Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
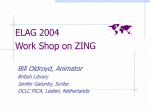
Pica Patricia Frese, RDH, MEd Continuing Education Units: 1 hour Online Course: www.dentalcare.com/en-US/dental-education/continuing-education/ce465/ce465.aspx Disclaimer: Participants must always be aware of the hazards of using limited knowledge in integrating new techniques or procedures into their practice. Only sound evidence-based dentistry should be used in patient therapy. The goal of this course is to provide the dental team with the skills and knowledge to recognize the symptoms of pica and appropriately manage the dental needs of patients who exhibit pica. Conflict of Interest Disclosure Statement • Ms. Frese has done consulting work for P&G. ADA CERP The Procter & Gamble Company is an ADA CERP Recognized Provider. ADA CERP is a service of the American Dental Association to assist dental professionals in identifying quality providers of continuing dental education. ADA CERP does not approve or endorse individual courses or instructors, nor does it imply acceptance of credit hours by boards of dentistry. Concerns or complaints about a CE provider may be directed to the provider or to ADA CERP at: http://www.ada.org/cerp 1 Crest® Oral-B® at dentalcare.com Continuing Education Course, November 2, 2015 Approved PACE Program Provider The Procter & Gamble Company is designated as an Approved PACE Program Provider by the Academy of General Dentistry. The formal continuing education programs of this program provider are accepted by AGD for Fellowship, Mastership, and Membership Maintenance Credit. Approval does not imply acceptance by a state or provincial board of dentistry or AGD endorsement. The current term of approval extends from 8/1/2013 to 7/31/2017. Provider ID# 211886 Overview This course is an introduction to the eating disorder pica. This eating disorder has been recognized for centuries and is still an occasional problem today. The course will explore the history, prevalence and etiology of pica. The various pica substances consumed, diagnosis, and complications will also be covered. Management techniques for the dental team and treatment options for patients with pica will be presented. Learning Objectives Upon completion of this course, the dental professional should be able to: • Define pica. • List three possible causes of pica. • Recognize intraoral signs of pica. • Describe how to educate patients on the dental health risks of pica. • Describe appropriate dental management techniques for patients with pica. • Describe appropriate medical and dental treatment options for patients with pica. • Identify additional resources for patients and dental professionals. Course Contents • • • • • • • • • • • • • Introduction Brief History Prevalence Etiology and Conditions Associated with Pica Substances Consumed Diagnosis Complications Dental Concerns and Management Treatment Conclusion Course Test References About the Author Pica is the most common eating disorder in individuals with developmental disabilities.6 In some societies, pica is a culturally sanctioned practice and is not considered pathologic. The consequences of pica can be benign or lifethreatening.6 Introduction Pica is included in a broad category of eating disorders. Pica is defined as a pattern of consuming nonfood materials, such as soil, clay and hair, for a period of at least one month. This ingestion of materials is inappropriate to the developmental level of the individual. Therefore, it does not include the exploration or accidental ingestion of nonnutritive substances by children under the age of 2. Occasionally, the definition is broadened to include the mouthing of nonnutritive substances.6 According to The Diagnostic and Statistical Manual of Mental Disorders: Fifth Edition (DSM-5),5 to be diagnosed with pica a person must display: • Persistent eating of nonnutritive substances for a period of at least one month. • The eating of nonnutritive substances is 2 Crest® Oral-B® at dentalcare.com Continuing Education Course, November 2, 2015 inappropriate to the developmental level of the individual. • The eating behavior is not part of a culturally supported or socially normative practice. • If occurring in the presence of another mental disorder (e.g., autistic spectrum disorder) or during a medical condition (e.g., pregnancy), it is severe enough to warrant independent clinical attention. of “normal foodstuffs” has cultural implications.16 In addition, those who practice pica may be hesitant to divulge such a practice. All these factors combine to make precise statistics on the prevalence of pica very challenging. Pica has been practiced by a wide variety of populations4,11,13,15 including: • Individuals with autism