Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
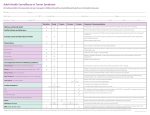
European Journal of Neurology 2012, 19: 800–811 doi:10.1111/j.1468-1331.2011.03627.x CME ARTICLE Susac syndrome: clinical characteristics and treatment in 29 new cases F. J. Mateena,b, A. Y. Zubkovc, R. Muralidharana, J. E. Fugatea, F. J. Rodriguezd, J. L. Winterse and G. W. Pettya a Department of Neurology, Mayo Clinic, Rochester, MN; bDepartment of Neurology, Johns Hopkins Hospital, Baltimore, MD; cMinneapolis Clinic of Neurology, Edina, MN; dDivision of Neuropathology, Department of Pathology, Johns Hopkins Hospital, Baltimore, MD; and e Division of Transfusion Medicine, Department of Laboratory Medicine and Pathology, Mayo Clinic, Rochester, MN, USA Keywords: cochlea, encephalopathy, plasma exchange, retina, stroke, susac syndrome, treatment, vasculopathy, young adults Received 24 August 2011 Accepted 17 November 2011 Background and purpose: There are few clinical studies on the attempted treatments and outcomes in patients with Susac syndrome (SS) (retinocochleocerebral vasculopathy). Methods: A retrospective review was performed of all patients presenting with SS at the Mayo Clinic in Rochester, Minnesota, USA (1 January 1998–1 October 2011). Results: There were 29 cases of SS (24 women, mean age at presentation, 35 years; range, 19–65; full triad of brain, eye, and ear involvement, n = 16; mean follow-up time, 29 months). Thirty CSF analyses were performed in 27 cases (mean protein 130 mg/dl, range 35–268; mean cell count 14, range 1–86). MRI of the brain showed corpus callosal involvement (79%), T2-weighted hyperintensities (93%), and gadolinium enhancement (50%). Average lowest modified Rankin Scale score was 2.5 (median 2, range 0–5). Most patients (93%) received immunosuppressive treatment, with a mean time to treatment of 2 months following symptomatic onset. Treatments included intravenous methylprednisolone or dexamethasone (n = 23), oral corticosteroids (n = 24), plasma exchange (PLEX) (n = 9), intravenous immunoglobulin (IVIg) (n = 15), cyclophosphamide (n = 6), mycophenolate mofetil (n = 5), azathioprine (n = 2), and rituximab (n = 1). Most patients also received an antiplatelet agent (n = 21). Improvement or stabilization was noted in eight of 11 cases treated with IVIg in the acute period (three experienced at least partial deterioration) and eight of nine cases of PLEX treatment (one lost to follow up). Conclusions: Susac syndrome may be severe, disabling, and protracted in some patients. PLEX may be an adjunct or alternative therapy for patients who do not experience symptomatic improvement following steroid treatment. Introduction Susac syndrome (SS) is a rare disorder of unknown pathogenesis that affects the pre-capillary arterioles of the brain, retina, and cochlea. The associated syndrome is a triad of hearing loss, branch retinal artery occlusions leading to visual loss, and cerebral symptoms that may include seizures, headaches, cognitive decline, and personality changes. Since its initial description in 1979 [1], more than two hundred cases have been reported, mostly involving young women [2]. Correspondence: Farrah J. Mateen, Department of Neurology, Johns Hopkins Hospital, Pathology Building, Room 627, 600 North Wolfe Street, Baltimore, MD 21287, USA (tel.: +410 935 5181; fax: +410 502 6736; e-mail: [email protected]). This is a Continuing Medical Education article, and can be found with corresponding questions on the Internet at http://www.efns.org/EFNS Continuing-Medical-Education-online.301.0.html. Certificates for correctly answering the questions will be issued by the EFNS. 800 Patients with SS usually experience discrete symptomatic episodes that can recur [3,4]. Although some episodes prove to be self-remitting without treatment, the clinical course cannot be readily predicted and patients may experience sequelae of epilepsy, dementia, permanent deafness, and/or visual loss. The heterogeneity and rarity of the disorder have prevented large clinical case series that include treatment. Because of a presumed autoimmune etiology, acute symptomatic treatment has justifiably centered on corticosteroids. There are no randomized trials on treatment efficacy to date. Anecdotal reports have suggested a therapeutic benefit from azathioprine, cyclophosphamide, mycophenolate mofetil, infliximab, nimodipine, antiplatelet agents, intravenous immunoglobulin (IVIg), and/or plasma exchange (PLEX) in some patients [5–18]. We aim to expand the knowledge of the clinical course of patients with SS following various attempted treatments by qualitatively and, where possible, 2012 The Author(s) European Journal of Neurology 2012 EFNS Susac syndrome quantitatively presenting our experience of the diagnosis, assessment, and management of a large series of patients with SS at a high-volume referral center. 