Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
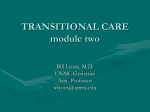
Experimental Neurology 243 (2013) 67–73 Contents lists available at SciVerse ScienceDirect Experimental Neurology journal homepage: www.elsevier.com/locate/yexnr Review Sundowning syndrome in aging and dementia: Research in mouse models Tracy A. Bedrosian ⁎, Randy J. Nelson Department of Neuroscience, Wexner Medical Center at The Ohio State University, Columbus, OH 43210, USA a r t i c l e i n f o a b s t r a c t Article history: Received 11 January 2012 Revised 30 April 2012 Accepted 8 May 2012 Available online 14 May 2012 Both normal aging and dementia are associated with altered circadian regulation of physiology and behavior. Elderly individuals and dementia patients commonly experience disrupted sleep–wake cycles, which may lead to psychomotor agitation, confusion, and wandering. These behaviors are disruptive to both patients and caregivers. Sundowning syndrome, which encompasses many of these behaviors, is characterized by a temporal pattern in the severity of symptoms, usually expressed as worse during the late afternoon or evening. Other than antipsychotic medications, off-label medications, and restraint, few treatment options are available. The aim of this paper is to review mouse studies of circadian behavioral disturbances relevant to sundowning, in order to determine potential models for studying the mechanisms of sundowning syndrome. The emergence of a useful mouse model should facilitate the development of novel therapeutic approaches. © 2012 Elsevier Inc. All rights reserved. Keywords: Aging Alzheimer disease Agitation Circadian Contents Introduction . . . . . . . . . . What is sundowning? . . . . . Clinical research . . . . . . . . Pre-clinical research . . . . . . Potential mechanisms underlying Future directions . . . . . . . . Acknowledgments . . . . . . . References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . sundowning . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Introduction Increasingly, evidence suggests a role for the circadian system in mood and emotion (Benca et al., 2009). Circadian disturbances are particularly common during the aging process, which may contribute to psychological or behavioral disturbances. Much of this circadian dysregulation is exacerbated in cases of underlying dementia pathology, leading to even more behavioral problems among this population. Traditionally, greater importance has been given to cognitive symptoms of aging and dementia, though non-cognitive symptoms represent a major cause of hospitalization, institutionalization, and distress for these individuals (Finkel, 2000). One prominent age-related change in circadian organization is dysregulation of physiological rhythms. For example, aging is often ⁎ Corresponding author at: Department of Neuroscience, 636 Biomedical Research Tower, Wexner Medical Center at The Ohio State University, Columbus, OH 43210, USA. E-mail address: [email protected] (T.A. Bedrosian). 0014-4886/$ – see front matter © 2012 Elsevier Inc. All rights reserved. doi:10.1016/j.expneurol.2012.05.005 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 67 68 69 69 70 71 72 72 associated with reduced amplitude of 24-h patterns in arousal, body temperature, and hormone fluctuations (for review: Van Someren, 2000). Altered period, amplitude, and responsiveness to zeitgebers (i.e., entraining cues) may also occur for certain rhythms among aged individuals. In Alzheimer patients, phase delays in core body temperature may be related to the severity of disease pathology (Hatfield et al., 2004). Mouse studies have similarly shown a decrease in circadian output with age, originating in the brain's master clock (Nakamura et al., 2011), and behavioral changes in locomotor activity and anxiety (Scheuermaier et al., 2010). Some of this circadian dysregulation, particularly altered activity and arousal rhythms, may facilitate circadian behavioral disturbances such as sundowning. Sundowning syndrome, which includes agitation and delirium, is characterized by a temporal pattern in the severity of symptoms, usually expressed as more severe during the late afternoon or evening (Bachman and Rabins, 2006). Elderly individuals and dementia patients commonly experience disrupted sleep–wake cycles and poor sleep quality, which may lead to psychomotor agitation, confusion, and wandering (Vitiello and 68 T.A. Bedrosian, R.J. Nelson / Experimental Neurology 243 (2013) 67–73 Borson, 2001). These behaviors are disruptive to both the patient and caregivers (Donaldson et al., 1998; Pollak and Perlick, 1991). Interestingly, degree of sleep disturbance is associated with disease severity in Alzheimer patients (Bliwise et al., 2011). In mice, sleep deprivation may be anxiogenic in animals exposed to assessments of anxiety-like responses (e.g., performance in an elevated plus maze) (Silva et al., 2004). Sundowning symptoms may or may not simply reflect sleep deprivation; alternatively, sundowning symptoms may be exacerbated by sleep deprivation or relatively independent of sleep. Taken together, circadian disturbances represent a serious detriment to individuals' quality of life. The majority of the elderly population experiences chronic sleep disturbances, which worsen with age (Van Someren, 2000). Other than antipsychotic medications, off-label medications, and restraint, few treatment options are available. Novel therapies require an understanding of the underlying mechanisms of sundowning and development of new therapeutic approaches. Research using mouse models is integral to expanding research on circadian aging from observation of outward rhythms to mechanistic studies. Mouse models represent a useful tool in understanding the mechanisms of circadian behavioral disorders in aging humans. Clinical studies are useful in their direct application; however, these studies are limited to establishing correlations between biological metrics and behavior, whereas animal research makes it possible to determine causative mechanisms of