Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
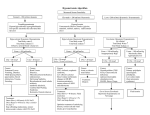
Approach To A Patient With Hyponatremia A Muruganathan INTRODUCTION H yponatremia is defined as a decrease in the serum sodium concentration to a level below 136 mmol per liter. Whereas hypernatremia always denotes hypertonicity, hyponatremia can be associated with low, normal, or high tonicity. Serum sodium concentration and serum osmolarity normally are maintained under precise control by homeostatic mechanisms involving stimulation of thirst, secretion of antidiuretic hormone (ADH), and renal handling of filtered sodium. FREQUENCY Most common electrolyte disorder Incidence of approximately 1% Prevalence of approximately 2.5% Surgical ward, approximately 4.4% 30% of patients treated in the intensive care unit Hyponatremia's prevalence is lower in the ambulatory setting. SEX No sexual predilection exists. However, symptoms are more likely to occur in young women > men AGE Infants fed tap water in an effort to treat symptoms of gastroenteritis. Infants fed dilute formula in attempt to ration. Elderly patients with diminished sense of thirst, especially when physical infirmity limits independent access to food and drink. More common in elderly persons. Due to increased incidence of comorbid conditions (eg, cardiac, hepatic, or renal failure) PATHOPHYSIOLOGY Increases in serum osmolarity above the normal range (280-300 mOsm/kg) stimulate hypothalamic osmoreceptors, which, in turn, cause an increase in thirst and in circulating levels of ADH. ADH increases free water reabsorption from the urine, yielding urine of low volume and relatively high osmolarity and, as a result, returning serum osmolarity to normal. ADH is also secreted in response to hypovolemia, pain, fear, nausea, and hypoxia. Aldosterone, synthesized by the adrenal cortex, is regulated primarily by serum potassium but also is released in response to hypovolemia through the renin-angiotensin-aldosterone axis. Aldosterone causes absorption of sodium at the distal renal tubule. Sodium retention obligates free water retention, helping to correct the hypovolemic state. The healthy kidney regulates sodium balance independently of ADH or aldosterone by varying the degree of sodium absorption at the distal tubule. Hyponatremia Types and Causes Hypovolemic hyponatremia, Euvolemic hyponatremia, Hypervolemic hyponatremia, Redistributive hyponatremia, Pseudohyponatremia Hypovolemic hyponatremia Hypovolemic hyponatremia develops as sodium and free water are lost and replaced by inappropriately hypotonic Medicine Update-2011 fluids, such as tap water, half-normal saline, or dextrose in water. Total body water (TBW) decreases. Total body sodium (Na+) decreases to a greater extent. The extracellular fluid (ECF) volume is decreased. Nonrenal loss: GI losses, Vomiting, Diarrhea, fistulas, Third spacing of fluids, Ascites, peritonitis, pancreatitis, and burns, Excessive sweating. Cerebral salt-wasting syndrome seen in patients with traumatic brain injury, aneurysmal subarachnoid hemorrhage, and intracranial surgery. Prolonged exercise in a hot environment, especially in patients who hydrate aggressively with hyposmolar fluids during exertion. Severe symptomatic hyponatremia has been reported in marathon runners and in recreational hikers. Renal Loss Acute or chronic renal insufficiency, in which the patient may be unable to excrete adequate amounts of free water Salt-wasting nephropathy Euvolemic hyponatremia TBW increases while total sodium remains normal. The ECF volume is increased minimally but without the presence of edema. Causes Drugs/Tumors continuous ADH secretion or increased action of ADH Associated with … CNS: Encephalitis, Meningitis, Head trauma, Brain Abscess,Brain tumors, CVA. Peripheral neuropathy, Subarachnoid Hge, Guillian Barre Syndrome, Multiple sclerosis. Carcinomas: Bronchogenic Ca, Mesothelioma. Ca duodenum, pancreas, stomach, Bladder, ureter, prostate. Pulmonary: Pneumonias,Tuberculosis, Asthma, Pulmonary abscess, Positive pressure Ventilation, Pneumothorax. Others: HIV, Idiopathic (elderly), Prolonged Exercise. Acute intermittent porphyria Surgery. MEDICATIONS Known offenders include acetazolamide, amiloride, amphotericin, aripiprazole, atovaquone, thiazide diuretics, amiodarone, basiliximab, angiotensin II receptor blockers, 197 angiotensin-converting enzyme inhibitors, bromocriptine, carbamazepine, carboplatin, carvedilol, celecoxib, cyclophosphamide, clofibrate, desmopressin, donepezil, duloxetine, eplerenone, gabapentin, haloperidol, heparin, hydroxyurea, indapamide, indomethacin, ketorolac, levetiracetam, loop diuretics, lorcainide, mirtazapine, mitoxantrone, nimodipine, oxcarbazepine, opiates, oxytocin, pimozide, propafenone, proton pump inhibitors, quetiapine, sirolimus, ticlopidine, tolterodine, vincristine, selective