Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
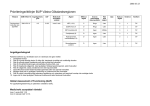
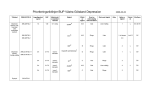
Ortodontisk forskning – vad är på gång på Malmöfakulteten? - Evidensbaserad forskning om behandlings- och kostnadseffektivitet Hur påverkas livskvaliteten av malocklusioner Vilka sidoeffekter som ”white spot leisons”, smärta och obehag förekommer och hur kan sidoeffekter undvikas Lars Bondemark och Mikael Sonesson Avdelningen för Ortodonti Odontologiska fakulteten Malmö högskola, Sverige Förutsättningar för att forska • • • • • Nyfikenhet Intresse för ämnet Kreativitet Noggrannhet Uthållighet, långsiktigt mål Vad behöver man kunna? - Hur förbereder man sig? Fråga Projektidé Litteraturgenomgång Problemformulering Hypotes Material och metoder Hur ställer man en bra forskningsfråga? PICO P I C O Population Intervention Control Outcome PICO P I C O Population Intervention Control Outcome Hur effektiv är en Quad helix i jämförelse med en expansionsplåt avseende kostnadseffektivitet för patienter med korsbett i växelbettet? Ytterligare förberedelser • Informationssökning och litteraturstudier • Forskningsprogram och flödesschema PubMed http://www.ncbi.nlm.nih.gov/sites/entrez http://www.cochrane.org/ Ytterligare förberedelser inför studien • • • • Etisk prövning Statistikkonsult Manualer Finansiellt stöd Patienter Vilka? Hur många? Inklusions- och exklusionskriterier? Patienter - Urvalet? Patienter - Urvalet? - patienter som avgränsas av inklusions- och exklusionskriterierna Hur ska patienterna fördelas ? Ska patienterna randomiseras? Strong or weak evidence Strong Systematic Review and Meta-analysis gold standard RCT Cohort studies Case control studies Weak Case series Case reports No Ideas, editorials, opinions Stark eller svag evidens • prospektiva studier är bättre än retrospektiva • kontrollerade studier är bättre än studier som jämför situationen före och efter i enbart en grupp (fallserie) • stora material är att föredra framför små eftersom med små material är risken större för att förväxlingsfaktorer (confounders) kan påverka utfallen Det randomiserade kontrollerade försöket När är det bra? Varför tjatar vi om det hela tiden? Randomiserad kontrollerad studie (RCT) “golden standard”: ger mer tillförlitlig evidens än okontrollerade studier eller expertutlåtande för att... Randomiserad kontrollerad studie (RCT) • behandlingen styrs av slumpen • faktorer under studieperioden som vi inte kan kontrollera (“confounders” – förväxlingsfaktorer) drabbar grupperna lika • extra lämplig då två eller flera behandlingar ska jämföras Men…, det finns svårigheter! • prospektiva studier tar lång tid att genomföra – blir därför ofta dyra • etiska problem - speciellt om obehandlade kontroller används Vad ska mätas? Patientnära effektmått Hörnstenar: - behandlingseffekter på kort/lång sikt - kostnadseffektivitet - patienters upplevelser (smärta/obehag) - livskvalitet - sidoeffekter Betydelsen av blindning Minskar de systematiska felen Blinda det som går att blinda! Betydelsen av bortfallet Var snäll mot patienterna så att de stannar kvar i försöket Ett stort bortfall är alltid problematiskt – tillförlitligheten av resultaten sänks vid stora bortfall Sammanfattat - en bra fråga - tillräckligt antal av patienter - randomisering och blindning - minimera bortfallet Avhandlingar 2007-2015 Gudrun Lillemor Cecilia Ingela Liselotte Ingalill Sofia PÅ GÅNG… Mikael Sonesson, ortodonti, Odontologiska fakulteten, Malmö högskola LOW-LEVEL LASER THERAPY TO IMPROVE ORTHODONTIC TREATMENT - A SYSTEMATIC REVIEW Emelie De Geer, leg. tandläkare, Sundsvall Jaqueline