behavior. Most clinical studies are observational or retrospective (e.g., assaying post-mortem brain gene expression), but animal research allows studies of changes in hormones or neurotransmitters during the behavior itself. Research in mouse models furthermore provides opportunity to directly manipulate variables such as genes or environmental conditions. There are, however, limitations to using mouse models to study psychiatric disorders. Certain components of these disorders are impossible or very difficult to model in mice. For example, hallucinations or nighttime wandering are not easily evaluated in mice. And furthermore, some behaviors that we can demonstrate in a mouse model may not exactly replicate the human behavior. For these reasons, it is difficult for a single mouse model to completely replicate a complex psychiatric disorder. Nevertheless, it is useful to model specific symptoms using different mouse models, in order to dissect out the mechanisms of each behavior (Workman and Nelson, 2010). Establishing a useful mouse model requires satisfaction of three criteria of validity: face, construct, and predictive validity. Face validity is satisfied when the mouse model phenotype closely resembles the symptoms of the human disorder. Construct validity refers to similarities in the mouse model to the underlying mechanisms of the human disorder, for example certain genes are implicated in both the behavior of the model and the human disorder. Predictive validity requires that therapeutic treatments administered in the mouse model elicit a similar response as observed in human patients. An ideal mouse model satisfies each of these criteria, but a model can still be useful and offer insights into mechanisms if it only satisfies one or two of these criteria. The aim of this paper is to review mouse studies of circadian behavioral disturbances relevant to sundowning, in order to determine potential models for studying the mechanisms of sundowning syndrome. The emergence of a useful mouse model should facilitate the development of novel therapeutic approaches. What is sundowning? Sundowning syndrome, also referred to as “nocturnal delirium”, is characterized by a temporally specific pattern of recurring disruptive behaviors that can have many contributing causes (Fig. 1). Patients may become highly agitated, aggressive, restless, vocal, or delirious. These behaviors worsen specifically during the late afternoon or early evening, whereas symptoms improve or disappear during the day. Dementia patients are more often afflicted than any other group; however, cognitively-intact elderly individuals have also been reported to exhibit sundowning symptoms during hospitalization (Evans, 1987; Kim et al., 2005). Estimates of the prevalence of sundowning vary depending on disease state and living conditions. Reported rates among institutionalized patients range from 10 to 25% (Evans, 1987; Martin et al., 2000), whereas numbers are much higher, approximately 66%, for dementia patients living at home (Gallagher-Thompson et al., 1992). The greatest prevalence is observed among patients with severe dementia, in particular those living at home, rather than in a nursing home or other institution. It is unknown whether sundowning varies in prevalence by subtype of dementia and rates among cognitively intact individuals are difficult to obtain. The costs of sundowning syndrome are tremendous, both in terms of the financial burden placed on caretakers, the emotional distress caused to families, and the cost in quality of life for the patient. Sundowning symptoms are often cited as a main reason for families to move the patient from home into a skilled nursing facility (Coen et al., 1997; Pollak et al., 1990). In 2006, costs of care for each dementia patient were almost $1300 per month in the United States, with the severity of behavioral disturbances directly affecting the costs (Herrmann et al., 2006). Sundowning symptoms also cause emotional distress for family members. Caretakers are under high stress and at elevated risk for anxiety and depression (Gallagher-Thompson et al., Fig. 1. Possible contributors to sundowning symptoms. AVP: arginine vasopressin; VIP: vasoactive intestinal peptide. T.A. Bedrosian, R.J. Nelson / Experimental Neurology 243 (2013) 67–73 1992; Mahoney et al., 2005). Some symptoms of sundowning, such as physical aggression and agitation, may put professional caregivers (i.e., nurses, attendants, doctors) at a safety risk. Finally, sundowning syndrome is detrimental to the quality of life of the afflicted individual, especially because some behaviors such as wandering and physical aggression may compromise safety of the patient or lead to uncomfortable treatments like physical restraint. At present, treatment options for sundowning are limited, primarily because of our limited knowledge of the etiology and pathophysiology of this disorder. Clinical literature describes four main strategies to control sundowning symptoms, each with limited efficacy. First, light therapy may be somewhat useful in ameliorating the sleep–wake disturbance associated with sundowning. Reduced sensitivity to zeitgebers and degenerative pathology in the SCN occur in aging and dementia, thus stimulation with light therapy may help counteract these changes. One study administered bright light pulses to hospitalized Alzheimer disease patients experiencing sundowning and sleep disturbances (Satlin et al., 1992). The light therapy occurred between 19:00 and 21:00 for one week. Ratings of sundowning symptoms by trained nurses improved during and after the week of therapy in eight of ten subjects. Interestingly, the most severe sundowners displayed the most improvement after treatment. In contrast, a review of 8 trials using light therapy for managing cognitive and behavioral symptoms in dementia found insufficient evidence to support the value of light therapy (Forbes et al., 2009). Melatonin treatment has been used in several clinical studies to improve sundowning symptoms, in response to the hypothesis that it may