serotonin reuptake inhibitors, sulfonylureas, trazodone, tolbutamide, venlafaxine, zalcitabine, and zonisamide. Psychogenic polydipsia, often in psychiatric patients. Administration of hypotonic intravenous or irrigation fluids during procedures or in the immediate postoperative period Infants who may have been given inappropriate amounts of free water. Ingestion of sodium phosphate or sodium picosulfates and magnesium citrate combination as a bowel preparation before colonoscopy or colorectal surgery. Uncorrected hypothyroidism or cortisol deficiency (adrenal insufficiency, hypopituitarism). Consumption of large quantities of beer or use of the recreational drug MDMA (ecstasy) Hypervolemic hyponatremia Total body sodium increases. TBW increases to a greater extent. The ECF is increased markedly, with the presence of edema. This may result from renal causes such as acute or chronic renal failure, when dysfunctional kidneys are unable to excrete the ingested sodium load. It also may occur in response to states of decreased effective intravascular volume. History of hepatic cirrhosis, congestive heart failure, or nephrotic syndrome, in which patients are subject to insidious increases in total body sodium and free water stores Redistributive hyponatremia Water shifts from the intracellular to the extracellular compartment, with a resultant dilution of sodium. The TBW and total body sodium are unchanged. This condition occurs with hyperglycemia. Administration of mannitol Pseudohyponatremia The aqueous phase is diluted by excessive proteins or lipids. The TBW and total body sodium are unchanged. Hypertriglyceridemia. Multiple myeloma Approach to Hyponatremia For the diagnosis and treatment of a given hyponatremia 198 Medicine Update-2011 the clinical evaluation has to include a careful medical history, a physical examination with attention to the patient’s extracellular fluid volume status and laboratory measurements. Symptoms: Patients with clinically significant hyponatremia present with nonspecific symptoms attributable to cerebral edema. These symptoms, especially when coupled with a peripheral edema, or ascites suggest hypervolemic hyponatremia due to excess retention of sodium and free water (ie, cirrhosis, nephrotic syndrome, congestive heart failure). Other nonspecific signs include muscle weakness and cramping. Rhabdomyolysis is an occasional consequence of hyponatremia and should be considered in patients with muscle pain or tenderness. LABORATORY TESTS FOR THE DIFFERENTIAL DIAGNOSIS OF HYPONATREMIA Preliminary tests Serum osmolality Urine osmolality or urine specific gravity Urine levels of sodium and creatinine, and calculation of fractional excretion of sodium (FENa+)* Serum levels of potassium, chloride and bicarbonate Serum levels of glucose, urea, creatinine, total proteins, triglycerides and uric acid Serum levels of thyroid-stimulating hormone and cortisol. Brain CT Scans Effects of Hyponatremia on the Brain and Adaptive Responses. recent history of altered fluid balance, should suggest the possibility of hyponatremia. Anorexia, Nausea and vomiting, Difficulty concentrating, Confusion, Lethargy, Agitation, Headache, Seizures. Physical Most abnormal findings on physical examination are characteristically neurologic in origin. Level of alertness ranging from alert to comatose. Variable degrees of cognitive impairment (eg, difficulty with short-term recall; loss of orientation to person, place, or time; frank confusion or depression). Focal or generalized seizure activity. In those patients with acute severe hyponatremia, signs of brainstem herniation, including coma; fixed, unilateral, dilated pupil; decorticate or decerebrate posturing; sudden severe hypertension and respiratory arrest. In addition to neurologic findings, patients may exhibit signs of hypovolemia or hypervolemia. Dry mucous membranes, tachycardia, diminished skin turgor, and orthostasis suggest hypovolemic hyponatremia due to excessive loss of body fluids and replacement with inappropriately dilute fluids. Pulmonary rales, S3 gallop, jugular venous distention, Normal Study Fataly Hyponatremia CT head, EKG, CXR Additional tests Arterial blood gases if serum bicarbonate level is abnormal Urine levels of urea and uric acid, and calculation of their fractional excretion for the differential diagnosis of hypovolemia versus SIADH. Plasma osmolality: Normally ranges from 275 to 290 mosmol/ kg. If >290 mosmol/kg: Hyperglycemia or administration of mannitol. If 275 - 290 mosmol/kg: Hyperlipidemia or Hyperproteinemia In the hypo-osmolar state (serum osmolality less than 280 mOsm/kg), urine osmolality is used to determine whether water excretion is normal or impaired. A urine sodium level less than 20 mmol/L is indicative of hypovolemia, whereas a level greater than 40 mmol/L is suggestive of the syndrome