and other developmental disabilities • Pregnant women •Children • Individuals from developing countries • Women born outside the United States • African-American women • Individuals of lower socioeconomic status • Those with a family history of pica Note: Pica often occurs with other mental health disorders associated with impaired functioning. Brief History The term pica comes from the Latin word for magpie. Magpies show a propensity to eat almost anything, including nonfood items.13 The Eurasian Magpie is Pica pica. It is estimated that pica affects:4 • 10-30% of children 1-6 years old • 20% of dialysis patients • 20% of pregnant women Pica has been known throughout the ages, dating back to 1800 BC in Sumeria, Egypt and China.14 Clay eating for medicinal purposes dates back to 10 BC.10 The eating of dirt and clay was known to the Greeks and Romans and was recorded in a 13th century Latin work.13 The first medical text reference to pica occurred in 1563 with an entry on geophagia (eating earth or soil-like substrates such as clay or chalk) in pregnant women and children.12 Etiology and Conditions Associated with Pica The exact etiology of pica remains unknown despite the fact that pica has been reported since antiquity. Pica is considered a multifactorial phenomenon because of this potential for multiple etiologies.1,4 Several theoretical approaches attempt to explain pica from nutritional, sensory, neuropsychiatric, ethnic, or psychosocial perspectives.4,6,13 Pica still occurs in some modern cultures as a ritualistic practice. Geophagia was a common practice in the southern Unites States during the 1800s. It has been practiced as part of religious ceremonies, magical beliefs and attempts at healing.12 During the 1950s and 1960s, geophagia was so common in the south that one could purchase small bags of clay at bus stops. In addition, as northern migration occurred, bags of special local clay were mailed by southern family members to northern relatives who still craved the clay.13 Currently, white clay can be purchased in southern grocery stores as well as online.2 The most common nutritional theories attribute pica to deficiencies of specific minerals including iron and zinc. Several case studies describe patients with low iron or zinc levels whose pica behavior diminishes with iron or zinc supplementation.4 Clay, especially red clay from the southern United States, is high in iron and may prompt pica behavior in an attempt to supplement Prevalence Pica has been described in the literature as “underreported” and “unrecognized.”6 There have been few epidemiologic studies detailing the prevalence of pica.13 There is disagreement as to the precise definition of pica. For instance, the use of the terms nonnutritive and normal foodstuffs have limitations. Cornstarch provides calories and soils may provide micronutrients. The definition 3 Crest® Oral-B® at dentalcare.com Continuing Education Course, November 2, 2015 for this micronutrient.16 However, clay eating may be the cause of iron deficiency anemia, as clay is an iron chelator and binds iron, reducing its bioavailability. A less common theory postulates that people eat nonfood substances because they do not have anything else to eat.16 are used to treat nausea, diarrhea and vomiting.16 Clay is also consumed to coat the stomach and intestines before eating foods such as fish that may contain toxins or pathogens.4,16 This coating could slow the absorption of these toxins and pathogens.16 It is understandable that children could mimic the pica behavior of those around them as a practice as well as a method of relieving intestinal distress.4 Sensory theories focus on the reports that patients say they enjoy the taste, texture or smell of the item they are consuming.13 The “crunch” of cornstarch or clay, the “chew” of rubber bands or the smell of foam rubber are described as pleasing to the consumer. Psychosocial theories of the etiology of pica suggest an association with family stress (abuse, parental separation, neglect or poor parenting), a smaller social support network and as a display of aggression.4,13 A neuropsychiatric component is supported by evidence in laboratory animals with certain brain lesions and abnormal eating behaviors in these animals. Therefore, pica may be associated with certain brain disorders in humans.13 Recent evidence indicates that pica may be part of the obsessive-compulsive disorder (OCD) spectrum of diseases. There are case reports from five patients undergoing OCD treatment who indicate their pica behavior is a ritualistic behavior they are compelled to carry out and that eating the substance lessens the anxiety or tension they experienced.13 Traditional OCD therapy, which is primarily psychotherapy, had a