Subraian , leg. tandläkare, Örebro Sofia Petrén, övertandläkare, Odont dr, Odontologiska fakulteten Malmö Mikael Sonesson, övertandläkare, Odont dr, Odontologiska fakulteten Malmö VARFÖR SYSTEMATISK LITTERATURÖVERSIKT? Ny kunskap Ny teknik Forskning och utvärdering Rutiner Klinisk praxis EVIDENSBASERAD VÅRD (EBV) • Använda bästa tillgängliga vetenskapliga bevis när det gäller beslut om vård • Tillförsäkra patienten bästa behandling, dvs mest effektiva och minst riskabla behandling • Utnyttja resurserna på bästa sätt, dvs i första hand ta bort metoder som inte gör nytta FINNS OLIKA TYPER AV STUDIER BEVISBÄRIGHET Systematic Review, Meta-analysis BEVISBÄRIGHET RCT Systematic Review, Meta-analysis BEVISBÄRIGHET RCT Cohort studies Systematic Review, Meta-analysis BEVISBÄRIGHET Systematic Review, Meta-analysis RCT Cohort studies Case control studies BEVISBÄRIGHET Systematic Review, Meta-analysis RCT Cohort studies Case control studies Case series BEVISBÄRIGHET Systematic Review, Meta-analysis RCT Cohort studies Case control studies Case series Case reports BEVISBÄRIGHET Systematic Review, Meta-analysis RCT Cohort studies Case control studies Case series Case reports Ideas, Editorials, opinions SYSTEMATISK ÖVERSIKT Bedömer enligt särskild metod hur bra studierna är på att besvara den specifika forskningsfrågan Studiekvalitet och evidensstyrka • Studiekvalitet avser den vetenskapliga kvaliteten hos en enskild studie och dess förmåga att besvara en viss fråga på ett tillförlitligt sätt • Evidensstyrkan uttrycker det sammanlagda vetenskapliga underlaget för en slutsats, dvs hur många högkvalitativa studier som stöder slutsatsen Evidensstyrka Starkt vetenskapligt underlag; • Bygger på studier med hög eller medelhög kvalitet utan försvagande faktorer vid en samlad bedömning Evidensstyrka Måttligt vetenskapligt underlag; • Bygger på studier med hög eller medelhög kvalitet med förekomst av försvagande faktorer vid en samlad bedömning Evidensstyrka Begränsat vetenskapligt underlag; • Bygger på studier med hög eller medelhög kvalitet med kraftigt försvagandefaktorer vid en samlad bedömning Evidensstyrka Otillräckligt vetenskapligt underlag; • När studier saknas, tillgängliga studier har låg kvalitet eller där studier av likartad kvalitet visar motsägande resultat, anges det vetenskapliga underlaget som otillräckligt ALLTSÅ: DEN SYSTEMATISKA LITTERATURÖVERSIKTEN GRANSKAR PÅ ETT KONSEKVENT SETT STUDIERNAS VETENSKAPLIGA KVALITET OCH TILLFÖRLITLIGHET. PÅ SÅ SÄTT HJÄLPER ÖVERSIKTEN TILL ATT ÄVEN IDENTIFIERA KUNSKAPSLUCKOR LOW-LEVEL LASER THERAPY TO IMPROVE ORTHODONTIC TREATMENT - A SYSTEMATIC REVIEW Emelie De Geer, leg. tandläkare, Sundsvall Jaqueline Subraian , leg. tandläkare, Örebro Sofia Petrén, övertandläkare, Odont dr, Odontologiska fakulteten Malmö Mikael Sonesson, övertandläkare, Odont dr, Odontologiska fakulteten Malmö BAKGRUND - Laser har använts sedan 1960-talet BAKGRUND - Laser har använts sedan 1960-talet - Light Amplification by Stimulated Emission of Radiation = LASER Light Oscillation by Stimulated Emission of Radiation = LOSER - BAKGRUND - Laser i tandvården används i alla specialiteter; Först endast kirurgisk laser, senare även ”terapilaser” - LLLT BAKGRUND - Få bieffekter har setts med terapilaser BAKGRUND OrthoPulse™ TERAPILASER - Subcellulära fotoreceptorer i mitokondrierna - Reagerar på synligt rött ljus och nära infrarött ljus TERAPILASER - Elektrontransports- & andningskedja, oxidation ökad metabolisk process TERAPILASER - Hämmar fibroblasters produktion av PGE2 TERAPILASER - Stimulering av kollagenproduktion TERAPILASER - Vasodilatation via relaxering av