Medicine Update-2011 of inappropriate antidiuretic hormone secretion. Urine osmolality: Normal value is > 100 mosmol/kg. Normal to high: Hyperlipidemia, hyperproteinemia, hyperglycemia, SIADH. FeNa-Help to determine pre-renal from renal causes MANAGEMENT The key to effective management of hyponatremia is establishing the type and its cause, so that the cause can be removed, if possible, and the management will be appropriate. The treatment of hyponatremia is determined by 3 major factors: severity of hyponatremia, that is, the 199 presence or absence of severe central nervous system symptoms such as lethargy, delirium, seizure, and coma; onset of hyponatremia: acute (within 48 hours) or chronic (_48 hours); and volume status. Prehospital Care Hyponatremia is necessarily a hospital-based diagnosis, but patients may exhibit signs of severe neurologic dysfunction during prehospital evaluation and transport. Address acute life-threatening conditions and initiate supportive care. Diagnosis-Algorithm 200 Medicine Update-2011 Establish reliable intravenous access and give supplemental oxygen to patients with lethargy or obtundation. In these patients, evaluate the possibility of hypoglycemia with a rapid glucose check. Administer intravenous glucose to hypoglycemic patients. Administer standard prehospital anticonvulsant therapy to patients experiencing seizures. Seizures secondary to hyponatremia are unlikely to respond to this therapy, but it should be administered until a definitive diagnosis and therapy are available. Intubate and initiate hyperventilation to reduce intracranial pressure in patients exhibiting signs of brainstem herniation (eg, obtundation; fixed, unilateral, dilated pupil; decerebrate or decorticate posturing) until a more definitive therapy can be initiated. Avoid giving hypotonic intravenous fluids because they may exacerbate cerebral edema. Emergency Department Care The ultimate danger for these patients is brainstem herniation when sodium levels fall below 120 mEq/L. The source of free water must be identified and eliminated. Patients with seizures, severe confusion, coma, or signs of brainstem herniation should receive hypertonic (3%) saline to rapidly correct serum sodium level toward normal but only enough to arrest the progression of symptoms. An increase in serum sodium level of 4-6 mEq/L is generally sufficient. Any further correction is potentially dangerous and must be avoided unless necessary to correct continued seizures or other severe CNS abnormality. Chronic hyponatremia must be managed with extreme care. Treatment of chronic hyponatremia has been associated with the development of the osmotic demyelination syndrome (also known as central pontine myelinolysis) characterized by focal demyelination in the pons and extrapontine areas associated with serious neurologic sequelae. The estimated total body water (in liters) is calculated as a fraction of body weight. The fraction is 0.6 in children; 0.6 and 0.5 in nonelderly men and women, respectively; and 0.5 and 0.45 in elderly men and women, respectively. Normally extracellular and intracellular fluids account for 40 and 60 percent of total body water, respectively. The syndrome is caused by overly rapid correction or overcorrection of chronic hyponatremia. Some investigators note that osmotic demyelination often develops when chronic hyponatremia is complicated by hypoxia and believe that osmotic demyelination may be a form of hypoxic encephalopathy associated with hyponatremia and not a complication of therapy. Until further data are available, management should include meticulous attention to adequate oxygenation and a gradual increase in serum sodium level to 120-125 mEq/L. Serum sodium level should not be allowed to reach normal levels or hypernatremic levels within the first 48 hours. Symptoms of osmotic demyelination (eg, dysarthria, Formulas For Use In Managing Hyponatremia And Charecteristics Of Infusates Medicine Update-2011 dysphagia, seizures, altered mental status, quadriparesis, hypotension) typically begin 1-3 days after correction of serum sodium level. Patients with hypokalemia, female gender, or history of alcoholism or liver transplant seem to be particularly prone to develop osmotic demyelination. Exercise extreme caution in treating hyponatremia in these subgroups. 