help regulate sleep and synchronize rhythms. Open label pilot studies demonstrate improved daytime sleepiness and reduced evening agitation both by nursing staff reports and wrist actigraphy in samples of dementia patients residing in nursing homes (CohenMansfield et al., 2000; Mahlberg et al., 2004). Meta-analyses of the literature have revealed similar conclusions that melatonin treatment improves sundowning symptoms and disrupted sleep–wake cycles in dementia patients (Cardinali et al., 2010; de Jonghe et al., 2010). These studies mainly involve small pilot study samples or case reports, thus more extensive trials are necessary before making clinical recommendations. Atypical neuroleptics are an appealing choice to mollify a patient displaying extremely disruptive or aggressive behaviors. They are reportedly the most-prescribed pharmacotherapeutic in treating sundowning syndrome, despite little empirical evidence to support their use (Greve and O'Connor, 2005) and possible risks (Schneider et al., 2005). Given the reduced strength of the sleep–wake rhythm in aging and dementia, neuroleptics, which further weaken these rhythms, may ultimately be a poor choice of therapy. These drugs tend to enhance symptoms of confusion, impaired cognition, and excessive sedation (Ancoli-Israel and Kripke, 1989; Stoppe et al., 1999), and also may increase the duration of hospitalization (Yuen et al., 1997). More evidence toward the efficacy and biological mechanism of these drugs in sundowning is necessary to fully justify their use. Some evidence suggests donepezil, an acetylcholinesterase inhibitor, may be effective in improving sundowning symptoms. A case study report of a 71-year old man diagnosed with dementia with Lewy bodies demonstrated improved behavioral symptoms after treatment with donepezil (Skjerve and Nygaard, 2000). The patient exhibited sundowning symptoms as assessed by trained nurses and wrist activity measures. After 10 days of treatment with donepezil, behavioral symptoms improved and evening activity levels markedly decreased. Meta-analysis of the efficacy of cholinesterase inhibitors in treating neuropsychiatric symptoms in Alzheimer disease also found a beneficial impact of this treatment (Trinh et al., 2003). Though more extensive studies must be completed, it is possible that reduced cholinergic activity in aging and dementia may provoke circadian rhythm disturbances, such as sundowning, and that augmenting cholinergic function may counteract these changes. 69 Clinical research Sundowning was first reported in the clinical literature more than 70 years ago (Cameron, 1941), and since then many clinical studies and case reports have characterized the disorder. Most physicians and nursing staff recognize the phenomenon of sundowning as a legitimate syndrome; however, there has been some argument in the field (Khachiyants et al., 2011). Some researchers have questioned whether sundowning symptoms are only perceived worse near sundown by fatigued caregivers. This difference of opinions may reflect discrepancies between studies arising from varying settings or methods. Sundowning symptoms can be characterized by many different techniques, including caregiver questionnaires, retrospective chart review, and wrist actigraphy. In the current Diagnostic and Statistical Manual of Mental Disorders (DSM), sundowning remains a descriptor, rather than an independent psychiatric diagnosis, although its independent addition has been proposed. Evidence against sundowning as a legitimate syndrome comes from the notion that caregivers and nursing staff are particularly fatigued near the end of the day. Shift changes routinely occur around this time as well, giving rise to the possibility that disruptive behavior is only perceived worse at sundown due to fatigue and understaffing, and that there is no real temporal pattern to the behavior. One study investigated patterns of agitation by hour and season in dementia patients residing in nursing home facilities (Bliwise et al., 1993). Patients exhibited a consistent peak in agitation around 16:00, irrespective of the season. This suggested agitation was not tied to sundown because the peak occurred at the same clock time regardless of day length. The 16:00 peak corresponds to the time of nursing staff shift change, though the increase in agitation was a gradual slope, rather than a sharp peak. This was interpreted as reflective of the gradual tiring of nursing staff, leading up to the major disruption of shift change, though this pattern was only observed for the end of the day shift, not the evening shift. Alternatively, this increase in agitation could reflect a disconnect between the internal biological clock of elderly residents and external zeitgebers so that internal clock time did not entrain appropriately to the changing times of dusk. In contrast, many clinical studies support the notion of a legitimate sundowning syndrome. One study observed a peak in disruptive vocalizations, compulsive picking, and aggression among nursing home residents between 16:30 and 23:00 (Cohen-Mansfield, 2007). Interestingly, individualized patterns were observed among patients, despite the constant daily routine experienced by all, which suggests that there is a biological basis for the peak in symptoms. Other studies have also confirmed an afternoon or evening peak in behavioral symptoms using observation, retrospective chart review, accelerometry, and computer-assisted measurements (Burgio et al., 1994, 2001; Godfrey et al., 2010; Lebert et al., 1996; Martin et al., 2000; Nowak and Davis, 2007). Variability in the diagnostic criteria for sundowning syndrome may contribute to some of the discrepancy in opinion about its existence. A unified addition in the DSM would be useful in this regard. Pre-clinical research Pre-clinical studies investigating the biological basis of sundowning syndrome are lacking, despite the marked need for basic animal research to elucidate the mechanisms of this disorder. One likely explanation for the paucity of work in this field is the