801 All procedures were performed on the COBE Spectra (CaridianBCT; Roundlake, CO, USA). Results Methods The Mayo Clinic Institutional Review Board approved this study. A retrospective medical record review was performed of all patients with the diagnosis of SS between 1 January 1998 and 1 October 2011 at the Mayo Clinic in Rochester, Minnesota, USA. Keyword search terms included ÔSusac SyndromeÕ and Ôretinocochleocerebral vasculopathyÕ, Ôcerebral vasculopathyÕ, ÔcerebroretinovasculopathyÕ, and Ôother encephalopathyÕ. The institutional experience of SS prior to this time has been reported [3]. None of the patients included in the previous report were included in this study. Diagnoses were confirmed by review of the laboratory tests, imaging studies, and treating cliniciansÕ diagnoses. Demographic and clinical data included age, sex, and details of the symptomatic presentation, methods of diagnostic evaluation, treatment course, and any evidence of recurrence. Dates of birth, symptomatic onset, first treatment, first signs of improvement, and last follow-up were collected. A modified Rankin Scale score [19] was assigned retrospectively by the authors, based on detailed clinical notes. Magnetic resonance images of the brain were analyzed for the following: (i) evidence of lesions consistent with SS, notably punctuate T2 hyperintense lesions in the cerebral parenchyma and subcortical structures, (ii) T2 hyperintense lesions involving the corpus callosum thought to be highly characteristic of SS, and (iii) gadolinium enhancement of the T2 hyperintense lesions noted in (i) and (ii). Patient therapy was determined by the treating neurologist(s) at the time of evaluation in conjunction with a consultant rheumatologist, ophthalmologist, and/or otolaryngologist when appropriate. Use of PLEX was determined by the treating physician without any pretreatment criteria. These were not necessarily more severe cases. There are no standard algorithms for the use of steroids, IVIg, or PLEX in SS at our institution. Treatment course was assessed by the presence of symptomatic improvement documented in the medical records, corroborated by audiogram, retinal examination, and brain imaging when performed. PLEX is an extracorporeal technique for removing humoral factors such as immunoglobulins, complement, or cytokines from the blood. At our institution, the usual course of PLEX for SS consisted of a one-volume PLEX administered every other day for a planned course of five treatments. Replacement fluid was 5% albumin with the anticoagulant consisting of either acid citrate dextrose solution A (ACDA) or heparin and ACDA. Search results and patient characteristics There were 43 case records retrieved that had SS within the differential diagnosis. A total of 29 patients (24 women (83%), mean age at symptomatic presentation 35 years, range 19–65) had a diagnosis of SS. All patients were diagnosed or had the diagnosis confirmed by a neurologist. All patients underwent an extensive workup to exclude other diagnoses that may mimic SS. Patients were seen as an inpatient (n = 10), outpatient (n = 15), or both (n = 4). One patient was diagnosed during pregnancy. Patients included in this series had at least two of the three retinal, cochlear, or cerebral symptoms characteristic of SS, including 16 (55%) with the full triad of brain, vestibulocochlear, and eye involvement at the time of first assessment. Hearing was involved in 24 cases (83%), vision in 24 cases (83%), and cerebral symptoms in 26 cases (90%) (Table 1). Follow-up ranged from a single visit with further treatment and care by local physicians