201 Pharmacological Rx of Chronic Asymptomatic Hyponatremia Patients with chronic hyponatremia and severe symptoms (eg, severe confusion, coma, seizures) should receive hypertonic saline but only enough to raise the serum sodium level by 4-6 mEq/L and to arrest seizure activity. Anecdotal reports suggest that therapeutic relowering of the serum sodium level with hypotonic fluids and desmopressin (DDAVP) may help avert neurologic sequelae in patients whose chronic hyponatremia is inadvertently corrected too quickly. Regardless of the therapeutic approach, serum sodium must be monitored closely and corrected no faster than 10-12 mEq/L in the first 24 hours and 18 mEq/L in the first 48 hours. Hypovolemic hyponatremia: If symptoms are mild to moderately severe, treat with isotonic saline; monitor serum sodium levels frequently to ensure that the serum sodium level increases slowly. Because most hyponatremia is caused by the non-osmotic release of vasopressin, the availability of vasopressin antagonists is exciting and may change the management of hyponatremia completely. V2-receptor antagonists are not suitable for certain causes of hyponatremia, such as cerebral salt wasting syndrome, psychogenic polydipsia/ potomania, and others. Hypervolemic hyponatremia: Treatment consists of sodium and water restriction and attention to the underlying cause. The vasopressin receptor antagonists conivaptan (Vaprisol) and tolvaptan (Samsca) are now approved for use in hospitalized patients with hypervolemic hyponatremia, though clinical experience is scant. Euvolemic hyponatremia: Treatment consists of free water restriction and correction of the underlying condition. convivaptan, tolvaptan show promise as effective and welltolerated intravenous therapy for SIADH. Clozapine appears to be effective in the long-term treatment of schizophrenic patients with compulsive water drinking. Prevention Hyponatremia that is acquired in the hospital is largely preventable. A defect of water excretion can be present on admission, or it can worsen or develop during the course of hospitalization as a result of several antidiuretic influences (e.g., medications, organ failure, and the postoperative state). The presence of such a defect notwithstanding, hyponatremia will not develop as long as the intake of electrolyte-free water does not exceed the capacity for water excretion plus insensible losses. Prognosis Prognosis is dependent on the underlying condition and the severity of disease. Medicolegal Pitfalls Failure to consider the possibility of sampling or analysis error, hyperglycemia, hyperproteinemia, or hyperlipidemia before making the diagnosis of hypovolemic hyponatremia Failure to recognize high-risk groups, including elderly patients, patients on diuretics, infants, postoperative patients, and patients with malignancy. Failure to quickly recognize severe acute hyponatremia and to correct it promptly, allowing ongoing risk of brainstem herniation. Correcting serum sodium level too rapidly in patients with chronic hyponatremia (in excess of 0.5 mEq/L/h or 12 mEq/ L/d), thereby incurring the risk of osmotic demyelination syndrome. TAKE HOME MESSAGES It is a more a disorder of water balance than sodium itself. Look for hyponatremia in a drowzy patient when cause is 202 Medicine Update-2011 unclear. Always look for in an unconscious icu patient. Look for offending drugs (diuretics ..,). “Start low - go slow” applies for hypertonic saline treatment. Avoid hypertonic REFERENCES 1. Review Article Hyponatremia By Horacio J. A.Drogué, M.D.,And Nicolaos E. Madias, M.D. May 25, 2000 in The New England Journal of medicine. 2. Hyponatremia: Clinical Diagnosis and Management By Yeong-Hau H. Lien, MD, PhD, Joseph I. Shapiro, MD. The American Journal of Medicine Aug.2007 3. Lee DS, Austin PC, Rouleau JL, Liu PP, Naimark D, Tu JV. redicting mortality among patients hospitalized for heart failure: derivation and validation of a clinical model. JAMA. 2003;290(19):2581-2587. 4. Almond CS, Shin AY, Fortescue EB, etal. Hyponatremia among runners in the Boston Marathon. N Engl J Med. 005;352(15):1550- 1556. 5. Noakes TD, Sharwood K, Speedy D, etal. Three independent biological mechanisms cause exercise-associated hyponatremia: evidence from 2,135 weighed competitive athletic performances. Proc Natl Acad Sci U S A. 2005;102(51):18550-18555. saline in asymptomatic patient. Free oral water restriction - an important but ignored step in treatment. Monitor renal parameters and daily fluid balance. 6. 7. 8. 9. 10. Noakes T. Fluid replacement during marathon running. Clin J Sport Med. 2003;13(5):309-318. Schrier RW, Chen YC, Cadnapaphornchai MA. From finch to fish to man: role of aquaporins in body fluid and brain water regulation. Neuroscience. 2004;129(4):897-904. Lee DS, Austin PC, Rouleau JL, Liu PP, Naimark D, Tu JV. Predicting mortality among patients hospitalized for heart failure: derivation and validation of a clinical model. JAMA. 2003;290(19):2581-2587. Zeltser D, Rosansky S, van Rensburg H, Verbalis JG, Smith N. Conivaptan study group. Assessment of the efficacy and safety of intravenous conivaptan in euvolemic and hypervolemic hyponatremia. Am J Nephrol. 2007;27:447-57. Schrier RW, Gross P, Gheorghiade M, et al. SALT Investigators. Tolvaptan, a selective oral vasopressin V2-receptor antagonist, for hyponatremia. N Engl J Med. 2006;355:2099-112.