Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
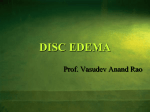
July 2015 OWL Award for Woman Leadership The Not-So-Skinny on Papilledema During the recent ASCRS meeting, Northwest Eye Surgeons’ own Audrey Talley Rostov was recognized with the Visionary Woman Award. The award, presented by the Ophthalmic Women Leaders (OWL) organization, honors an ophthalmic professional who has paved the way for other women in the field through her achievements. By Landon Jones, OD The achievements, qualifying Dr. Rostov for the award, include her service on the medical advisory board of Sightlife, her surgical instruction of femtosecond laser keratoplasty technique to surgical staff in New Delhi, India, and her work with the Himalayan Cataract Project, to create a cornea fellowship for Ethiopian surgeons. More information about the DSEK technique that Dr. Rostov taught to other surgeons can be found on our website: www.nweyes.com. While acquired optic nerve edema occurs infrequently, the cases that do present can be challenging. Misdiagnoses or suspicion of papilledema are often referred in by general practitioners or emergency room physicians. These patients rightfully present with anxieties attached to the diagnosis. This article acts as a terse overview for the condition of papilledema and its differentials. Papilledema Defined Disc edema is a general, non-specific term referring to a multitude of potential disease etiologies. In Left optic nerve of a 13 year old boy who presented with addition to papilledema, papilledema. Photo courtesy of Merge.com disc edema includes conditions such as optic neuritis, optic neuropathy, and diabetic papillopathy, among others. Optic nerve papilledema refers specifically to swelling of the optic nerve as a result of elevated intracranial pressure. This term can be considered as a clinical finding. Pseudotumor cerebri, a synonym to Idiopathic Intracranial Hypertension, is the true diagnosis or cause of the papilledema when spaceoccupying lesions have been ruled-out. It is deemed a diagnosis of exclusion. The most common space-occupying lesions which can rule-out papilledema include intracranial tumors, subarachnoid hemorrhage, and subdermal hematomas. It is important to rule out benign causes of optic disc elevation when examining patients that are suspect for papilledema. Optic disc drusen and anatomically crowded optic nerves are both forms of pseudopapilledema that can fool the practitioner into believing that the nerve is edematous. B-scan and OCT of the peripapillary area can both be utilized to help make this diagnosis more definitively. Incidence and Demographics Audrey Talley Rostov, MD, with NWES CEO Maureen Tipp and Business Operations Manager, Susan Oliveto, at 2015 ASCRS meeting in San Diego. It is widely accepted that a higher incidence of pseudotumor is linked to a higher incidence of obesity across the globe. The most likely demographic is obese women during childbearing years. These facts, along with weight gain contributing to higher recurrence rates, supports obesity as one of the most likely theorized etiologies. Many studies consider it more of a strong chance Continued on page 4 “Life Is Good” Photo courtesy of C. Freeman A Patient Recounts Cataract Surgery with Vision Correction I was living with creeping glaucoma and cataracts, unaware of how bad it was getting, when my local eye guy said something needed to be done, and recommended Northwest Eye Surgeons. They fixed my right eye in December, and a month later, my left. After the right eye [surgery], white was white, red was red, and edges were sharp. When I closed my right eye and looked out of my unfixed left eye, it was a blurred view through a nicotine stained window, which proved to me that you won’t know how bad it was until someone makes it better. I can’t praise NWES enough. They were kind, humorous, polite and timely. Better yet, they told me what to expect, what they were going to do and then did it. They were what I always expect and seldom get. Now, when I look at a mountain top, I see a mountain top. Life is good. -NWES patient Charlie Freeman Education Highlights: Tried and Tested Along With a New Offering! On April 29th, we were pleased to present the 5th annual MultiDisciplinary Spring Symposium at the Lynnwood Convention Center. This year’s four-hour CE covered the broad topic of Oncology. Northwest Eye Surgeons staff presenters included Dr. Michael Giese, providing an update on ocular side effects of cancer treatments, Dr. Tom Osgood, discussing external lesions and Drs. Paul Griggs and Richard Lee covering retinal oncology. Guest expert Nancy Thompson, RN, AOCNS, rounded out the program with prevention updates and a high-level outline of the issues impacting patients who are undergoing or recovering from cancer treatment, or receiving palliative care. Guest speaker and neurosurgeon, Johnny Delashaw, MD, closed the program, providing an anatomy review and detailing surgical interventions for removing lesions of the visual pathway. Mingled with our education was a delicious dinner and time for the 245 ODs in attendance to mingle and share personal and professional updates with each other. We are committed to continuing this popular program. We offered our First Annual Resident Grand Rounds at the Shoreline Conference Center on Wednesday, May 27th. Attendees enjoyed a catered dinner while five Washington-located optometric residents presented cases from their training, covering topics including