to more than 10 years of extended follow-up at this institution (mean 29 months (2.4 years), median 13 months, range < 1– 128 months). Average lowest modified Rankin Scale score reported was 2.5 (mRS 2 = slight disability, able to look after own affairs without assistance but unable to carry out all previous activities) [median 2, range 0 (no symptoms) to 5 (severe disability, incontinent, bedridden, and requiring constant attention for care)]. No patient is known to have died. Twenty-four additional patients had SS within the differential diagnosis of their condition but had a different final diagnosis. These alternative diagnoses were confirmed by the treating physicians to be multiple sclerosis, central nervous system lymphoma, primary central nervous system vasculitis, probable central nervous system vasculitis, WegenerÕs granulomatosis, CoganÕs syndrome, retinal vasculitis, cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy (CADASIL), cerebroretinal vasculopathy, episodic vertigo with sensorineural hearing loss, conversion syndrome, or indeterminate symptoms that lacked at least two features of the triad of SS. Investigations The diagnostic evaluation of patients with SS is summarized in Table 1. There were 30 CSF analyses in 27 individuals with an average CSF protein of 130 mg/dl 2012 The Author(s) European Journal of Neurology 2012 EFNS European Journal of Neurology 51/F 26/F 5 6 36/F 3 35/F 32/F 2 4 34/F 1 Age/sex Headaches, numbness and tingling of hands and face, visual field defect, hearing loss, tinnitus Vertigo, diplopia, visual loss, tingling of hands and feet, and amnestic episodes Tongue numbness, TIA-like episodes of upper extremity numbness, tingling, and weakness, photosensitivity, HA Unilateral tinnitus, hearing loss, unilateral visual loss, disequilibrium memory loss, uncontrollable laughter Segmental visual loss, vertigo Diplopia, stroke-like episodes of right hemiparesis, hearing loss, episodic gait instability, slurred speech, numbness in UE Presenting symptoms/ clinical findings/first symptom(s) Out Both B, H, V Out Out Out In Inpatient/ outpatient evaluation (episode #) H, V B, H, V B, V B, V B, H, V Involvement of brain (B), hearing (H), and vision (V) 185 Normal 47 105, 76 161 101 CSF protein 70 5 2 86, 6 11 2 CSF cell count Table 1 Investigations and demographic features of patients with susac syndrome 0 n/a 0 <2 0 n/a Oligoclonal bands Low-frequency hearing loss Bilateral hearing loss; right at 40 DB (250–1000Hz, 80dB at 1000–6000 Hz) Bilateral asymmetric hearing loss, particularly in lower frequencies n/a Low- to mid-frequency hearing loss n/a Audiogram ANA mildly positive Rheumatoid factor mildly positive; mild diffuse lymph adenopathy (biopsy negative for malignant cells) EEG: diffuse abnormalities VEP: abnormal prolongation bilaterally Y Y N Y Y N Y Y Y Y Symptoms began postpartum Positive FTA · 2 (negative RPR); elevated IgG synthesis rate Y Y MRI T2 hyperintensities (y/n) Symptoms during 3rd trimester of pregnancy Other findings MRI corpus callosum involvement (y/n) N N N N Y N MRI gadolinium enhancement Normal Normal Normal Normal Normal Normal Cerebral angiogram or MRA findings 802 F. J. Mateen et al. 2012 The Author(s) European Journal of Neurology 2012 EFNS European Journal of Neurology 30/M 46/M 23/F 50/F 36/F 20/F 7 8 9 10 11 12 Age/sex 2012 The Author(s) European Journal of Neurology 2012 EFNS European Journal of Neurology Gait ataxia, uni lateral hearing loss, confusion, pseudobulbar affect, urinary incontinence Intractable HA, unilateral hearing loss, progressive cognitive decline, scintillating scotoma, photophobia, N&V Episodes of visual loss, hearing loss, disorientation, imbalance, memory loss, hallucinations, lethargy Headaches, unilat eral visual loss, imbalance, vertigo, hemiparesis Confusion, cognitive difficulty, new headaches, unilateral hearing loss, and tinnitus Vertigo, numb hands, vision loss, hearing loss, cognitive decline, agitation Presenting symptoms/ clinical findings/first symptom(s) Table 1 (Continued ) In In B, H, V Out B, H B, H, V Both In B, V, H B, H, V In Inpatient/ outpatient evaluation (episode #) H, B Involvement of brain (B), hearing (H), and vision (V) 170 106 171, 157 133 Ôslightly elevatedÕ 188 CSF protein 20 