threatening hyponatremia. Furosemide also is given to increase urinary water excretion (Finley; Keenan). Critical Value Diagnostic of SIADHa > 20 mEq/L a In the absence of diuretic therapy Note. Based on information from Dietz & Flaherty, 1993; Ezzone, 1999; Finley, 1998; Haapoja, 1997; Keenan, 1999; Schafer, 1997. ing physical assessment to detect early signs of neurologic complications caused by hyponatremia. This especially is important when assessing the volume status of patients, which is critical for diagnosing SIADH. Nurses should assess for signs and symptoms of hypovolemia or hypervolemia and understand that the occurrence of these clinical manifestations excludes the diagnosis of SIADH. Nurses should review medications to reveal possible causative agents of SIADH and provide patients and caregivers with necessary instructions regarding fluid restriction. IV hydration, chemotherapy, medications, and electrolytes may be ordered and must be monitored carefully. Assessment of patients for side effects of treatment of SIADH should be ongoing. Attention to the timeliness of completion of laboratory tests will ensure that electrolyte status is evaluated promptly. In addition, nurses should monitor blood and urine chemistry levels and ensure that measures to correct abnormal values are instituted in a timely manner. Nurses should assess the coping abilities of critically ill patients and caregivers; assess for pain, anxiety, and depression; and provide interventions to improve pain management and coping ability. However, management of pain and depression may be challenging, because some analgesics and antidepressants that cause SIADH may need to be withdrawn and substitutions made. The choice of medications must involve consideration of causative agents of SIADH. Nurses should provide patients and caregivers with instructions on signs and symptoms of complications that should be reported to a physician. Discharge planning should include consideration of referral for home care or hospice services. The author would like to thank John Sprandio, MD, of Consultants in Medical Oncology and Hematology, Drexel Hill, PA, for reviewing this manuscript. Author Contact: Jo Ann Flounders, MSN, CRNP, OCN®, CHPN, can be reached at [email protected], with copy to editor at [email protected]. References Bunn, P., & Ridgway, E. (1993). Paraneoplastic syndromes. In V. DeVita, S. Hellman, & S. Rosenberg (Eds.). Cancer principles and practice of oncology (4th ed., pp. 2026–2071). Philadelphia: Lippincott. DeMichele, A., & Glick, J. (2001). Cancer-related emergencies. In R. Lenhard, R. Osteen, & T. Gansler (Eds.), Clinical oncology (pp. 733–764). Atlanta, GA: American Cancer Society. Dietz, K., & Flaherty, A. (1993). Oncologic emergencies. In S. Groenwald, M. Frogge, M. Goodman, & C. Yarbro (Eds.), Cancer nursing principles and practice (3rd ed., pp. 800–839). Boston: Jones and Bartlett. Ezzone, S. (1999). SIADH. Clinical Journal of Oncology Nursing, 3, 187– 188. Finley, J. (1998). Metabolic emergencies. In J. Itano & K. Taoka (Eds.), Core curriculum for oncology nursing (3rd ed., pp. 315–339). Philadelphia: Saunders. FLOUNDERS – VOL 30, NO 3, 2003 E67 Flombaum, C. (2000). Metabolic emergencies in the cancer patient. Seminars in Oncology, 27, 322–334. Frizzell, J. (2000). Altered endocrine function. In B. Bullock & R. Henze (Eds.), Focus on pathophysiology (pp. 669–706). Philadelphia: Lippincott. Haapoja, I. (1997). Paraneoplastic syndromes. In S. Groenwald, M. Frogge, M. Goodman, & C. Yarbro (Eds.), Cancer nursing principles and practice (4th ed., pp. 702–720). Boston: Jones and Bartlett. Jones, L. (1999). Electrolyte imbalances. In C. Yarbro, M. Frogge, & M. Goodman (Eds.), Cancer symptom management (2nd ed., pp. 438–456). Boston: Jones and Bartlett. Keenan, A. (1999). Syndrome of inappropriate secretion of antidiuretic hormone in malignancy. Seminars in Oncology Nursing, 15, 160–167. List, A., Hainsworth, J., Davis, B., Hande, K., Greco, F., & Johnson, D. (1986). The syndrome of inappropriate secretion of antidiuretic hormone (SIADH) in small cell lung cancer. Journal of Clinical Oncology, 4, 1191– 1198. Martini, F. (1998). Fundamentals of anatomy and physiology (4th ed.). Upper Saddle River, NJ: Prentice Hall. Moses, A., & Scheinman, S. (1991). Ectopic secretion of neurohypophyseal peptides in patients with malignancy. Endocrinology and Metabolism Clinics of North America, 20, 489–506. Mulvey, M., & Bullock, B. (2000). Fluid, electrolyte, and acid-base balance. In B. Bullock & R. Henze (Eds.), Focus on pathophysiology (pp. 158–188). Philadelphia: Lippincott. Poe, C., & Taylor, L. (1989). Syndrome of inappropriate antidiuretic hormone: Assessment