lack of an appropriate animal model. It has been difficult to model both the circadian and affective components of sundowning syndrome in mice. Also, as a nocturnal species, the timing of sundowning symptoms is reversed in mice relative to humans, meaning that sundowning would occur toward the end of the night (i.e., during the onset of the inactive phase) in mice versus the end of the day (i.e., onset of the inactive period) in humans. Thus far, only a few studies have successfully captured aspects of sundowning in mice. In particular, mouse models of Alzheimer 70 T.A. Bedrosian, R.J. Nelson / Experimental Neurology 243 (2013) 67–73 disease and of anxiety have been investigated as possible models for sundowning symptoms. Transgenic APP23 mice express a Thy-1 promoter to drive human APP751 cDNA encoding the Swedish double mutation K670N/M671L, implicated in familial AD (Sturchler-Pierrat et al., 1997). These mice develop hyperactivity relative to wild-type mice at the end of the active period in an age-dependent manner. Altered activity patterns begin to develop around 6 months of age and are quite prominent at 12 months (Vloeberghs et al., 2004). In comparison to human actigraphy data from probable AD patients exhibiting sundowning symptoms, the activity pattern is quite similar, making transgenic APP23 mice a potential model for sundowning activity disturbances, though the model lacks the affective component of the syndrome. Transgenic PDAPP mice express a platelet-derived growth factor promoter driving hβAPP minigene encoding for the 717v→F mutation implicated in familial AD (Sasahara et al., 1991). Sleep and wakefulness were measured in these mice using telemetry to evaluate electroencephalogram (EEG) and electromyographic (EMG) activity (HuitronResendiz et al., 2002). Data were shown in 3 h intervals across 24 h. At a young age of 5–6 months, preceding the development of amyloid plaques, PDAPP mice behaved similarly to non-transgenic mice in terms of time spent awake versus engaged in slow wave sleep. Aged PDAPP mice (20–26 months), however, spent more time awake and less time in slow wave sleep during the last part of the dark phase compared to age-matched non-transgenic mice. During the light phase, aged PDAPP were generally more wakeful, perhaps indicating fragmented sleep such as that seen in AD patients. Although the authors do not allude to the concept of sundowning in this study, it is interesting that the pattern of wakefulness observed among aged PDAPP mice might be interpreted as similar to that of the sundowning patient. Aged PDAPP mice and non-transgenic mice differed only during the very last part of the active period, not during earlier hours within the dark phase. This may be reminiscent of the increases in activity observed among sundowning patients, whereas a typical individual is “gearing down” during this time period. Alterations in cholinergic neurotransmission have been implicated in anxiety induction; muscarinic acetylcholine receptor antagonists are anxiogenic in rodents (Rodgers and Cole, 1995; Smythe et al., 1996), whereas nicotinic receptor agonists decrease anxiety (Brioni et al., 1993; Irvine et al., 1999; Szyndler et al., 2001) and acetylcholinesterase inhibitors reduce neophobia (Sienkiewicz-Jarosz et al., 2000). Scopolamine, a muscarinic receptor antagonist, administered to rodents provokes certain symptoms reminiscent of sundowning, though without the circadian component. For example, scopolamine-treated rats have been proposed as a delirium model (Nakamura et al., 2008); however, scopolamine also induces other symptoms more similar to schizophrenia or psychosis as well (Barak and Weiner, 2007). This model captures the delirium that sometimes manifests during an episode of sundowning, and may be useful in understanding the mechanism of that particular symptom. Interestingly, sundowning behavior may be related to the notion that dementia patients are more susceptible to psychosocial stress, leading to increased fear and anxiety. A triple-transgenic mouse model of AD (3×TgAD mice) was administered a chronic psychosocial stress regimen for 6 weeks, consisting of random changes in cage composition of group-housed mice (Rothman et al., 2012). Stress increased open-field anxiety-like behaviors in 3×TgAD mice and prolonged the corticosterone response to acute stress, but these responses were not observed in wild-type mice. These data suggest that AD patients may have heightened sensitivity to stressors, perhaps provoking anxiety and agitation. An interesting follow-up study would be to evaluate anxiety-like behaviors after acute psychosocial stress administered at different times throughout the day, in order to determine the effect of acute stress and whether time of day interacts with the anxiety response. A phenomenon of generalized CNS arousal has been proposed, in which more arousal corresponds to greater responsiveness to sensory stimuli, more motor activity, and greater emotional reactivity. Fluctuations of generalized arousal are the most obvious effects of circadian rhythms and sleep–wake cycles, in turn activating other behavioral responses which may lead to behavioral disorders in a pathological situation. Mice rendered brain-damaged using anoxia treatment and tested in a generalized arousal assay reduced fear behavior and reduced horizontal activity across the day, except for the end of the active phase, during which the mice were hyperactive (Arrieta-Cruz and Pfaff, 2009). This diurnal fluctuation in generalized arousal seen in post-anoxia mice, but not in control mice, is interpreted as reminiscent of sundowning syndrome in elderly adults. Wild-type C57BL6 mice aged 29-months and housed in static long-day lengths (14:10 L:D) increased homecage locomotor activity relative to middle-aged (9-month) control mice at the end of the active phase (Bedrosian et al., 2011b). Interestingly, when these mice are tested for anxiety-like behavior on an elevated plus maze at different times of the night, those aged mice tested late in the active phase display an