2 12, 6 10 8 16 CSF cell count n/a 1 n/a n/a n/a 1 Oligoclonal bands 50% reduced hearing left ear Sensorineural hearing loss (250–2000 Hz range on one ear, all frequencies other ear) n/a n/a n/a n/a Audiogram None None ANA positive 1:80, CK = 5000, LDH 338, ESR 24. Brain biopsy: scant perivascular chronic inflammation, microglial activation and mild nonspecific gliosis EEG: generalized slowing None Other findings Y Y Y Y Y Y n/a Y Y Y Y MRI T2 hyperintensities (y/n) Y MRI corpus callosum involvement (y/n) Y Y N n/a N Y MRI gadolinium enhancement n/a Normal Normal Normal Normal Normal Cerebral angiogram or MRA findings Susac syndrome 803 37/F 44/F 19/F 24/F 16 17 18 23/F 14 15 35/F 13 Age/sex Headaches, R vi sual loss, R hearing loss, cognitive difficulty, gait ataxia, R facial sensory disturbance, confusion, pseudobulbar affect Segmental visual loss, dizziness, weak and numb UE Episodic loss of consciousness, transient visual disturbance, progressive cognitive decline, and memory loss Headache, hearing loss, blurry vision, disorientation, personality change, and cognitive decline Vertigo, tinnitus, bilateral hearing loss, segmental visual loss Headaches, blurry vision, hearing loss, confusion, memory loss, gait instability Presenting symptoms/ clinical findings/first symptom(s) Table 1 (Continued ) B, H, V Out In Both B, H, V B, H, V Out Out B, H, V V, B Out Inpatient/ outpatient evaluation (episode #) B, H, V Involvement of brain (B), hearing (H), and vision (V) n/a 126 131 n/a 59 177 CSF protein n/a 3 0 n/a 4 n/a CSF cell count n/a n/a 0 n/a n/a n/a Oligoclonal bands Moderate left hearing loss 250–1000 Hz range n/a 10% word recognition in left ear Normal n/a n/a Audiogram Prothrombin 20 210 A mutation heterozygote Y N N Y N Y Y MRI T2 hyperintensities (y/n) Y Y None None N Y Y None Positive IgM and IgG anticardiolipin antibody, V Leiden heterozygous None Other findings MRI corpus callosum involvement (y/n) N Y Y N Y N MRI gadolinium enhancement Normal Normal Normal Normal Normal n/a Cerebral angiogram or MRA findings 804 F. J. Mateen et al. 2012 The Author(s) European Journal of Neurology 2012 EFNS European Journal of Neurology 46/F 28/F 27/M 43/F 20/F 33/F 57/F 39/M 25/F 19 20 21 22 23 24 25 26 27 Age/sex 2012 The Author(s) European Journal of Neurology 2012 EFNS European Journal of Neurology Headache, nausea, vomiting, tinnitus, hearing loss, dizziness, short-term memory loss Visual loss, hearing loss, headache Disorientation, visual loss, headache Disorientation, hearing loss Disorientation, urinary retention, gait instabliity Right ear discomfort, gait instability, disorientation Scotomatous vi sual loss, vertigo, worsening gait, tinnitus, headache, paresthesias of face and extremities Hearing loss, headache, blurred vision Hearing loss, headache, vertigo, left numbness, gait unsteadiness Presenting symptoms/ clinical findings/first symptom(s) Table 1 (Continued ) In B, V Out Out B, H B, H Out Out Out In Out Both Inpatient/ outpatient evaluation (episode #) B, V H, V B,H,V B, H H,V B, H, V Involvement of brain (B), hearing (H), and vision (V) 147 79 248 84 84 > 200 164 35 83, 57 CSF protein 14 4 n/a 11 2 50 5 1 0, 0 CSF cell count 0 0 n/a n/a 0 0 0 0 n/a Oligoclonal bands Not done but had abnormal brainstem evoked potentials Sensorineural hearing loss bilaterally (1000–8000 Hz range) n/a Normal Unilateral 6000 and 8000 Hz loss Mild R and moderate– severe left sensorineural hearing loss, all frequencies Mostly normal but loss at 1500 Hz left and 2000 Hz right ear n/a Low-frequency hearing loss left, low- and high-frequency loss right Audiogram Y Y None None Y Y Y None None None Y Y None None N Y None ANA (1:40) Other findings MRI corpus callosum involvement (y/n) Y Y Y Y Y Y Y Y Y MRI T2 hyperintensities (y/n) Y n/a n/a N N Y Y N Y MRI gadolinium enhancement *Normal Normal Normal Normal *Normal Normal n/a Normal n/a Cerebral angiogram or MRA findings Susac syndrome 805 65/M 29 *Digital subtraction angiography; ANA, antinuclear antibody; B, brain; EEG, electroencephalogram; FTA, fluorescent treponemal antibody absorption; H, hearing; HA, headache; MRI, magnetic resonance imaging study of the brain; L, left; N, no; N&V, nausea and vomiting; n/a, not done; R, right; VEP, visual evoked