glatt muskulatur TERAPILASER Påskyndar vävnadsremodellering snabbare tandförflyttning TERAPILASER Modifierar akut inflammation minskad akut smärta SYFTE/FRÅGESTÄLLNING Vilket vetenskapligt underlag finns för terapilaser som metod för att; • påskynda tandförflyttning? • förhindra recidiv? • minska akut smärta? HYPOTES Det vetenskapliga underlaget otillräckligt för att bestämma om LLLT är en effektiv metod för att kunna; • accelerera tandförflyttning • förhindra recidiv • minska akut smärta under ortodontisk behandling hos barn och unga METOD Systematisk litteratursökning; • PubMed • Cochrane • Scitation Kvalitetsanalys enligt SBUs riktlinjer METOD METOD RESULTAT RESULTAT RESULTAT: ACCELERATION Antal studier Metod Laser Strålningstillfällen Kontroll Effektmått Resultat Kvalitet 3 Retraktion av hörntänder GaAlAs > 1 ggn/vecka Split mouth Avstånd i mm 20-58 % ökad tandförflyttningshastighet Medel RESULTAT: RECIDIV Inga identifierade artiklar som matchade inklusionskriterier RESULTAT: SMÄRTA Antal studier Metod Laser Strålningstillfällen Kontroll Effektmått Resultat Kvalitet 13 Smärta vid fast app. eller sep. lig. GaAlAs HeNe CO2 AlGaInP En till flera strålningstillfällen Kontroll Placebo (Flertal split mouth) Maxsmärta Smärtdebut Förändring i smärta m.m. mha VAS Upp till 50 % minskad smärta Låg Medel Hög DISKUSSION - Tandförflyttningshastighet: 3 studier, bedömdes vara av en medelhög kvalitet, begränsat vetenskapligt underlag Smärta: 1 högkvalitativ studie, begränsat vetenskapligt underlag oklar kostnad för utrustning DISKUSSION - Tandförflyttningshastighet: 3 studier, bedömdes vara av en medelhög kvalitet, begränsat vetenskapligt underlag Smärta: 1 högkvalitativ studie, begränsat vetenskapligt underlag Oklar kostnad för utrustning DISKUSSION - Tandförflyttningshastighet: 3 studier, bedömdes vara av en medelhög kvalitet, begränsat vetenskapligt underlag Smärta: 1 högkvalitativ studie, begränsat vetenskapligt underlag Oklar kostnad för utrustning Konsensus saknas kring laserschema verkningsmekanism delvis oklar DISKUSSION - Tandförflyttningshastighet: 3 studier, bedömdes vara av en medelhög kvalitet, begränsat vetenskapligt underlag Smärta: 1 högkvalitativ studie, begränsat vetenskapligt underlag Oklar kostnad för utrustning Konsensus saknas kring laserschema Verkningsmekanism delvis oklar KONKLUSION Terapilaser som metod för att; 1. påskynda ortodontisk tandförflyttning 30%, 2. minska akut smärta vid ortodontisk behandling genom att smärtan minskade generellt KONKLUSION LLLT kan underlätta den ortodontiska behandlingen med avseende på behandlingstid och smärta MEN! Fler väldesignade högkvalitativa studier fordras BAKGRUND Kunskapsluckor finns avseende: • prevalens av bettavvikelser samt dess utveckling på individnivå från mjölktandsbettet till det permanenta bettet • bettavvikelsers betydelse för barn och ungdomars livskvalitet SYFTE Fastställa prevalensen och självkorrigering av bettavvikelser från mjölktandsbettet till det unga permanenta bettet 3 år 7 år 11.5 år SYFTE Relatera prevalensen av bettavvikelser till tänkbara etiologiska faktorer som sugvanor 3 år 7 år 11.5 år MATERIAL MATERIAL • Barn födda 2000 - 2002 • Barnen undersöktes vid 3 tillfällen • Genomsnittlig ålder vid respektive undersökningstillfälle var 3, 7 och 11.5 år • En undersökare (LD) vid 3 och 7 års ålder och två vid 11.5 år (LD och BL) 3 yrs Subjects N = 457 Declined to participate, N = 41 Left the district/unable to reach, N = 30 7 yrs Subjects N = 386 Declined to participate, N = 75 Left the district/unable to reach , N = 34 11.5 yrs Subjects N = 277 BORTFALL • Totalt bortfall 39.4 % mellan 3 