exaggerated anxiety-like response compared to middle-aged mice tested at the same timepoint (Figs. 2C–E). In contrast, testing either age group at an earlier timepoint in the active phase reveals no differences in anxiety response, showing some temporal component to anxiety-response exists among aged mice. A similar pattern of behavior in the elevated plus maze is observed in APPSWE (Taconic) mice at 9 months of age, the same age at which amyloid plaques begin to accumulate in the brains of these mice (Hsiao et al., 1996). Potential mechanisms underlying sundowning At present, the neurobiological mechanisms underlying sundowning syndrome remain unspecified, but likely include several contributors. Sleep disruption may be one very important contributor (Staedt and Stoppe, 2005). Aging and dementia can lead to reduced consolidation of NREM sleep, decreased sleep efficiency, increased sleep disruptions, and episodes of nocturnal wandering, as well as elevated daytime napping (Klaffke and Staedt, 2006). These sleep-related disturbances are common with aging and often exacerbated by the presence of dementia. Over 38% of individuals aged 65 years and older report sleep disturbances (Foley et al., 1995) and this number is higher for those diagnosed with dementia (Tractenberg et al., 2003). Furthermore, cognition, affect, and sleep are closely related. In dementia patients, the disruption of normal sleep is correlated with the severity of dementia (Bliwise et al., 1995). Mood is also modulated by quality of sleep (Vandekerckhove and Cluydts, 2010). For example, mild sleep deprivation increases negative affect, including depression, anxiety, paranoia, and somatic complaints (Kahn-Greene et al., 2007). It also enhances negative emotional reactivity and subdues positive reactions to positive events (Zohar et al., 2005). Reduced zeitgebers contribute to sleep disturbances and impaired synchronization in a variety of daily rhythms. For example, many aged individuals, particularly dementia patients, are bound to their homes and experience relatively constant dim light exposure. Because of the lack of exposure to bright light outdoors and chronic exposure to dim indoor illumination, elderly individuals frequently lack sufficient lighting to entrain and reset the circadian system. Level of light exposure has been positively associated with stability of the sleep–wake rhythm in dementia patients, pointing to the importance of light as a zeitgeber in this population (Ancoli-Israel et al., 2003). Nevertheless, in some nursing homes, median light intensity reaches only 54 lx, in comparison to 300–500 lx measured in workplaces or 3000–4000 lx outdoors in the winter (Shochat et al., 2000; Staedt and Stoppe, 2005). Intensities of ~ 180 lx are required to significantly phase shift the human circadian clock (Boivin et al., 1996). At least one study, however, has reported that healthy elderly individuals are actually exposed to higher levels of light than healthy young adults; but this group also experienced greater light at night T.A. Bedrosian, R.J. Nelson / Experimental Neurology 243 (2013) 67–73 71 Fig. 2. Sundowning-like behaviors in aged mice. Aged mice (29 months) are more active than middle-aged adults (7 months) during the last part of the dark (active) phase, between 23:00 and 01:00 (A–B). Arrows in A indicate the times at which anxiety testing was performed. Aged mice tested at the end of active phase exhibit more anxiety-like behaviors in the elevated plus maze than aged mice tested early in the dark phase or middle-aged adult mice tested at either time, in terms of duration spent in the open arms (C), number of open arm entries (D), and latency to first enter the open arms (E). Activity graph (A) depicts mean ± SD and bar graphs depict mean ± SEM. *p b 0.05; † p b 0.05 Aged Late vs. All other groups; ††p b 0.01 Aged Late vs. All other groups. For activity, N = 10–13 mice per group. For anxiety, N = 3–7 mice per group. Adapted from Bedrosian et al. (2011b). exposure (Scheuermaier et al., 2010). Disruptive lighting during the night, especially in nursing homes, can also impair sleep and disrupt circadian timing. There is evidence for negative effects of light at night on mood in rodent models as well (Bedrosian et al., 2011a). Complicating matters, reductions in melatonin production and melatonin receptor sensitivity have been reported in aging individuals, which may further disrupt regulation of sleep and wake (Skene and Swaab, 2003; Wu and Swaab, 2005). Also, age-related changes in lens opacity decrease transmission of short-wavelength light to the retina (Charman, 2003). Short-wavelength (i.e., blue light) most potently entrains the circadian system (Hattar et al., 2003), so reductions in these wavelengths may have detrimental effects for circadian timekeeping. Furthermore, napping, reduced physical activity, and lack of daily routine can all contribute to a disrupted sleep–wake cycle. The suprachiasmatic nuclei (SCN), comprising the body's master circadian clock, undergo age-related degenerative changes which further contribute to overall circadian dysregulation. Reduced cholinergic input to the SCN from the nucleus basalis of Meynert (NBM) impairs neuropeptide synthesis and expression (Madeira et al., 2004). This impaired activity of the SCN, along with reduced external zeitgebers, disrupts a variety of biological rhythms. For this reason, bright light therapy has been suggested as a possible therapy for age-related circadian disorders and sundowning, as was described above. Interestingly, there is some evidence to relate decreased SCN output to sundowning syndrome. Break-down of the circadian rhythm in body temperature, especially reduced amplitude and phase delays, correlates with worsening of sundowning symptoms (Volicer et al., 2001). Neuropathology within the NBM may also affect sleep and sundowning behavior in dementia patients. The NBM is part of the ascending reticular activating system and sends cholinergic projections to the prefrontal cortex (Wenk, 1997) to modulate arousal. It undergoes