potentials; V, vision; Y, yes. Normal N N In B, H, V 96 2 0 Moderate–se vere bilateral sensorineural hearing loss None Y Normal N Y Y n/a 0 19 In 32/F 28 Age/sex Acute unilateral hearing loss, visual loss, disorientation Headache, disori entation B, H, V 268 Other findings Audiogram Oligoclonal bands CSF cell count Inpatient/ outpatient evaluation (episode #) Presenting symptoms/ clinical findings/first symptom(s) Involvement of brain (B), hearing (H), and vision (V) CSF protein None MRI gadolinium enhancement MRI corpus callosum involvement (y/n) MRI T2 hyperintensities (y/n) Cerebral angiogram or MRA findings F. J. Mateen et al. Table 1 (Continued ) 806 (median 129, range 35–268, normal range 15–45 mg/dl) and an average cell count of 14 cells/ml (median 5, range 0–86, normal range 0–5 cells/ml). MRI was performed in all cases (Fig. 1). Corpus callosal involvement of lesions was noted in 23/29 cases (79%). Punctate T2-weighted hyperintense lesions were seen in 26 individuals (absent in two cases, not available in one case, 93%). Gadolinium enhancement of lesions occurred in 13 cases (available in 26 cases, 50%). One patient had the diagnosis confirmed by brain biopsy (Fig. 2). Treatment and outcomes Two patients (cases 4 and 20) were untreated. Mean time to treatment was 2 months (median 1 month) amongst the 27 cases who received immunosuppressive therapy (Table 2). PLEX was used in nine cases (range of 3–10 exchanges). Symptomatic improvement was observed in six cases, stabilization was in two cases, and one case was lost to follow up. No patient continued to worsen. Amongst the patients treated with IVIg, there were 11 cases who received initial treatment with IVIg (cases 6, 9, 10, 11, 14, 17, 22, 24, 26, 28, and 29) and three cases who were observed whilst receiving maintenance monthly IVIg (cases 21, 23, and 25). Amongst the 11 cases who were evaluated in the acute symptomatic treatment phase and treated with IVIg, improvement was noted in six cases, stability or modest improvements in two cases, deterioration in symptoms in two cases, and mixed results (both improvement and deterioration) in one case. Additional treatments included intravenous methylprednisolone or dexamethasone (n = 23), oral corticosteroids (n = 24), mycophenolate mofetil (n = 5), cyclophosphamide (n = 5), azathioprine (n = 2), and rituximab (n = 1). Most patients also received an antiplatelet agent: aspirin (n = 18), clopidogrel (n = 2), and aspirin and dipyridamole (n = 1). Nimodipine was taken by five individuals. Discussion Given the variable course and rarity of SS, there are no prospective studies on the best treatment of patients. Retrospective studies are also challenging given the wide range of symptomatic manifestations of SS, delay to diagnosis in many cases, lack of diagnostic biomarkers, and limited literature on the natural history of the disease. In our experience, which is subject to referral bias, not all patients with SS have a symptomatic response to corticosteroids. Most patients were treated with additional immunosuppressive therapy with the goal of achieving symptomatic remission in the acute 2012 The Author(s) European Journal of Neurology 2012 EFNS European Journal of Neurology Susac syndrome Figure 1 Axial view of a T1-weighted MRI of the brain with gadolinium contrast, demonstrating involvement of the cochlea in a patient with diagnosed Susac syndrome. period. This is especially true for patients with severe presentations, including dementia, recurrent seizures, and recurrent visual loss despite treatment with corticosteroids. There are several reports of refractory cases of SS treated with IVIg in the acute period [7,8,10–12]. Rarely, IVIg may cause additional ischaemic changes in the microvasculature [20,21], which is a theoretical concern in SS, given the arteriolar distribution of the disease. By contrast, reports of patients with SS treated with PLEX are exceptional. Five patients with SS are reported to have been treated with PLEX [3,5–8]. The positive therapeutic effects probably involve removal of humoral factors from the patientÕs blood including immunoglobulins, complement, and/or cytokines [22]. 