variable effect on the pica behavior in these patients. These case reports lend support to the theory that, at least in some patients, pica may be a manifestation of OCD.13 Pica has comorbid associations with other diseases and disorders including autism, autism spectrum disorders (ASD), psychosis, and developmental disabilities.2,7,11,13 Neurochemical and neuropathological changes that occur in patients with dementia may also contribute to a change in eating habits resulting in pica behavior.4 Substances Consumed Substances may be labeled or identified as objects of pica. Certain groups may show a preference for a substance as part of their pica behavior. It is interesting to note that the range of items reported has changed little over 4 centuries. Table 1 presents a selection of information on the more common items consumed.1,2,6,10,13,16 Diagnosis There are no definitive laboratory tests to provide a diagnosis of pica. Instead pica is a clinical diagnosis, confirmed by the patient’s history.11 Suspicions about the presence of pica behavior should be investigated. Health care providers should ask the patient (or parent or caregiver, as appropriate) about pica behavior or unusual cravings, especially in high risk groups. Some patients may self-report the pica behavior. However, patients are likely to underreport because of embarrassment or because they are not aware the behavior could be problematic.13 An evaluation of symptoms may be the best approach. If a patient has anemia, lead poisoning or intestinal obstruction, the health care provider should investigate pica as a cause. Certain laboratory tests can be performed to confirm the symptoms, but the cause of the pica behavior must be admitted by the patient. Parents may be counseled to observe children for signs of pica behavior. Pica is a widespread practice in India and has been reported in Australia, Canada, Israel, Iran, Uganda, Wales and Jamaica.6 Pica is culturally acceptable among families of African heritage and is reported to be problematic in 70% of provinces in Turkey. In Guatemala, clay is molded into small religious icons, called panito del senor, and consumed. Pica has been associated with fertility rites; the eating of soil is thought to ensure future offspring. Clay and starch have been eaten by pregnant women to ease morning sickness.4 Some clay contains kaolin, formerly the active ingredient in Maalox® and Kaopectate. These over-the-counter products Complications Complications of pica are generally classified into five groups.4,13 First is inherent toxicity where there are direct toxic effects from the consumption of lead, mercury, arsenic or other 4 Crest® Oral-B® at dentalcare.com Continuing Education Course, November 2, 2015 Table 1. Common Items Consumed. 5 Crest® Oral-B® at dentalcare.com Continuing Education Course, November 2, 2015 is a symptom of anemia, and the patient should be questioned about ice or freezer frost consumption. Ingestion of cigarette butts poses multiple risks, such as gingival recession, periodontal disease and oral cancer.4,6 Pica behavior occasionally manifests as overconsumption of food items. If lemons or candy are consumed in this manner, enamel erosion and tooth decay can result. In addition, caution is necessary if the patient or health care provider substitutes sugar containing foods for the pica substance. All dental patients should have a thorough medical history taken and reviewed. A complete oral exam should be performed. Any unusual findings should be investigated. Patients with autism, pregnant women, and children with developmental disorders are at higher risk for pica. Any suspicions should be investigated further and patients (or their parents or caregivers, as appropriate) should be directly questioned about pica behavior. If nutritional deficiencies are suspected, a consultation with the patient’s physician is warranted.1,4 heavy metals. An example is eating paint chips from lead paint or soil surrounding a house painted with lead-based paint. In a child, this can cause irreversible neurological damage. In an adult, it can cause behavior changes. Another example is consumption of clay which could lead to hypokalemia. Potassium is a critical electrolyte, necessary for proper nerve and muscle cell function, especially in the heart. Second is the risk of obstruction or aspiration. Bezoars, indigestible masses that lodge in the digestive tract, may form. A trichobezoar forms as a result of hair eating. Consumption of other objects, such as metal, can block the trachea, esophagus or intestines. Subsequent perforation, peritonitis and death can result. Third is excessive caloric intake, typically seen in amylophagia (starch eating). Fourth is general nutritional deprivation. Nonnutritive