major degenerative changes and loss of cholinergic activity in Alzheimer disease (McGeer et al., 1984). Thus, one theory is that disrupted rest–activity rhythms in conjunction with disrupted arousal and attentional processes may combine at the end of the day to contribute to agitation and sundowning symptoms (Staedt and Stoppe, 2005). Klaffke and Staedt (2006) have proposed an interesting theory on the pathophysiology of sundowning syndrome based on the circadian disturbances mentioned above. They suggest that sundowning in Alzheimer disease is precipitated by a desynchronization of arousal processes and the rest–activity rhythm. Arousal, such as anxiety produced by the environment, may rise at the end of the day due to nursing staff shift changes, impaired visual orientation due to decreased lighting, or a variety of other disruptions. At the same time, the neocortex is “turned off” in preparation for sleep, an effect of poorly entrained sleep–wake cycles and decreased cholinergic input to the cortex by the NBM. The patient thus lacks the attentional capacity to process the arousal and anxiety, which further augments the agitation symptoms. Aged mice exhibiting sundowning-like symptoms have increased expression of acetylcholinesterase in the NBM (Fig. 3), which temporally coincides with the behavior, as well as overall reductions in NBM choline acetyltransferase expression, lending some support to this theory (Bedrosian et al., 2011b). Future directions Sundowning syndrome is a complex behavioral disorder affecting elderly individuals, with tremendous costs for families, caretakers, and patients themselves. Without a strong mouse model to use in investigating the pathophysiology of this disorder, it will be difficult to develop new therapeutic options, which are greatly needed. An ideal mouse model must display both the circadian and affective components of sundowning. Several models presented in this review exhibited either circadian locomotor activity changes, without measurement of any affective behaviors, or exhibited affective changes without a circadian component. The combination of both factors is at the core of sundowning syndrome and should be represented in a strong mouse model. Furthermore, ideally the symptoms of sundowning should be modeled in a transgenic mouse expressing dementia-like brain pathology, as dementia patients are the most 72 T.A. Bedrosian, R.J. Nelson / Experimental Neurology 243 (2013) 67–73 Fig. 3. Acetylcholinesterase staining in nucleus basalis of Meynert (NBM) of aged mice. Relative optical density was quantified in sections containing the NBM (A). Aged mice had greater AchE expression late in the dark phase compared to other groups (B), coinciding with the sundowning-like behavioral changes observed (see Fig. 2). Images captured at 10 ×. Scale bar = 100 μm. Graph depicts mean relative optical density ± SEM. *p b 0.05. NBM: nucleus basalis of Meynert; opt: optic tract; f: fornix. N = 3–6 mice per group. Adapted from Bedrosian et al. (2011b). commonly afflicted group. Such a model would provide the opportunity to gain insight into the mechanisms of this complex circadian disorder. Acknowledgments We thank Dr. Zachary M. Weil for comments on this manuscript. TAB was supported by a National Defense Science and Engineering Graduate fellowship and RJN was supported by NIH grant RO1MH057535 and NSF grant IOS-08-38098 during the preparation of this review. References Ancoli-Israel, S., Kripke, D.F., 1989. Now I lay me down to sleep: the problem of sleep fragmentation in the elderly and demented residents of nursing homes. Bull. Clin. Neurosci. 127–132. Ancoli-Israel, S., Gehrman, P., Martin, J.L., Shochat, T., Marler, M., Corey-Bloom, J., Levi, L., 2003. Increased light exposure consolidates sleep and strengthens circadian rhythms in severe Alzheimer's disease patients. Behav. Sleep Med. 1, 22–36. Arrieta-Cruz, I., Pfaff, D.W., 2009. Definition of arousal and mechanistic studies in intact and brain-damaged mice. Ann. N. Y. Acad. Sci. 1157, 24–31. Bachman, D., Rabins, P., 2006. “Sundowning” and other temporally associated agitation states in dementia patients. Annu. Rev. Med. 57, 499–511. Barak, S., Weiner, I., 2007. Scopolamine induces disruption of latent inhibition which is prevented by antipsychotic drugs and an acetylcholinesterase inhibitor. Neuropsychopharmacology 32, 989–999. Bedrosian, T.A., Fonken, L.K., Walton, J.C., Haim, A., Nelson, R.J., 2011a. Dim light at night provokes depression-like behaviors and reduces CA1 dendritic spine density in female hamsters. Psychoneuroendocrinology 36, 1062–1069. Bedrosian, T.A., Herring, K.L., Weil, Z.M., Nelson, R.J., 2011b. Altered temporal patterns of anxiety in aged and amyloid precursor protein (APP) transgenic mice. Proc. Natl. Acad. Sci. U. S. A. 108, 11686–11691. Benca, R., Duncan, M.J., Frank, E., McClung, C., Nelson, R.J., Vicentic, A., 2009. Biological rhythms, higher brain function, and behavior: gaps, opportunities, and challenges. Brain Res. Rev. 62, 57–70. Bliwise, D.L., Carroll, J.S., Lee, K.A., Nekich, J.C., Dement, W.C., 1993. Sleep and “sundowning” in nursing home patients with dementia. Psychiatry Res. 48, 277–292. Bliwise, D.L., Hughes, M., McMahon, P.M., Kutner, N., 1995. Observed sleep/wakefulness and severity of dementia in an Alzheimer's disease special care unit. J. Gerontol. A Biol. Sci. Med. Sci. 50, M303–M306. Bliwise, D.L., Mercaldo, N.D., Avidan, A.Y., Boeve, B.F., Greer, S.A., Kukull, W.A., 2011. Sleep disturbance in dementia with Lewy bodies and Alzheimer's disease: a multicenter analysis. Dement. Geriatr. Cogn. Disord. 31, 239–246. Boivin, D.B., Duffy, J.F., Kronauer, R.E., Czeisler, C.A., 1996. Dose–response relationships for resetting of human circadian clock by light. Nature 379, 540–542. Brioni, J.D., O'Neill, A.B., Kim, D.J., Decker, M.W., 1993. Nicotinic receptor agonists exhibit anxiolytic-like effects on the elevated plus-maze test. Eur. J. Pharmacol. 238, 1–8. Burgio, L.D., Scilley, K., Hardin, J.M., Janosky, J., Bonino, P., Slater, S.C., Engberg, R., 1994. Studying disruptive vocalization and contextual factors in the nursing home using computer-assisted real-time observation. J. Gerontol. 