807 The putative pathogenic antibody or antibodies are probably removed or reduced in this process. Many cases of SS are treated with antiplatelet agents including aspirin and clopidogrel given the arteriolar involvement seen under fluorescein angiography of the retina and cerebral pathology [3,4]. Possible arteriolar vasospasm has prompted the use of the calcium channel blocker nimodipine, which is almost always an adjunct treatment. These treatments are difficult to assess for efficacy independently of immunosuppressive treatment. These findings are not definitive evidence for the use of PLEX in the treatment of SS. Our observations are rather intended to be foundational for prospective studies on the treatment of patients with SS. Based on our data alone, we cannot confirm that any treatment improved the course of patients with Susac syndrome. There are only occasional cases of untreated individuals, including just two in this series, some of whom experience spontaneous resolution of symptoms without immunosuppressive treatment. It is unclear whether the currently employed treatments hasten symptomatic recovery. The appropriate duration of treatment requires proper study and presently is anecdotal. Our study had limitations. This was a retrospective, observational study and, at times, had incomplete data. Follow-up was not consistent amongst patients, and not all patients received their complete care for SS at this institution. There are no defined criteria for SS. Therefore, we considered cases to have SS if they had at least two of the three features of the triad of retinal, cochlear, or brain involvement during our observation period. Deficits from SS are difficult to quantify with standard functional outcome scales, such as the modified Rankin Scale; therefore, the degree of cognitive and functional deficits can be underestimated. However, our findings report the largest series of SS to date including the careful evaluation and confirmation of this diagnosis in a large referral center over the (a) Figure 2 Pathologic features of Susac syndrome in brain biopsy of case 21. Histologic sections demonstrate aggregates of macrophages representing a subacute microinfarct (arrowheads) associated with a small vessel (large arrow). Rare isolated acute ischaemic neurons are also present (small arrows) (a). Distinct microthrombi were also identified within leptomeningeal vessels (arrow) (b). 2012 The Author(s) European Journal of Neurology 2012 EFNS European Journal of Neurology (b) 26/F 30/M 46/M 23/F 8 9 35/F 4 6 7 36/F 3 51/F 32/F 2 5 34/F 1 Age (years /sex) 6 3–4 Uncertain 1 1 5 1 0.25 2 Duration of symptoms prior to treatment months) ASA ASA ASA-Dipyri damole Clopidogrel – ASA ASA ASA ASA Antiplatelet medication N N Y Y N N 2 pills only Y Y Oral steroids (Y/N) Y Y Y Y Y N Y Y N IV steroids Nimodipine, recommended to have cyclophosphamide 2 mg/kg PO daily · 6 months Cyclophosphamide – – – – Nimodipine – – Other treatments Table 2 Treatment and clinical course of patients with susac syndrome – Daily · 5, then 1 month later 4 more doses Daily · 5 days Every other day · 5 – – 5 5 2 2 0 5 0 Daily · 3 – 0 0 Every other day · 5 Every other day · 5 PLEX – 3 – – – – – – IVIg (# of days) Lowest modified rankin scale score Initially returned to baseline with IVIg maintained on monthly IVIg and Solu-Medrol; recurrence 1 year later with some improvement with PLEX but did not return to baseline Improved hearing and sight Improved Improved following IV steroids on 2 occasions Stable Weakness improved with IV steroids but later had visual changes (halos around objects), ear pressure, and objective hearing loss Initial episode resolved without treatment; later episode treated with IVIg Improved Stabilized symptoms postpartum Improvement following treatment Stable but poor baseline Some improvement with IVIg and PLEX but continually worsening baseline over 15 months Improvement without treatment then recurrent eye symptoms 6 years later No recurrent symptoms n/a Improved Recurrence after oral steroid taper Later episodes of visual and hearing loss Recommended to have PLEX but LFU Outcome 15 9 95 32 62 88 13 128 9 No. of months of follow-up available 808 F. J. Mateen et al. 2012 The Author(s) European Journal of Neurology 2012 EFNS European Journal of Neurology 50/F 36/F 20/F 35/F 23/F 37/F 44/F 