Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
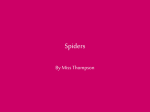
Review Laboratory Testing in Monitoring the Effects of Brown Recluse Spider Bites Amy L. Thompson, PhD, MLS(ASCP) ABSTRACT Most people regard brown recluse spiders as dangerous; however, the risk associated with its bite is not widely understood. Brown recluse spiders are among the genus Loxosceles, a group of brown spiders. All spiders in this genus have a violin or fiddle marking on their dorsal cephalothorax (back surface) and are often referred to as fiddleback spiders, but the brown recluse is considered the most dangerous to humans (Image 1). Brown recluse spider venom is more toxic than rattlesnake venom, but the quantity of spider venom injected in the bite of a brown recluse is typically smaller than the venom delivered in a rattlesnake bite. The brown recluse (Loxosceles reclusa) is found in the central United States, including Tennessee, Arkansas, Missouri, Oklahoma, and Kentucky, and may be accidentally transported to areas where it is not endemic (Image 2). Brown recluse spider bites in areas where the spiders are not endemic are rare.1-4 DOI: 10.1309/LMKIW3WIOO13EMMM Abbreviations ELISA, enzyme-linked immunosorbent assay; CBC, complete blood count; DAT, direct antiglobulin test; ALT, alanine transaminase; AST, aspartate aminotransferase; LDH, lactate dehydrogenase; CK, creatine kinase; DIC, disseminated intravascular coagulation; PT, prothrombin time; PTT, partial thromboplastin time; ESR, erythrocyte sedimentation rate; G6PD, glucose-6 phosphate dehydrogenase Department of Biology, Austin Peay State University, Clarksville, TN *To whom correspondence should be addressed. E-mail: [email protected] 300 3-Review_Amjad.indd 300 Lab Medicine Fall 2013 | Volume 44, Number 4 Key words: Spider bites, wounds, brown recluse spider The brown recluse is known for its reclusive behavior and prefers dark, secluded locations, such as in closets; under furniture; in folded clothing or in shoes; and in basements, garages, and crawl spaces. Human bites usually occur when the spider is inadvertently pressed against the skin, sometimes by getting trapped in clothing or in bed linens.1-4 Unlike most other spiders, the brown recluse prefers to consume dead prey rather than to hunt living creatures. The brown recluse spider does not trap its food in a web, but rather spins haphazard webs only for the purpose of laying its eggs.2 When the spider hunts, it bites and injects venom, then leaves, returning later to feed on its prey.5 For this reason humans who are bitten by the brown recluse often do not see the spider. To confirm a brown recluse spider bite, it is important to collect the spider and bring it to a specialist for identification. Only 10% of bite victims do this; some victims might not realize they have been bitten until later, or cannot find the spider.1,6,7 If the spider is not caught and brought in for confirmation, diagnosis is based on the patient’s report, wound appearance, and other signs and symptoms. Although a diagnostic test for Loxosceles reclusa bite is not available in clinical laboratories, an enzyme-linked immunosorbent assay (ELISA) has been developed to detect brown recluse spider venom. This test may have potential for clinical application, using samples collected by swabbing the bite site.8 Without the spider, the diagnosis often is reported as “presumptive brown recluse spider bite.” Some reports suggest that 80% of reported brown recluse bites were caused by another type of spider or insect or were actually not a bite at all.1,6,7 www.labmedicine.com 10/7/13 5:12 PM Downloaded from http://labmed.oxfordjournals.org/ by guest on October 13, 2016 Brown recluse spiders are endemic to the central United States and are highly venomous. Although most brown recluse spider bites do not cause dangerous wounds or systemic symptoms, severe cases can occur. Changes in laboratory values may include hemolysis, thrombocytopenia, coagulopathy, and altered chemistry and urinalysis results. Neutrophil involvement in wound progression and white blood cell changes can be observed. If blood products are indicated, fresh frozen plasma and cryoprecipitate should be avoided. There is no single clinical lab test that can be used to diagnose a brown recluse spider bite, but laboratory involvement in monitoring progression and treatment may be significant. Review Image 1 Brown recluse spider. Note fiddle marking on dorsal cephalothorax. Source: Wikipedia (Brown Recluse Spider), http://en.wikipedia.org/wiki/File:Brown-recluse-2-edit.jpg. Downloaded from http://labmed.oxfordjournals.org/ by guest on October 13, 2016 Image 2 Brown recluse spider endemic areas. Brown recluse spider bites are unlikely outside endemic areas. Source: Wikipedia (Brown Recluse Spider), http://upload.wikimedia.org/wikipedia/ commons/d/d9/Loxosceles_reclusa_range.png. Initial Bite and Progression of Wound A brown recluse bite and envenomation has been described as a pinprick with or without stinging and pain, although some victims felt nothing at all.1,3,9 The envenomated area may become swollen, red, and itchy. The bite usually develops a purple center (local thrombosis), surrounded by