och 11.5 års ålder • 14 % hade flyttat, 25 % tackade nej till fortsatt deltagande • Inga skillnader sågs avseende kön, klinik, prevalens av bettavvikelse eller sugvana RESULTAT Prevalens av bettavvikelser 3 yrs 70 % 7 yrs 58 % 11.5 yrs 71 % Vanligaste bettavvikelsen vid 3 år 50 % FRONTALT ÖPPET BETT Vanligaste bettavvikelsen vid 7 år 28 % POSTNORMAL RELATION Vanligaste bettavvikelsen vid 11.5 år 31 % TRÅNGSTÄLLNING Självkorrigering Självkorrigering observerades bland samtliga bettavvikelser mellan 3 och 11.5 års ålder Det varierade mellan 43 % för djupa bett till 100 % för frontala öppna bett 83 % bland enkelsidiga korsbett Exempel på självkorrigering 3 yrs 7 yrs 11.5 yrs Exempel på självkorrigering 3 yrs 7 yrs 11.5 yrs Utveckling av nya bettavvikelser Nya bettavvikelser utvecklades för alla avvikelser mellan 3 och 11.5 års ålder utom för Klass III bett och frontala öppna bett Exempel på utveckling av nya bettavvikelser 3 yrs 7 yrs 11.5 yrs Exempel på utveckling av nya bettavvikelser 7 yrs 11.5 yrs Ortodontiskt behandlingsbehov enligt IOTN-DHC index bland 11.5 åringar (n = 277). Grade of treatment need n % No need 64 23.1 Mild/Little need 87 31.4 Moderate/borderline need 65 23.5 Severe need 51 18.4 Extreme need 10 3.6 Total 277 100 22% Prevalens av sugvanor 3 år: 66% 7 år: 4% 11.5 år: <1% Sugvanors påverkan på bettet FALLFALL 1 1 Ett signifikant samband fanns mellan sugvanor och frontalt öppet bett, korsbett, stor horisontell överbitning och klass II relation vid 3 års ålder Sugvanors påverkan på bettet FALLFALL 1 1 Ett signifikant samband fanns mellan sugvanor och frontalt öppet bett samt korsbett vid 7 års ålder Sugvanors påverkan på bettet FALLFALL 1 1 Vid 11.5 år - inga samband med de bettavvikelser som förekom och sugvana vid 3 års ålder Tandtrauma 30% av barnen vid 11.5 års ålder hade upplevt ett tandtrauma Det var vanligare med tandtrauma om man hade ett överbett på mer än 4 mm, OR = 2.2 Inkompetent läppslut ökade risken ytterligare för tandtrauma, OR = 3.1 Konklusioner Prevalensen av bettavvikelser i det primära och permanenta bettet var 70% Självkorrigering förekom för alla bettavvikelser men även utveckling av nya sågs ökad förståelse för bettutvecklingen i tidig ålder - vissa behandlingar kan vara onödiga innan växelbettsperioden då självkorrigering är vanligt förekommande Risken för tandtrauma är förhöjd vid överbett mer än 4 mm och ofullständigt läppslut The impact of malocclusions on the quality of life among children and adolescents a systematic review of quantitative studies Dimberg L, Arnrup K, Bondemark L BAKGRUND Det är rimligt att anta att: för barn och ungdomar med obehandlade bettavvikelser kan barnets/ungdomens munhälsorelaterade livskvalitet påverkas SYFTE • En systematisk genomgång av litteraturen för att undersöka om belägg finns för att bettavvikelser har inverkan på den munhälsorelaterade livskvaliteten hos barn och ungdomar MATERIAL OCH METOD En systematisk genomgång gjordes av litteraturen enligt Goodman's modell som innehåller 4 steg 1. Frågeställning Har bettavvikelser betydelse för den munhälsorelaterade livskvaliteten hos barn och ungdomar? 2. Sökstrategi Litteratursökning i 5 databaser fram till och med Januari 2014 • PubMed • Cochrane Library • CINAHL • PSYCHINFO • EMBASE • Söksyntax: “quality of life” [MeSH term] OR “self concept” [MeSH term] OR “patient satisfaction” [MeSH term] OR “personal satisfaction” [MeSH term] OR “well being” [text word] OR “wellbeing” [text word] AND “malocclusion” [MeSH term] OR “orthodontics” [MeSH term] OR “dental esthetics” [MeSH term]. 