Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
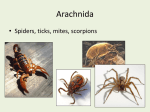
“I think something bit me.” Gretchen Shaughnessy, MD Clinical Fellow Dept of Infectious Diseases 4/16/08 CC: Arm pain 27 yo CM remote history of substance abuse presented to OSH with R arm swelling. 6 days PTA he had been helping his brother move a woodpile. After he carried the logs from one side of the yard to the other he noticed a sore spot on the inside of his right elbow. He had seen spiders on the logs and recently killed some brown spiders in his house, so concluded he had been bit by a spider. The sore spot became more swollen and red over the next few days. The area became more firm and tender then started to darken in color. HPI (cont) One day PTA the patient was seen at his primary care physician’s office for severe pain and swelling. He was prescribed levofloxacin and instructed to go to the ED if his symptoms got worse. The patient went home from the doctor’s office planning to refill the prescription in the morning. That night at midnight he presented to his local ED for severe pain and redness in his arm. He states his arm was “so swollen it felt like it was gonna pop open.” It was “so dark it looked like a hunk of meat.” He said the wound “smelled like rotting meat.” HPI (cont) The ER MD called a surgical consult to assess for necrotizing fasciitis. The surgeons Recommended transfer to UNC. Called the UNC ID fellow and requested a transfer. Per physician – redness was previously all below the elbow, since the patient had been in the ED (3 hours) it had extended superiorly towards his bicep. HPI (cont) The patient was started on imipenum, clindamycin, and vancomycin and transported to UNC. From departure of OSH to arrival at UNC ED the patient reports the redness has decreased. Prior marker line approximately 2cm from current errythematous border PMH Face and head trauma (2000) - the patient had been battered, experienced multiple facial lacerations but no LOC. h/o Anxiety and depression previously treated with lexapro Medications Prior to hospitalization - None Allergies - NKDA History (cont) Social History: tob 2 pacs a day for 10 years ETOH 2 drinks /week h/o cocaine, XTC, mj use in the distant past. The patient adamantly denies using any IV drugs recently, denies any HIV risk factors. His last HIV test was 2 years ago and was negative. No pets Lives near Fayetteville, NC Family History: DM - uncles. HTN - father Physical Exam 154/89 - 76 - 15 - 36.2 INAD, resting comfortably. EOMI, PERRLA, nonicteric no e/e on OP. no JVDLymph Nodes no LAD appreciated in cervical, supraclavicular, or inguinal regions RRR no murmurs CTAB no rash or lesions other than RUE a&ox3, pleasant and cooperative soft NT nabs, no HSM LUE and BLE have no c/c/e RUE with approx 2cm area of dark discoloration, exquisite tenderness, and purulent drainage on the medial aspect of the R anticubital fossa. there is surrounding edema, minimal induration. The errythema is approximately 5cm receeded from the marker line labelled 4/11/04 0445am. Neurological no focal defecits, sensation intact Radiology Radiology CT with contrast CT with contrast CT with contrast CT with contrast CT with contrast CT with contrast CT with contrast CT with contrast CT without contrast CT without contrast CT without contrast CT without contrast CT without contrast CT without contrast CT without contrast Discussion Further Diagnostic Tests Operative Report a small cavity in the subcutaneous area of the antecubital fossa that did involve the defect into the fascia, but there was no deep collection of pus, dead muscle or deeper involvement. There was a small amount of necrotic skin and subcutaneous tissue, all of which was debrided away. Hospital Course Diagnosed with streptococcus anginosus cellulitis with fascial defect s/p debriedment Did well clinically, no further fevers, WBC remained normal. 4 days of IV therapy then d/ced on amoxicillin/clavulanate to follow up with ortho and ID DDx of blackened eschar lesion Cutaneous anthrax lesions Brown recluse spider bite Rickettsial pox Cutaneous leishmaniasis Varicella zoster Herpes simplex Staphylococcal or streptococcal cellulitis Ecthyma gangrenosum Ulceroglandular tularemia Plague Eczema Typhus Glanders Rat-bite fever Aspergillosis Mucormycosis Leprosy Vaccinia Spider Bite? Brown Recluse is often blamed for necrotic lesions In North Carolina this is fairly unlikely Literature looking at the falsely high incidence of “spider bites” Brown Recluse photo: R. Bessin, University of Kentucky Entomology. Distribution map from R. Vetter, Univ. Calif. Riverside Spider Survey Vetter et al. survey of a Kansas home using glue boards Found 2055 confirmed Loxosceles reclusa from June-Nov 2001 No bites to family of four living in the home during that time Brown Recluse Bite vs Bacterial Infection Images from University of Kentucky Dept of Entomology. References Uptodate.com 4/15/08 Mandell’s Principles and Practices of Infectious Disease, 5th Ed. Majeski, J. Necrotizing fasciitis developing from a brown recluse spider bite. Am Surg 2001; 67:188. Wright, SW, Wrenn, KD, Murray, L, et al. Clinical presentation and outcome of brown recluse spider bites. Ann Emerg Med 1997; 30:28. Anderson, PC. Spider bites in the United States. Dermatol Clin 1997; 15:307. Williams, ST, Khare, VK, Johnson, GA, et al. Severe intravascular hemolysis associated with brown recluse spider envenomation: A report of two cases and review of the literature. Am J Clin Pathol 1995; 104:463. Vetter, R. Identifying and misidentifying the brown recluse spider. Dermatol Online J 1999; 5:7. Vetter RS, Barger DK. An infestation of 2,055 brown recluse spiders (Araneae: Sicariidae) and no envenomations in a Kansas home: implications for bite diagnoses in non-endemic areas. J Med Entomol 2002; 39:948-951. Vetter RS, Cushing PE, Crawford RL, Royce LA. Diagnoses of brown recluse spider bites (loxoscelism) greatly outnumber actual verifications of the spider in four western American states. Toxicon 2003; 42:413-418.