49, P230–P239. Burgio, L.D., Scilley, K., Hardin, J.M., Hsu, C., 2001. Temporal patterns of disruptive vocalization in elderly nursing home residents. Int. J. Geriatr. Psychiatry 16, 378–386. Cameron, D., 1941. Studies in senile nocturnal delirium. Psychiatr. Q. 15, 47–53. Cardinali, D.P., Furio, A.M., Brusco, L.I., 2010. Clinical aspects of melatonin intervention in Alzheimer's disease progression. Curr. Neuropharmacol. 8, 218–227. Charman, W.N., 2003. Age, lens transmittance, and the possible effects of light on melatonin suppression. Ophthalmic. Physiol. Opt. 23, 181–187. Coen, R.F., Swanwick, G.R., O'Boyle, C.A., Coakley, D., 1997. Behaviour disturbance and other predictors of carer burden in Alzheimer's disease. Int. J. Geriatr. Psychiatry 12, 331–336. Cohen-Mansfield, J., 2007. Temporal patterns of agitation in dementia. Am. J. Geriatr. Psychiatry 15, 395–405. Cohen-Mansfield, J., Garfinkel, D., Lipson, S., 2000. Melatonin for treatment of sundowning in elderly persons with dementia — a preliminary study. Arch. Gerontol. Geriatr. 31, 65–76. de Jonghe, A., Korevaar, J.C., van Munster, B.C., de Rooij, S.E., 2010. Effectiveness of melatonin treatment on circadian rhythm disturbances in dementia. Are there implications for delirium? A systematic review. Int. J. Geriatr. Psychiatry 25, 1201–1208. Donaldson, C., Tarrier, N., Burns, A., 1998. Determinants of carer stress in Alzheimer's disease. Int. J. Geriatr. Psychiatry 13, 248–256. Evans, L.K., 1987. Sundown syndrome in institutionalized elderly. J. Am. Geriatr. Soc. 35, 101–108. Finkel, S., 2000. Introduction to behavioural and psychological symptoms of dementia (BPSD). Int. J. Geriatr. Psychiatry 15 (Suppl. 1), S2–S4. Foley, D.J., Monjan, A.A., Brown, S.L., Simonsick, E.M., Wallace, R.B., Blazer, D.G., 1995. Sleep complaints among elderly persons: an epidemiologic study of three communities. Sleep 18, 425–432. Forbes, D., Culum, I., Lischka, A.R., Morgan, D.G., Peacock, S., Forbes, J., Forbes, S., 2009. Light therapy for managing cognitive, sleep, functional, behavioural, or psychiatric disturbances in dementia. Cochrane Database Syst. Rev. CD003946. Gallagher-Thompson, D., Brooks III, J.O., Bliwise, D., Leader, J., Yesavage, J.A., 1992. The relations among caregiver stress, “sundowning” symptoms, and cognitive decline in Alzheimer's disease. J. Am. Geriatr. Soc. 40, 807–810. Godfrey, A., Leonard, M., Donnelly, S., Conroy, M., Olaighin, G., Meagher, D., 2010. Validating a new clinical subtyping scheme for delirium with electronic motion analysis. Psychiatry Res. 178, 186–190. Greve, M., O'Connor, D., 2005. A survey of Australian and New Zealand old age psychiatrists' preferred medications to treat behavioral and psychological symptoms of dementia (BPSD). Int. Psychogeriatr. 17, 195–205. Hatfield, C.F., Herbert, J., van Someren, E.J., Hodges, J.R., Hastings, M.H., 2004. Disrupted daily activity/rest cycles in relation to daily cortisol rhythms of home-dwelling patients with early Alzheimer's dementia. Brain 127, 1061–1074. Hattar, S., Lucas, R.J., Mrosovsky, N., Thompson, S., Douglas, R.H., Hankins, M.W., Lem, J., Biel, M., Hofmann, F., Foster, R.G., Yau, K.W., 2003. Melanopsin and rod-cone photoreceptive systems account for all major accessory visual functions in mice. Nature 424, 76–81. Herrmann, N., Lanctot, K.L., Sambrook, R., Lesnikova, N., Hebert, R., McCracken, P., Robillard, A., Nguyen, E., 2006. The contribution of neuropsychiatric symptoms to the cost of dementia care. Int. J. Geriatr. Psychiatry 21, 972–976. T.A. Bedrosian, R.J. Nelson / Experimental Neurology 243 (2013) 67–73 Hsiao, K., Chapman, P., Nilsen, S., Eckman, C., Harigaya, Y., Younkin, S., Yang, F., Cole, G., 1996. Correlative memory deficits, Abeta elevation, and amyloid plaques in transgenic mice. Science 274, 99–102. Huitron-Resendiz, S., Sanchez-Alavez, M., Gallegos, R., Berg, G., Crawford, E., Giacchino, J.L., Games, D., Henriksen, S.J., Criado, J.R., 2002. Age-independent and age-related deficits in visuospatial learning, sleep–wake states, thermoregulation and motor activity in PDAPP mice. Brain Res. 928, 126–137. Irvine, E.E., Cheeta, S., File, S.E., 1999. Time-course of changes in the social interaction test of anxiety following acute and chronic administration of nicotine. Behav. Pharmacol. 10, 691–697. Kahn-Greene, E.T., Killgore, D.B., Kamimori, G.H., Balkin, T.J., Killgore, W.D., 2007. The effects of sleep deprivation on symptoms of psychopathology in healthy adults. Sleep Med. 8, 215–221. Khachiyants, N., Trinkle, D., Son, S.J., Kim, K.Y., 2011. Sundown syndrome in persons with dementia: an update. Psychiatry Investig. 8, 275–287. Kim, P., Louis, C., Muralee, S., Tampi, R., 2005. Sundowning syndrome in the older patient. Clin. Geriatr. 13, 32–36. Klaffke, S., Staedt, J., 2006. Sundowning and circadian rhythm disorders in dementia. Acta Neurol. Belg. 106, 168–175. Lebert, F., Pasquier, F., Petit, H., 1996. Sundowning syndrome in demented patients without neuroleptic therapy. Arch. Gerontol. Geriatr. 22, 49–54. Madeira, M.D., Pereira, P.A., Silva, S.M., Cadete-Leite, A., Paula-Barbosa, M.M., 2004. Basal forebrain neurons modulate the synthesis and expression of neuropeptides in the rat suprachiasmatic nucleus. Neuroscience 125, 889–901. Mahlberg, R., Kunz, D., Sutej, I., Kuhl, K.P., Hellweg, R., 2004. Melatonin treatment of day–night rhythm disturbances and sundowning in Alzheimer disease: an openlabel pilot study using actigraphy. J. Clin. Psychopharmacol. 24, 456–459. Mahoney, R., Regan, C., Katona, C., Livingston, G., 2005. Anxiety and depression in family caregivers of people with Alzheimer disease: the LASER-AD study. Am. J. Geriatr. Psychiatry 13, 795–801. Martin, J., Marler, M., Shochat, T., Ancoli-Israel, S., 2000. Circadian rhythms of agitation in institutionalized patients with Alzheimer's disease. Chronobiol. Int. 17, 405–418. McGeer, P.L., McGeer, E.G., Suzuki, J., Dolman, C.E., Nagai, T., 1984. Aging, Alzheimer's disease, and the cholinergic system of the basal forebrain. Neurology 34, 741–745. Nakamura, K., Kurasawa, M., Tanaka, Y., 2008. Scopolamine model of delirium in rats and reversal of the performance impairment by aniracetam. Drug Dev. Res. 43, 85–97. Nakamura, T.J., Nakamura, W., Yamazaki, S., Kudo, T., Cutler, T., Colwell, C.S., Block, G.D., 2011. Age-related decline in circadian output. J. Neurosci. 