items like dirt, gravel, wood or ice are eaten in place of a variety of nutritive foods. Young children may exhibit a failure to thrive and adults may appear anorexic. Fifth is other complications such as parasitic infections or dental injury. If contaminated feces or dirt are consumed, toxoplasmosis (infection from a parasite found in cat feces) or toxocariasis (infection from a roundworm found in dog and cat feces) may result. While healthy adults may not develop symptoms, children, immunocompromised individuals and pregnant women are at greater risk for developing a severe infection.13 Treatment Treatment of pica should take multiple approaches as no one treatment is universally effective. The first concern would be the treatment of medical problems such as obstruction, infection or heavy metal poisoning.13,15 Nutritional counseling might be the first wave of intervention.13 Education about proper nutrition and elimination of consumption of nonfood items as well as iron or zinc supplementation may be effective. Patients can be encouraged to substitute better food choices for the craved substance: sugar-free candies for pebbles, powered milk for starch or sugar-free ice pops for ice or freezer frost. Psychological approaches could include counseling and behavior therapy. Interventions such as positive reinforcement for eating from a plate have been effective in children with developmental disabilities. Mild aversion therapy, where unpleasant consequences or punishment followed by positive reinforcement for eating the correct foods, has been successful.13 A combination of positive reinforcement and response reduction, blocking or obstructing the patient’s attempt to consume the pica substance, have shown good efficacy.11 The identification of stressors followed by stress reduction therapy is warranted, Dental Concerns and Management The mouthing or chewing of pebbles or grit can cause wear to both the natural dentition and restorations. Chewing of hard objects like metal or ice can cause tooth or restoration fracture. Sharp objects like glass or wood splinters can cause lacerations or other trauma. Atrophy of the tongue 6 Crest® Oral-B® at dentalcare.com Continuing Education Course, November 2, 2015 especially in children where family-based stress may play a role.13 In certain cases, pharmacological intervention may be necessary. Selective serotonin reuptake inhibitors, prescribed for patients with anxiety, depression or other mental disorders; atypical neuroleptics (olanzapine) and attentiondeficit/hyperactivity disorder medications (methylphenidate) have been used, with varying levels of success.8,11,13,15 Not all pica substances are dangerous and intervention might not be necessary in some cases.13 For instance, if the pica substance being consumed is small quantities of cornstarch and no medical or dental issues are present, there may be no benefit to counselling the patient to stop consuming the cornstarch. The patient should be educated about consuming excessive amounts of cornstarch due to additional empty calories. in childhood and the patient enters teen or adult age.13,15 Prevention strategies may be important as well. Pica is most often practiced when the patient is alone or unsupervised.8 Increased supervision, especially in children and patients with developmental disabilities, can prevent or lessen the behavior. Knowing about and getting proper nutrition may be helpful.15 Removing or reducing access to the source of the pica substance (removing lead-based paint chips or monitoring children playing in sand boxes) is important.13 Stool checks may be used with institutionalized patients.8 Conclusion Having the knowledge and skills to recognize the oral implications of pica, educate the patient or patient’s family about the concerns and provide appropriate referral is important to provide quality care to dental patients. Pica can last for a number of years then resolve on its own; especially when the behavior is seen 7 Crest® Oral-B® at dentalcare.com Continuing Education Course, November 2, 2015 Course Test Preview To receive Continuing Education credit for this course, you must complete the online test. Please go to: www.dentalcare.com/en-US/dental-education/continuing-education/ce465/ce465-test.aspx 1. Pica is defined as the consumption of nonfood materials for a period of at least one year. a.True b.False 2. Pica can be diagnosed in children as young as 18 months. a.True b.False 3. Some definitions of pica include mouthing of objects. a.True b.False 4. Pica is the most common eating disorder in individuals with developmental disorders. a.True b.False 5. Pica is not considered pathologic as it is a culturally sanctioned practice in some countries. a.True b.False 