a red ring, like a bull’s eye, and a white blister will emerge. Unlike most skin wounds, the brown recluse bite is dry with little or no drainage. The center eventually retracts into a lighter center with irregular dark edges surrounded by redness. The red area may be surrounded by a white or blanched area due to vasoconstriction and ischemia, creating a red, white, and blue appearance. Bruising often appears along the local lymphatic vessels (Image 3). In rare cases, the wound can become necrotic, turning black. Many people are familiar with this dramatic result of brown recluse spider bites, although development into a www.labmedicine.com 3-Review_Amjad.indd 301 necrotic lesion is not common. The severity of symptoms depends on each individual victim’s immune response and the amount of venom injected by the spider; 90% of bites heal without complications. Three percent of brown recluse bites, however, eventually require a skin graft.1,3 The bite may go unnoticed for 6 to 8 hours, with the wound changing over a period of days to weeks; complete healing may require weeks to months and years in some cases. Neutrophil activation and granular secretion exacerbate the effects seen with these bites. Treatment of brown recluse spider bites often involves a wait-and-see approach, since the bite typically gets worse over a period of days and then begins to heal.1-3 Systemic Loxoscelism Systemic symptoms (systemic loxoscelism) are observed in fewer than 1% of brown recluse bites and are mostly seen Fall 2013 | Volume 44, Number 4 Lab Medicine 301 10/7/13 5:12 PM Review Image 3 Brown recluse spider bite day 12 of patient on prednisone. Note angry redness with white blanching and sinking in of center. Image provided by Amy L. Thompson. Laboratory Testing Although no single laboratory test can be used to diagnose a brown recluse spider bite, the laboratory is involved in more severe bite cases involving necrosis or when systemic symptoms exist. Important laboratory parameters potentially involve red blood cells, white blood cells, platelets, bilirubin, liver enzymes, and urinalysis.3,7,9 Red Blood Cell Changes Complete blood counts (CBCs) taken over several days are important to document changes associated with the poisoning. Hemolysis potentially leading to hemolytic anemia is sometimes observed with brown recluse spider bites due to sphingomyelinase D activity as previously described. Intravascular and/or extravascular hemolysis may be observed and laboratory testing will be helpful in determining whether either type is occurring. The plasma-free hemoglobin test or serum haptoglobin can be used to monitor hemolysis and differentiate between intravascular and extravascular states. Increased levels of plasma-free hemoglobin are suggestive of intravascular 302 3-Review_Amjad.indd 302 Lab Medicine Fall 2013 | Volume 44, Number 4 hemolysis, since normally little to no free hemoglobin is observed in plasma. Since haptoglobin binds free hemoglobin in the blood, decreased levels of haptoglobin suggest intravascular hemolysis, whereas normal levels of haptoglobin suggest extravascular hemolysis.3,7,9 The Direct Coombs’ Test (direct antiglobulin test or DAT) result is variable among brown recluse spider bite patients and may be positive or negative, with positive results suggesting that complement or antibodies are present on the red blood cell surface. One study suggested that interleukin-8, the factor that attracts neutrophils, and granulocyte-macrophage colony stimulating factor, the cytokine that stimulates granulocyte production, might be involved in this process.3,12,13 For patients requiring blood products, packed red blood cells should be used in place of fresh frozen plasma or cryoprecipitate, since both contain complement and may worsen hemolysis.7 Chemistry and Urinalysis Changes Increased total and indirect bilirubin levels often result from hemolysis.12 Another potential finding is elevated liver enzymes, including alanine transaminase (ALT) and aspartate aminotransferase (AST). If liver enzymes are elevated, supportive treatment should not include potentially hepatotoxic medications. Elevated lactate dehydrogenase (LDH) is consistent with hemolysis.7 Urinalysis may reveal hemoglobinuria, but not hematuria, as a result of hemolysis.2,9 Urine may be dark and high levels of urobilinogen may be present, suggesting extravascular hemolysis.7 Myoglobin may be found in the urine due to rhabdomyolysis and corresponding elevated blood creatine kinase (CK) may be noted.12 Platelet and Coagulation Changes Thrombocytopenia occurs due to platelet activation by sphingomyelinase D.4 The presence of elevated fibrin degradation products, such as the D-dimer, is suggestive of disseminated intravascular coagulation (DIC). Prothrombin www.labmedicine.com 10/7/13 5:12 PM Downloaded from http://labmed.oxfordjournals.org/ by guest on October 13, 2016 in children, elderly individuals, and immunocompromised patients. Systemic symptoms include fever, chills, nausea, vomiting, anorexia, malaise, arthralgia, myalgia, cellulitis, and a morbilliform rash. Brown recluse spider venom contains sphingomyelinase D, which converts erythrocytic membrane sphingomyelin to ceramide-1-phosphate, leading