Papilledema and Central Serous Retinopathy. We are excited to make this an annual event and to see more of you there next year. Keep up to date on future education offerings on our website: www.nweyes.com. Practice Update Femtosecond Laser Adds to Vision Correction Armamentarium By Tom Osgood, MD In addition to making precise incisions for the paracentesis, corneal tunnel, capsulorhexis and phacofragmentation, the femtosecond laser also makes perfect limbal relaxing incisions (LRIs). The precision that femtosecond laser technology adds to our ability to treat astigmatism is demonstrated in the following case. Case: Mr. W. is a skeptical seventy-nine year old retired Boeing engineer. His pre-op MR and K’s are shown below. Manifest Refraction: K’s OD: -0.50 + 1.00 x 174 OD: 44.66/45.52 x 170 OS: -1.25 + 1.25 x 113 OS: 43.75/46.03 x 102 I was not able to convince Mr. W. that without treating his astigmatism he would end up with more astigmatism than he had preoperatively, because removing the lens would allow the full corneal astigmatism to manifest. Fortunately, I was able to offer LRI. Mr. W. desired to have good uncorrected near vision at 20 to 22 inches. Therefore, I targeted -1.75 D. During his left cataract surgery the femtosecond laser was programmed to make paired 42 degree arcs, at a radius of 9.2 mm, centered on the steep corneal axis of 102-282 degrees. The laser cut beautiful, perfect arcs at 80 percent of corneal depth. Postoperatively, in the left eye, Mr. W. could see J1 without correction and 20/40 at a distance, without correction, but he wanted even better near vision for his right eye. I then targeted his right eye for -2.25 D and performed a similar surgery with femtosecond laser LRIs. Mr. W. is now extremely happy with his uncorrected near vision. Even his uncorrected distance vision is good enough at 20/40 that he does not wear glasses. His post-op MR and acuities are: SC OD: 20/100 (-2.50 sph) 20/20 J1+ SC OS: 20/40 (-1.50 + 0.25 x 90) 20/25 J1 This case points to the precision of the femtosecond laser in making perfect LRI incisions, rivaling that of LASIK. With Vision Correction, one advantage of femtosecond laser LRIs is that they can be used in combination with Toric IOLs to treat high degrees of astigmatism. Femtosecond laser LRI’s can even be titrated for more effect, either during surgery in conjunction with ORA (intraoperative aberrometry), or later in the post-op period, by gently “opening” the LRI to give more effect. In Mr. W’s case this was not needed, but is an option that can be added to our Vision Correction armamentarium. Femtosecond Laser with Vision Correction is available now in our Mount Vernon and Seattle clinics. Our physicians would be glad to talk with you further about incorporating femtosecond laser into your patient’s cataract surgery planning. For more information reach us at 800-826-4631. 10330 Meridian Ave. N. Suite 370 Seattle, WA 98133 Medical Article: Papilledema, continued from page 1 CONTINUING EDUCATION SEPTEMBER 17 | THURSDAY OCT Analysis of Nerve and Macula Drs. Meng Lu and Richard Lee Renton Dinner 6:00 p.m. Program 6:30 p.m. SEPTEMBER 22 | TUESDAY OCT Analysis of Nerve and Macula Drs. Meng Lu and Richard Lee Seattle Dinner 6:00 p.m. Program 6:30 p.m. Please send us your thoughts about our continuing education efforts: Reach us at 800-826-4631, or [email protected]. Thank you for sharing your comments. association since the hypothesis fails to explain the presence of pseudotumor in obesity’s absence. Two other popular theories of etiology target stenosis of the transverse cerebral sinuses and pathogenesis based on levels of vitamin A in the cerebrospinal fluid. Signs and Symptoms Patients present to the office most commonly with a diffuse and non-specific headache. Transient vision loss, peripheral visual disturbances, and pulsatile tinnitus are often reported. Horizontal diplopia due to compression of the sixth nerve could be a presenting factor as well. Optic disc edema is the hallmark sign of pseudotumor cerebri. The papilledema is most often bilateral but can have asymmetrical presentation. Disc hemorrhages, obscuration of retinal vascularization leaving the optic nerve, and striae of the peripapillary retina can be present in more severe cases. While an enlarged blind spot on perimetry can be an early finding, if left untreated, papilledema can lead to optic atrophy and permanent field loss. Diagnosis and Treatment Official diagnosis of pseudotumor is often made via referral to a neurologist. An MRI is ordered to rule-out space-occupying lesions to start. If no cause for the suspected elevation of intracranial pressure is discovered, then lumbar puncture is subsequently ordered to confirm the diagnosis. General treatment of pseudotumor involves lowering the intracranial pressure to alleviate symptoms and to prevent potential vision loss. This is often done medically through use of oral carbonic anhydrase inhibitors. Weight loss of about 5-10% has been found to improve signs and symptoms and to reduce risk of recurrence. Optic nerve sheath fenestration and cerebrospinal fluid shunting are the most commonly used surgical procedures if systemic medications do not achieve a desired therapeutic effect. References: Whiting AS, Johnson LN. Papilledema: clinical clues and differential diagnosis. Am Fam Physician. 1992 Mar;45(3):1125-34. Yri HM, Wegener M, Sander B, Jensen R. Idiopathic intracranial hypertension is not benign: a longterm outcome study. J Neurol. 2012 May;259(5):886-94.