3. Urval av artiklar Inklusionskriterier: Kontrollerade eller subgruppering enligt bettavvikelse/ej bettavvikelse alt behov/ej behov Bettavvikelser och/ eller ortodontiskt behandlingsbehov mätt av professionen med hjälp av standardiserad metod Självskattad munhälsorelaterad livskvalitet med validerat mätinstrument Fulltextartiklar skrivna på engelska eller skandinaviskt språk Studierna ska beröra barn och ungdomar Urval av artiklar 3. Urval av artiklar • Urval och bedömning av kvalitet gjordes utav 3 personer oberoende av varandra • En artikel beställdes i fulltext om åtminstone en av tre ansåg den relevant • Ett protokoll upprättat utifrån inklusionskriterierna användes • Referenslistorna av utvalda artiklar genomsöktes manuellt Kvalitetsbedömning – hög kvalitet • • • • Tillräckligt stort material Relevant subgruppering Redovisning av bortfall – < 30 % Kontroll av viktiga confounders; karies, socioekonomiska faktorer, ålder och kön Om ett kriterium ovan saknades – nedgradering till moderat kvalitet, två eller fler saknades – nedgradering till låg kvalitet 4. Bedömning av evidens • Den totala evidensen fastställs utifrån samtliga bedömda studier • Klassifiering som otillräcklig; låg; moderat eller hög enligt GRADES riktlinjer och av de tre bedömarna oberoende av varandra (Guyatt et al 2011) RESULTAT Identification 1142 records after duplicates removed 1072 records excluded - not following the objective of the review (908) - cleft lip/palate syndromes or severe illness (85) - quality of life measured during orthodontic treatment (14) - studies of psychometric properties (24) - language (13) - letters (28) Screening 1142 records screened by reviewing titles and abstracts 48 full-text articles excluded Eligibility 70 records screened by reviewing the full-text articles 22 full-text articles met the eligibility criteria - not following the objective of the review (31) no control or subgroup categorization (10) inadequate data on quality of life (4) inadequate definition of malocclusions (3) 16 full-text articles excluded - study of low quality (16) Included 0 articles found via manual search of reference lists 6 articles included in the evaluation of evidence KOMPLETTERANDE SÖKNING • Förnyad sökning för perioden Januari till September 2014 och med samma söksyntax, inklusionskriterier, datainsamling och analyser som innan • Sökningen gav ytterligare 176 titlar och abstracts men endast 2 motsvarade inklusionskriterierna RESULTAT • 22 studier inkluderades i den fullständiga analysen • 16 av 22 studier var av låg kvalitet och uteslöts då dessa inte kan bidra till den totala evidensen • De kvarvarande 6 studierna var av tvärsnittsdesign och 4 studier var av hög kvalitet och 2 av medium kvalitet • Kompletterade sökningen gav 1 studie med hög kvalitet och 1 med moderat kvalitet • TOTALT: 8 studier som kan vara grund till evidens Fyra studier med hög kvalitet rapporterade att anterior trångställning, glesställning eller stort överbett hade negativ inverkan på livskvaliteten Malocclusion and oral health-related quality of life in Brazilian school children. Sardenberg, F., Martins, M.T., Bendo, C.B., Pordeus, I.A., Paiva, S.M., Auad, S.M. and Vale, M. P. (2013) Angle Orthodontist, 83, 83-89. Malocclusion impacts adolescents' oral health-related quality of life. Scapini, A., Feldens, C.A., Ardenghi, T.M. and Kramer, P.F. (2013) Angle Orthodontist, 83, 512-518. Impact of malocclusion on quality of life among New Zealand adolescents. Ukra, A., Foster Page, L.A., Thomson, W.M., Farella, M., Tawse Smith, A. and Beck, V. (2013) New Zealand Dental Journal, 109, 18-23. Social and dental status along the life course and oral health impacts