and nursing implications. Oncology Nursing Forum, 16, 373–381. Ritch, P. (1988). Cis-dichlorodiammineplatinum II-induced syndrome of inappropriate secretion of antidiuretic hormone. Cancer, 61, 448–450. Rohaly-Davis, J., & Johnston, K. (1996). Hematologic emergencies in the intensive-care unit. Critical Care Nursing Quarterly, 18(4), 35–43. Schafer, S. (1997). Oncologic complications. In S. Otto (Ed.), Oncology nursing (3rd ed., pp. 413–421). St. Louis, MO: Mosby. Smeltzer, S., & Bare, B. (1996). Brunner and Suddarth’s textbook of medicalsurgical nursing. (8th ed., pp. 265–316). Philadelphia: Lippincott-Raven. Stripp, R. (2000). Normal and altered cellular function. In B. Bullock & R. Henze (Eds.), Focus on pathophysiology (pp. 3–46). Philadelphia: Lippincott. Tesh, A. (2000). Normal renal function and urinary excretion. In B. Bullock & R. Henze (Eds.), Focus on pathophysiology (pp. 589–602). Philadelphia: Lippincott. For more information . . . ➤ eMedicine: Syndrome of Inappropriate Antidiuretic Hormone www.emedicine.com/emerg/topic784.htm ➤ Lucile Packard Children’s Hospital: SIADH www.lpch.org/DiseaseHealthInfo/HealthLibrary/diabetes/ siadh.html Links can be found using ONS Online at www.ons.org. ONF – VOL 30, NO 3, 2003 E68 ONF Continuing Education Examination Syndrome of Inappropriate Antidiuretic Hormone Contact Hours: 1.4 Passing Score: 80% Test ID #: 03-30/3-06 Test Processing Fee: $15 The Oncology Nursing Society is accredited as a provider of continuing education (CE) in nursing by the • American Nurses Credentialing Center’s Commission on Accreditation. • California Board of Nursing, Provider #2850. CE Test Questions 1. Which laboratory tests would indicate a patient has life-threatening syndrome of inappropriate antidiuretic hormone (SIADH)? a. Urine sodium of 18 mEq/l and urine osmolality of 550 mOsm/kg b. Urine osmolality of 550 mOsm/kg and serum sodium of 135 mEq/l c. Serum sodium of 110 mEq/l and serum osmolality of 250 mOsm/kg d. Serum osmolality of 280 mOsm/kg and urine osmolality of 450 mOsm/kg 2. A patient diagnosed with metastatic small-cell lung cancer is first placed at risk for developing SIADH because of her a. History of chronic obstructive pulmonary disease (COPD). b. Central nervous system metastasis. c. Lung cancer diagnosis. d. Treatment with antiemetics. 3. Which system should the nurse plan to assess first for a patient with SIADH effusion? a. Neurologic b. Cardiovascular c. Gastrointestinal d. Musculoskeletal 4. A patient’s electrolytes indicate low serum sodium. Which physical examination finding would be consistent with SIADH? a. Edema b. Tachycardia c. Altered mental status d. Orthostatic hypotension 5. The medical intervention that would be initiated first for a patient with SIADH is a. Fluid restrictions. b. Furosemide 40 mg IV twice a day. c. Hypertonic 3% saline infusion. d. Democlocycline. 6. A patient received high-dose cyclophosphamide for breast cancer, and within two days of treatment she developed SIADH. What is most likely the cause of her SIADH? a. Aggressive hydration b. High-dose antiemetics c. Breast cancer d. Metastasis to pituitary gland 7. The patient expresses fear that her cancer has spread and is causing SIADH. The nurse’s best response would be that SIADH is caused by a. Damage to of the thyroid gland from metastatic cancer. b. A malignancy spreading and invading the pituitary gland. c. A tumor secreting excess amounts of the antidiuretic hormone (ADH) d. Excess ADH production and release from the thyroid gland. 8. Which patient is at highest risk for developing acute neurologic symptoms? A patient with an onset of hyponatremia at a. Two days with a sodium of 130 mEq/l. b. Three days with a sodium of 110 mEq/l. c. Five days with a sodium of 125 mEq/l. d. Seven days with a sodium of 120 mEq/l. 9. A patient’s sodium is 105 mEq/l after being treated two days ago with cisplatin for lung cancer. What orders would the nurse expect? a. Low-sodium diet b. Seizure precautions c. Intravenous normal saline at 100 cc/hour d. Fluid restrictions of 1,000 ml/day 10. A patient develops mild hyponatremia and is placed on fluid restrictions. Which is the most appropriate patient education? a. Fluid restrictions, if followed carefully, can help SIADH resolve in one to two days. b. Your total amount of water intake will be restricted to 1,200 ml/day to prevent water retention. c. The restrictions will be 300 ml per meal and 200 ml with your medications four times each day. d. Hyponatremia occurs with excess free water and can be decreased by limiting the fluid intake. 