to hemolysis; platelet aggregation, and thrombosis. Damage to myelin may cause pain and interruption of nerve conduction. Although rare, pulmonary edema may occur as a result of sphingomyelinase D activity in the lungs; acute renal failure has also been reported. Even though systemic loxoscelism is not common, it is important for those suspecting a brown recluse bite to seek medical assistance, as necrosis and systemic loxoscelism can be severe.3,7,9-11 Review time (PT) and partial thromboplastin time (PTT) may be elevated or normal. If not treated promptly, DIC can lead to acute renal failure, multiple organ failure, and death.7,12 White Blood Cells and Inflammation Mild leukocytosis is common in brown recluse spider bites, although leukopenia may be observed.2,7 The erythrocyte sedimentation rate (ESR) often is elevated, supporting the presence of an inflammatory response. A skin biopsy of the wound typically reveals eosinophils and neutrophils, along with thrombosis and inflammation of subcutaneous adipose (fat).2 for all healthcare professionals, especially those in brown recluse spider endemic areas, to recognize the signs of a brown recluse bite and the clinical symptoms it may produce. In severe cases, particularly those involving hemolytic changes, the laboratory is important for monitoring the progression of disease and potential side effects of drugs used to treat the inflammatory response and hemolysis. Laboratory professionals should be aware of necessary requirements to prevent exacerbation of patient symptoms, such as G6PD with dapsone therapy, and avoiding fresh frozen plasma and cryoprecipitate. LM Treatment The treatments for a brown recluse spider bite are as varied as the symptoms. Some healthcare providers recommend the use of dapsone, which inhibits neutrophil migration, attachment to the endothelium, and granular secretion. Because of the hemolytic effects of dapsone, glucose-6 phosphate dehydrogenase (G6PD) evaluation prior to starting the drug is important and treatment should be avoided in those with a G6PD deficiency. Levels of G6PD, ALT, and AST should be followed during dapsone treatment and the patient should additionally be monitored for hemolysis and leukopenia. 2-4,7 The use of oral steroids, such as prednisone, to prevent systemic inflammation has been recommended, although there is disagreement over the benefit of steroid treatment.2,9 Aspirin can be used to inhibit platelet aggregation and reduce the risk of thrombosis and possibly DIC. A tetanus shot may be given prophylactically and antibiotics may be given to prevent secondary wound infections.3,7,9 Additionally, antihistamines, such as Benadryl (diphenhydramine), have been shown in some cases to be more effective than surgical wound care in stimulating wound healing.14 Conclusion Most brown recluse spider bites heal without medical input or laboratory testing. Some bites, however, result in systemic symptoms that require prompt treatment. The development of an ELISA for Loxosceles venom may aid in the diagnosis of brown recluse spider bites. Until such confirmatory testing can be established, it is important www.labmedicine.com 3-Review_Amjad.indd 303 Downloaded from http://labmed.oxfordjournals.org/ by guest on October 13, 2016 To read this article online, scan the QR code, http://labmed. ascpjournals.org/content/44/4/300. full.pdf+html References 1. Fishman TD. Wound assessment and evaluation. Brown recluse spider bite. DermatolNurs. 1999;11:290-291. 2. Rhoads J. Epidemiology of the brown recluse spider bite. J Am Acad Nurse Pract. 2007;19:79-85. 3. Sams HH, King LE Jr. Brown recluse spider bites. Dermatol Nurs. 1999;11:427-433. 4. Swanson DL, Vetter RS. Bites of brown recluse spiders and suspected necrotic arachnidism. N Engl J Med. 2005;352:700-707. 5. Sandidge JS. Arachnology: Scavenging by brown recluse spiders. Nature. 2003;426:30. 6. Parekh KP , Seger D. Systemic loxoscelism. Clin Toxicol (Phila). 2009;47:837. 7. Wasserman G, Lowry J, Algren DA. Systemic loxoscelism—not so quick! ClinToxicol (Phila). 2009;47:837. 8. Gomez HF, Krywko DM, Stoecker WV. A new assay for the detection of Loxosceles species (brown recluse) spider venom. Ann Emerg Med. 2002;39:469-474. 9. Lung JM, Mallory SB. A child with spider bite and glomerulonephritis: a diagnostic challenge. Int J Dermatol. 2000;39:287-289. 10. Hubbard JJ, James LP. Complications and outcomes of brown recluse spider bites in children. Clin Pediatr (Phila). 2011;50:252-258. 11. Tavares FL, Peichoto ME, Rangel DdeM, et al. Loxosceles gaucho spider venom and its sphingomyelinase fraction trigger the main functions of human and rabbit platelets. Hum ExpToxicol. 2011;30:1567-1574. 12. Blackall DP. Transfusion medicine illustrated: Intravascular hemolysis with brown recluse spider envenomation. Transfusion. 2004;44:1543. 13. Lane L, McCoppin HH, Dyer J. Acute generalized exanthematous pustulosis and Coombs-positive hemolytic anemia in a child following Loxosceles reculsa envenomation. Pediatr Dermatol. 2011;28:685-688. 14. Carlton PK Jr. Brown recluse spider bite? Consider this uniquely conservative treatment. J Fam Pract. 2009;58:E1-E6. Fall 2013 | Volume 44, Number 4 Lab Medicine 303 10/7/13 5:12 PM