31, 10201–10205. Nowak, L., Davis, J.E., 2007. A qualitative examination of the phenomenon of sundowning. J. Nurs. Scholarsh. 39, 256–258. Pollak, C.P., Perlick, D., 1991. Sleep problems and institutionalization of the elderly. J. Geriatr. Psychiatry Neurol. 4, 204–210. Pollak, C.P., Perlick, D., Linsner, J.P., Wenston, J., Hsieh, F., 1990. Sleep problems in the community elderly as predictors of death and nursing home placement. J. Community Health 15, 123–135. Rodgers, R.J., Cole, J.C., 1995. Effects of scopolamine and its quaternary analogue in the murine elevated plus-maze test of anxiety. Behav. Pharmacol. 6, 283–289. Rothman, S.M., Herdener, N., Camandola, S., Texel, S.J., Mughal, M.R., Cong, W.N., Martin, B., Mattson, M.P., 2012. 3×TgAD mice exhibit altered behavior and elevated Abeta after chronic mild social stress. Neurobiol. Aging 33 (4), 830.e1–830.e12. Sasahara, M., Fries, J.W., Raines, E.W., Gown, A.M., Westrum, L.E., Frosch, M.P., Bonthron, D.T., Ross, R., Collins, T., 1991. PDGF B-chain in neurons of the central nervous system, posterior pituitary, and in a transgenic model. Cell 64, 217–227. Satlin, A., Volicer, L., Ross, V., Herz, L., Campbell, S., 1992. Bright light treatment of behavioral and sleep disturbances in patients with Alzheimer's disease. Am. J. Psychiatry 149, 1028–1032. Scheuermaier, K., Laffan, A.M., Duffy, J.F., 2010. Light exposure patterns in healthy older and young adults. J. Biol. Rhythms 25, 113–122. 73 Schneider, L.S., Dagerman, K.S., Insel, P., 2005. Risk of death with atypical antipsychotic drug treatment for dementia: meta-analysis of randomized placebo-controlled trials. JAMA 294, 1934–1943. Shochat, T., Martin, J., Marler, M., Ancoli-Israel, S., 2000. Illumination levels in nursing home patients: effects on sleep and activity rhythms. J. Sleep Res. 9, 373–379. Sienkiewicz-Jarosz, H., Czlonkowska, A.I., Siemiatkowski, M., Maciejak, P., Szyndler, J., Plaznik, A., 2000. The effects of physostigmine and cholinergic receptor ligands on novelty-induced neophobia. J. Neural. Transm. 107, 1403–1412. Silva, R.H., Kameda, S.R., Carvalho, R.C., Takatsu-Coleman, A.L., Niigaki, S.T., Abilio, V.C., Tufik, S., Frussa-Filho, R., 2004. Anxiogenic effect of sleep deprivation in the elevated plus-maze test in mice. Psychopharmacology (Berl) 176, 115–122. Skene, D.J., Swaab, D.F., 2003. Melatonin rhythmicity: effect of age and Alzheimer's disease. Exp. Gerontol. 38, 199–206. Skjerve, A., Nygaard, H.A., 2000. Improvement in sundowning in dementia with Lewy bodies after treatment with donepezil. Int. J. Geriatr. Psychiatry 15, 1147–1151. Smythe, J.W., Murphy, D., Bhatnagar, S., Timothy, C., Costall, B., 1996. Muscarinic antagonists are anxiogenic in rats tested in the black-white box. Pharmacol. Biochem. Behav. 54, 57–63. Staedt, J., Stoppe, G., 2005. Treatment of rest–activity disorders in dementia and special focus on sundowning. Int. J. Geriatr. Psychiatry 20, 507–511. Stoppe, G., Brandt, C.A., Staedt, J.H., 1999. Behavioural problems associated with dementia: the role of newer antipsychotics. Drugs Aging 14, 41–54. Sturchler-Pierrat, C., Abramowski, D., Duke, M., Wiederhold, K.H., Mistl, C., Rothacher, S., Ledermann, B., Burki, K., Frey, P., Paganetti, P.A., Waridel, C., Calhoun, M.E., Jucker, M., Probst, A., Staufenbiel, M., Sommer, B., 1997. Two amyloid precursor protein transgenic mouse models with Alzheimer disease-like pathology. Proc. Natl. Acad. Sci. U. S. A. 94, 13287–13292. Szyndler, J., Sienkiewicz-Jarosz, H., Maciejak, P., Siemiatkowski, M., Rokicki, D., Czlonkowska, A.I., Plaznik, A., 2001. The anxiolytic-like effect of nicotine undergoes rapid tolerance in a model of contextual fear conditioning in rats. Pharmacol. Biochem. Behav. 69, 511–518. Tractenberg, R.E., Singer, C.M., Cummings, J.L., Thal, L.J., 2003. The Sleep Disorders Inventory: an instrument for studies of sleep disturbance in persons with Alzheimer's disease. J. Sleep Res. 12, 331–337. Trinh, N.H., Hoblyn, J., Mohanty, S., Yaffe, K., 2003. Efficacy of cholinesterase inhibitors in the treatment of neuropsychiatric symptoms and functional impairment in Alzheimer disease: a meta-analysis. JAMA 289, 210–216. Van Someren, E.J., 2000. Circadian and sleep disturbances in the elderly. Exp. Gerontol. 35, 1229–1237. Vandekerckhove, M., Cluydts, R., 2010. The emotional brain and sleep: an intimate relationship. Sleep Med. Rev. 14, 219–226. Vitiello, M.V., Borson, S., 2001. Sleep disturbances in patients with Alzheimer's disease: epidemiology, pathophysiology and treatment. CNS Drugs 15, 777–796. Vloeberghs, E., Van Dam, D., Engelborghs, S., Nagels, G., Staufenbiel, M., De Deyn, P.P., 2004. Altered circadian locomotor activity in APP23 mice: a model for BPSD disturbances. Eur. J. Neurosci. 20, 2757–2766. Volicer, L., Harper, D.G., Manning, B.C., Goldstein, R., Satlin, A., 2001. Sundowning and circadian rhythms in Alzheimer's disease. Am. J. Psychiatry 158, 704–711. Wenk, G.L., 1997. The nucleus basalis magnocellularis cholinergic system: one hundred years of progress. Neurobiol. Learn. Mem. 67, 85–95. Workman, J.L., Nelson, R.J., 2010. Potential animal models of seasonal affective disorder. Neurosci. Biobehav. Rev. 35, 669–679. Wu, Y.H., Swaab, D.F., 2005. The human pineal gland and melatonin in aging and Alzheimer's disease. J. Pineal Res. 38, 145–152. Yuen, E.J., Zisselman, M.H., Louis, D.Z., Rovner, B.W., 1997. Sedative-hypnotic use by the elderly: effects on hospital length of stay and costs. J. Ment. Health Adm. 24, 90–97. Zohar, D., Tzischinsky, O., Epstein, R., Lavie, P., 2005. The effects of sleep loss on medical residents' emotional reactions to work events: a cognitive-energy model. Sleep 28, 47–54.