6. Consequences of pica behavior can be both benign or life-threatening. a.True b.False 7. Pica can affect: a.Children b. Pregnant women c. Patients on dialysis d. All of the above 8. Pica may be caused by: a. Iron deficiency b. Cultural practices c. Psychosocial issues d. All of the above 9. Geophagia is the most common type of pica. a.True b.False 10. Amylophagia is the second most common type of pica. a.True b.False 11. There is an association with patients who consume glue and patients who have sickle cell disease. a.True b.False 8 Crest® Oral-B® at dentalcare.com Continuing Education Course, November 2, 2015 12. Complications of pica can include: a.Malnutrition b. Intestinal distress c.Obstruction/aspiration d. All of the above 13. Intraoral signs of pica can include: a. Tooth wear b.Erosion c. Oral cancer d. All of the above 14. If pregnant women show intraoral signs of pica, the dental health care professional should directly question the patient about pica behavior. a.True b.False 15. Treatment of pica may include: a. Behavior therapy b. Pharmacological intervention c. Nutritional counseling d. All of the above 9 Crest® Oral-B® at dentalcare.com Continuing Education Course, November 2, 2015 References 1. Barker D. Tooth wear as a result of pica. Br Dent J. 2005 Sep 10;199(5):271-3. 2. Blinder BJ. An update on pica: prevalence, contributing causes, and treatment. Psychriatric Times. 2008 May;25(6). Accessed October 19, 2015. 3. Chakraborty S, Sanyal D, Bhattacharyya R. A unique case of pica of adult onset with interesting psychosexual aspects. Indian J Psychol Med. 2011 Jan;33(1):89-91. 4. Cooper MD. Pica. Access. 2010 May-June;24:39. Accessed October 19, 2015. 5. Diagnostic and statistical manual of mental disorders: DSM-5. Arlington, Va: American Psychiatric Press, 2013. 6. Ellis CR, Schnoes, CJ, Pataki C, et al. Medscape. Practice Essentials. Pica: Practice Essentials. Updated September 23, 2014. Accessed October 19, 2015. 7. Hergüner S, Ozyildirim I, Tanidir C. Is Pica an eating disorder or an obsessive-compulsive spectrum disorder? Prog Neuropsychopharmacol Biol Psychiatry. 2008 Dec 12;32(8):2010-1. 8. Khan Y, Tisman G. Pica in iron deficiency: a case series. J Med Case Rep. 2010 Mar 12;4:86. 9. Klein A, Schröder C, Heinemann A, et al. Homicide or suicide? Xylophagia: a possible explanation for extraordinary autopsy findings. Forensic Sci Med Pathol. 2014 Sep;10(3):437-42. 10. Lacey EP. Broadening the perspective of pica: literature review. Public Health Rep. 1990 Jan-Feb; 105(1):29-35. 11. Mishori R, McHale C. Pica: an age-old eating disorder that’s often missed. J Fam Pract. 2014 Jul; 63(7):E1-4. 12. Parry-Jones B, Parry-Jones WL. Pica: symptom or eating disorder? A historical assessment. Br J Psychiatry. 1992 Mar;160:341-54. 13. Rose EA, Porcerelli JH, Neale AV. Pica: common but commonly missed. J Am Board Fam Pract. 2000 Sep-Oct;13(5):353-8. 14. Stokes T. The earth-eaters. Nature. 2006 Nov 30;444(7119):543-4. 15. U.S. National Library of Medicine. MedlinePlus. Pica. Updated 2/14. Accessed October 19, 2015. 16. Young SL, Wilson MJ, Miller D, et al. Toward a Comprehensive Approach to the Collection and Analysis of Pica Substances, with Emphasis on Geophagic Materials. PLoS ONE 2008 3(9):e3147. Accessed October 19, 2015. Additional Resources For Patients and Parents •KidsHealth • Psychology Today • Autism Speaks • American Pregnancy Association • eatright PRO For Dental Professionals • NIH U.S. National Library of Medicine • American Dental Hygienists’ Association • Psychology Today Selected Case Reports of Pica • Man swallows 227 metal objects including kitchen forks, coins and a screwdriver. • In the Glore Psychiatric Museum, St. Joseph, Missouri, there is an arrangement of 1,446 items swallowed by a patient and removed from her intestines and stomach. She died during surgery from bleeding caused by 453 nails, 42 screws, safety pins, spoon tops, and salt and pepper shaker tops. • Case reports of ice cube eating and rubber band chewing. • Case report of young girl consuming brick pieces. 10 Crest® Oral-B® at dentalcare.com Continuing Education Course, November 2, 2015 About the Author Patricia Frese, RDH, MEd Patricia Frese is Professor of Dental Hygiene at the University of Cincinnati Blue Ash College Cincinnati, Ohio. She has been in education since 1980. She is a 1976 graduate of the dental hygiene program at Raymond Walters College (now UC Blue Ash). She has private practice experience in general, research and periodontal practice settings. She has presented on a variety of topics at professional meetings. Pat is an active member of the American Dental Hygienists’ Association. Email: [email protected] 11 Crest® Oral-B® at dentalcare.com Continuing Education Course, November 2, 2015