11. The physician orders chemotherapy for a patient with SIADH. The family expresses concerns that the chemotherapy is being resumed. The nurse can best respond by explaining that if the chemotherapy is successful, a. The pituitary gland will stop producing ADH. b. The tumor, which is causing the SIADH to occur, will stop metastasizing. c. The tumor will stop secreting the excess ADH, and the SIADH will decrease. d. The tumor will decrease its pressure on the pituitary gland, which is excreting ADH. ONCOLOGY NURSING FORUM – VOL 30, NO 3, 2003 E69 12. Which nursing monitoring would be critical when caring for a patient with SIADH? a. Take vitals signs hourly. b. Keep strict input and output. c. Assess for signs of peripheral edema. d. Draw serum electrolytes every other day. 13. High-dose cisplatin is ordered despite a patient’s current hyponatremia. Which nursing assessment will be most critical? a. Amount of IV fluids administered to prevent hemorrhagic cystitis b. The type of antiemetics ordered for potential nausea and vomiting c. Amount of IV fluids administered to prevent nephrotoxicity d. Administration of furosemide with lactated ringers for hydration 14. The nurse is reviewing the current medication administration records for a patient at risk for SIADH. The patient is being treated for lung cancer and has an exacerbation of his COPD. Which medication ordered for this patient should be clarified? a. Furosemide 20 mg orally, twice a day b. Dexamethasone 3 mg orally, once daily c. Morphine 30 mg IV, as needed every two hours d. Lorazepam 1 mg orally, as needed at bedtime 15. In addition to hyponatremia, which kidney function test values would be most consistent with SIADH? a. Blood urea nitogen (BUN) 5 mg/dl and creatinine 0.2 mg/dl b. BUN 6 mg/dl and creatinine 1.8 mg/dl c. BUN 10 mg/dl and creatinine 0.5 mg/dl d. BUN 19 mg/dl and creatinine 1.7 mg/dl Oncology Nursing Forum Answer/Enrollment Form Syndrome of Inappropriate Antidiuretic Hormone (Test ID #03-30/3-06) To receive continuing education (CE) credit for this issue, simply 1. Read the article. 2. Oncology Nursing Society members may take the test and get results immediately on ONS Online. Simply log on to www.ons.org and click on ONF (Oncology Nursing Forum) under the Publications heading. Use your ONS membership number to access the site, select the issue you wish to use, scroll down to find the CE test, and follow the instructions. After successfully completing the test, pay with a credit card. 3. To enroll via the mail, record your answers on the form below Instructions: Mark your answers clearly by placing an “x” in the box next to the correct answer. This is a standard form; use only the number of spaces required for the test you are taking. Name 1. ❑ ❑ ❑ ❑ 11. ❑ ❑ ❑ ❑ a b c d 2. ❑ ❑ ❑ ❑ a b c d 3. ❑ ❑ ❑ ❑ a b c d and complete the program evaluation (you may make copies of the form.) Mail the completed answer/enrollment form along with a check or money order for $15 per test payable to the Oncology Nursing Society. Payment must be included for your examination to be processed. 4. The deadline for submitting the answer/enrollment form is two years from the date of this issue. 5. Contact hours will be awarded to RNs who successfully complete the program. Successful completion is defined as an 80% correct score on the examination and a completed evaluation program. Verification of your CE credit will be sent to you. Certificates will be mailed within six weeks fol- 4. ❑ ❑ ❑ ❑ a b c d State(s) of licensure/license no(s). Program Evaluation a b c d 6. ❑ ❑ ❑ ❑ a b c d 7. ❑ ❑ ❑ ❑ a b c d 8. ❑ ❑ ❑ ❑ a b c d 9. ❑ ❑ ❑ ❑ a 10. ❑ a ❑ b b ❑ c c ❑ d d a 12. ❑ a 13. ❑ a 14. ❑ a 15. ❑ a 16. ❑ a 17. ❑ a 18. ❑ a 19. ❑ a 20. ❑ a ❑ b ❑ b ❑ b b ❑ b ❑ b ❑ b ❑ b ❑ b ❑ b ❑ c ❑ c ❑ c c ❑ c ❑ c ❑ c ❑ c ❑ c ❑ c ❑ d ❑ d d ❑ d ❑ d ❑ d ❑ d ❑ d ❑ d ❑ d Telephone # Address City 5. ❑ ❑ ❑ ❑ Social Security # State Zip Not at all Low Medium 1. How relevant were the objectives to the CE activity’s goal? ❑ ❑ ❑ 2. How well did you meet the CE activity’s objectives (see page E63)? ❑ ❑ ❑ • Objective #1 ❑ ❑ ❑ • Objective #2 ❑ ❑ ❑ • Objective #3 ❑ ❑ ❑ 3. To what degree were the teaching/learning resources helpful? Too basic Appropriate Too complex 4. Based on your previous knowledge and experience, do you think ❑ ❑ ❑ that the level of the information presented in the CE activity was 5. How long did it take you to complete the CE activity? minutes ❑ My check or money order payable to the Oncology Nursing Society is enclosed. U.S. currency only. (Do not send cash.) After completing this form, mail it to: Oncology Nursing Society, P.O. Box 3510, Pittsburgh, PA 15230-3510. For more information or information on the status of CE certificates, call 866-257-4667, ext. 6296. ONCOLOGY NURSING FORUM – VOL 30, NO 3, 2003 E70 High ❑ ❑ ❑ ❑ ❑