19/F 24/F 36/F 10 11 12 13 14 15 16 17 18 19 Age (years /sex) 2012 The Author(s) European Journal of Neurology 2012 EFNS European Journal of Neurology 3 3.5 1 3 1 1.5 0.5 1.25 2 <1 Duration of symptoms prior to treatment months) Table 2 (Continued ) ASA Clopidogrel ASA ASA ASA ASA ASA ASA – – Antiplatelet medication Y Y Y Y Y Y Y Y Y Y Oral steroids (Y/N) Y Y Y N N Y Y Y Y N IV steroids Cyclophosphamide 100mg daily Azathioprine Nimodipine – Mycophenolate mofetil, Nimodipine – Nimodipine – – Cyclophosphamide Other treatments – 2 doses, then relapse then 5 every other day with improvement, then 3· per week – – 5 every other day than weekly – – – 5 doses on 2 different occasions Every other day · 5 IVIg (# of days) – – Every other day · 5; 2 separate occasion – Every other day · 5 Every other day · 5, then relapse then 2 more doses – – Every other day · 5 Stable, unclear whether improvement occurred 0 1 One relapse while on a 15-month course of cyclophospha mide, treated with steroids Improved following PLEX, then cognitive and gait deficits relapsed and then repeat treatment Improved 4 2 Improved Deteriorated Symptomatic response to IVIg reported in past No response to IV/ PO steroids, 4 weeks later had response to IVIg Improved objective gait speed and coordination Improved Improvement following treatment 0 4 2 4 4 0 PLEX – Lowest modified rankin scale score 24 Visual changes off immuno suppression nearly 2 years later treated with repeat PLEX No recurrent symptoms for nearly 5 years, persistent mild visual loss 59 43 15 9 73 76 <1 3 <1 No new symptoms No new symptoms Cognitive improvement but required wheelchair at 7 months No new symptoms n/a LFU Continued progression then LFU Improvement Outcome No. of months of follow-up available Susac syndrome 809 32/F 65/M 28 29 0.5 0.5 0.25–0.5 0.75 0.25 0.25 ÔmonthsÕ 1.75 4 No Treatment – ASA ASA ASA – – ASA – – ASA Antiplatelet medication Y Y Y Y Y Y Y Y Y N Oral steroids (Y/N) Y Y Y Y Y Y Y Y Y N IV steroids Cyclophosphamide recommended post-dismissal Mycophenolate mofetil Cyclophosphamide, later rituximab Mycophenolate mofetil Mycophenolate mofetil when symptoms remitted Mycophenolate mofetil when symptoms remitted – Azathioprine – Other treatments – – – Daily · 5 Daily · 5, then once monthly – Daily · 7 – – – – – – – PLEX Maintained on 0.25 g/kg every 3 weeks 5 doses days, then weekly · 3 Maintained on 2 g/kg monthly 5 doses daily, then once weekly Maintained on once monthly dose – IVIg (# of days) 4 4 3 5 4 4 1 4 2 1 Lowest modified rankin scale score Cognition improved, hearing loss worsened Cognition subtly improved Improved Stable Improved cognition Improved Improved vision and hearing loss Cognition significantly improved Stable Improved Improvement following treatment Persistent cognitive def icits Mild improvement in hearing loss and headaches – Gait improvement, cognitive gains to nearly normal Markedly improved cognition, legs weak, walker dependent – Hearing loss and vision improved Slight residual memory deficits Persistent memory problems, improved gait Normal examination Outcome – – 8 9 13 11 3 3 24 8 No. of months of follow-up available ASA, aspirin; F, female; LFU, lost to follow up; IV, steroids; IVIg, intravenous immunoglobulins; M, male; mRS, modified Rankin Scale score; N, no; n/a, not available; PLEX, plasma exchange; PO, by mouth; Y, yes. 25/F 27 33/F 24 39/M 20/F 23 26 43/F 22 57/F 27/M 21 25 28/F 20 Age (years /sex) Duration of symptoms prior to treatment months) Table 2 (Continued ) 810 F. J. Mateen et al. 2012 The Author(s) European Journal of Neurology 2012 EFNS European Journal of Neurology Susac syndrome course of nearly 14 years. Our findings help establish the clinical spectrum of SS, including a depiction of the treated history of the disease. Our qualitative analysis also suggests that PLEX is worthy of further evaluation, perhaps in a matched case control design compared to IVIg. Given that SS may rarely be fatal and is often disabling and severe [8,13], we propose that PLEX should be considered as an adjunct or alternative treatment to steroids in patients who do not improve with IVIg. Our clinical cohort underscores the value and necessity of prospective studies of this rare condition. Such studies would be most effectively achieved through an international collaboration of researchers, so that patients can participate in the acute symptomatic period from multiple centers. The use of standardized and uniform clinical assessment tools – where possible, also including audiogram and visual testing – will further help clarify the degree of impairment and long-term disability. Such tests must be carried out at sufficiently timed intervals to capture the fluctuating and occasionally recurrent nature of the disorder. In the longer term, outcome studies of the degree of disability and recovery through proposed international registries will provide valuable new information to the growing number of patients diagnosed with SS. Acknowledgements Dr. Mateen is supported by the American Academy of Neurology Practice Research Fellowship grant. Disclosure of conflict of interests The authors declare no financial or other conflict of interests. References 1. Susac JO, Hardman JM, Selhorst JB. Microangiopathy of the brain and retina. Neurology 1979; 29: 313–316. 2. Rennebohm R, Susac JO, Egan RA, Daroff RB. SusacÕs syndrome – update. J Neurol Sci 2010; 299: 86–91. 3. Petty GW, Engel AG, Younge BR, et al. Retinocochleocerebral vasculopathy. Medicine (Baltimore) 1998; 77: 12–40. 4. Petty GW, Matteson EL, Younge BR, et al. Recurrence of Susac syndrome (retinocochleocerebral vasculopathy) after remission of 18 years. Mayo Clin Proc 2001; 76: 958–960. 811 5. Bogousslavsky J, Gaio JM, Caplan LR, et al. Encephalopathy, deafness and blindness in young women: a distinct retinocochleocerebral arteriolopathy? J Neurol Neurosurg Psychiatry 1989; 52: 43–46. 6. Vila N, Graus F, Blesa R, Santamaria J, Ribalta T, Tolosa E. Microangiopathy of the brain and retina (SusacÕs syndrome): two patients with atypical features. Neurology 1995; 45: 1225–1226. 7. Do TH, Fisch C, Evoy F. Susac syndrome: report of four cases and review of the literature. AJNR Am J Neuroradiol 2004; 25: 382–388. 8. Hahn JS, Lannin WC, Sarwal MM. Microangiopathy of brain, retina, and inner ear (SusacÕs syndrome) in an adolescent female presenting as acute disseminated encephalomyelitis. Pediatrics 2004; 114: 276–281. 9. Snyers B, Boschi A, De Potter P, et al. Susac syndrome in four male patients. Retina 2006; 26: 1049–1055. 10. Fox RJ, Costello F, Judkins AR, et al. Treatment of Susac syndrome with gamma globulin and corticosteroids. J Neurol Sci 2006; 251: 17–22. 11. Rennebohm RM, Susac JO. Treatment of SusacÕs Syndrome. J Neurol Sci 2007; 257: 215–220. 12. Maillart E, Deschamps R, Moulignier A, et al. [Susac syndrome: study of five cases]. Rev Neurol (Paris) 2009; 165: 575–582. 13. Saux A, Niango G, Charif M, et al. SusacÕs syndrome, a rare, potentially severe or lethal neurological disease. J Neurol Sci 2010; 297: 71–73. 14. Wildemann B, Schülin C, Storch-Hagenlocher B, et al. SusacÕs syndrome: improvement with combined antiplatelet and calcium antagonist therapy. Stroke 1996; 27: 149– 151. 15. Papo T, Biousse V, Lehoang P, et al. Susac syndrome. Medicine (Baltimore) 1998; 77: 3–11. 16. OÕHalloran HS, Pearson PA, Lee WB, et al. Microangiopathy of the brain, retina, and cochlea (Susac syndrome). A report of five cases and a review of the literature. Ophthalmology 1998; 105: 1038–1044. 17. Aubart-Cohen F, Kelin I, Alexandra JF, et al. Long-term outcome in Susac syndrome. Medicine (Baltimore) 2007; 86: 93–102. 18. Hardy TA, Garsia RJ, Halmagyi GM, et al. Tumor necrosis factor (TNF) inhibitor therapy in SusacÕs syndrome. J Neurol Sci 2011; 302: 126–128. 19. Rankin J. Cerebrovascular accidents in patients over the age of 60. I. General considerations. Scott Med J 1957; 2(4): 127–136. 20. Marie I, Maurey G, Herve F, et al. Intravenous immunoglobulin-associated arterial and venous thrombosis: report of a series and review of the literature. Br J Dermatol 2006; 155: 714–721. 21. Paran D, Herishanu Y, Elkayam O, et al. Venous and arterial thrombosis following administration of intravenous immunoglobulins. Blood Coagul Fibrinolysis 2005; 16: 313–318. 22. Linker RA, Gold R. Use of intravenous immunoglobulin and plasma exchange in neurological disease. Curr Opin Neurol 2008; 21: 358–365. 2012 The Author(s) European Journal of Neurology 2012 EFNS European Journal of Neurology