in adolescents: a population-based birth cohort. Peres, K.G., Peres, M.A., Araujo, C.L., Menezes, A.M. and Hallal, P.C. (2009) Health and Quality of Life Outcomes, 7, 95. En studie med moderat/medelhög kvalitet rapporterade att munhälsorelaterad livskvalitet var influerad av psykologiska men också kliniska variabler såsom extremt uttalad bettavvikelse i jämförelse med mildare bettavvikelser Oral health-related quality of life of schoolchildren: impact of clinical and psychosocial variables. Schuch HS, Dos Santos Costa F, Torriani DD, Demarco FF Gottems ML. (2014) Int J Paediatr Dentistry, Jul 22. doi: 10.1111/ipd.12118. Två studier med moderat/medelhög kvalitet rapporterade att ett förhöjt ortodontiskt behandlingsbehov hade negativ inverkan på livskvaliteten The influence of oral health conditions, socioeconomic status and home environment factors on schoolchildren's self-perception of quality of life. Paula, J.S., Leite, I.C., Almeida, A.B., Ambrosano, G.M., Pereira, A.C. and Mialhe, F.L. (2012) Health and Quality of Life Outcomes, 10, 6. Oral health-related quality of life and orthodontic treatment seeking. Feu, D., de Oliveira, B.H., de Oliveira Almeida, M.A., Kiyak, H.A. and Miguel, J.A. (2010) American Journal of Orthodontics and Dentofacial Orthopedics, 138, 152-159. En studie med hög kvalitet rapporterade att individuella faktorer särskilt känslan av att tillhöra ett sammanhang var betydelsefullt medan bettavvikelser, gingival hälsa eller emalj-opaciteter inte var relaterade till den munhälsorelaterade livskvaliteten Determinant's of children's oral-health-related quality of life over time. Gururatana O, Baker SR, Robinsson PG. Community Dent Oral Epidemiol 2014;42(3): 206-15 1 H Malocklusioner påverkar inte Qol 3 M 4H Malocklusion påverkar negativt Qol Således vid sammanlagd viktning av de 8 olika studierna blir resultatet hög evidens för att synliga bettavvikelser har negativ inverkan på livskvaliteten, dvs 7 mot 1 studie RESULTAT Brasilien Scapini et al 2013 (H) Sardenberg et al 2013 (H) Paula et al 2012 (M) Feu et al 2010 (M) Peres et al 2009 (H) Schuch et al 2014 (M) Thailand Gururatana et al 2014 (H) Nya Zeeland Ukra et al 2013 (H) Konklusioner starkt stöd för att bettavvikelser i den estetiska zonen har betydelse för livskvaliteten hos barn och ungdomar spridningen av studier med hög kvalitet som berör bettavvikelsers betydelse för livskvaliteten är begränsad och innebär att fler studier från Europa och inte minst Sverige behövs DELARBETE V I. Prevalence of malocclusion traits and sucking habits among 3-year old children. Dimberg L, Bondemark L, Söderfeldt B, Lennartsson B. Swed Dent J 2010;34:35-42. II. Malocclusions in children at 3 and 7 years of age: a longitudinal study. Dimberg L, Lennartsson B, Söderfeldt B, Bondemark L. Eur J Orthod 2013;35:131-37. III. Prevalence and change of malocclusions from primary to early permanent dentition – a longitudinal study. Dimberg L, Lennartsson B, Arnrup K, Bondemark L. Accepted for publication in Angle Orthodontist. IV. The impact of malocclusion on the quality of life among children and adolescents: a systematic review of quantitative studies. Dimberg L, Arnrup K, Bondemark L. Eur J Orthod 2014; doi:10.1093/ejo/cju046. V. Oral health related quality of life among children – The impact from malocclusions. Dimberg L, Lennartsson B, Bondemark L, Arnrup K. Submitted. SYFTE • Beskriva den munhälsorelaterade livskvaliteten i en kohort med barn vid 11.5 års ålder inom den svenska tandvården • Utvärdera betydelsen av bettavvikelser eller ortodontiskt behandlingsbehov för den munhälsorelaterade livskvaliteten med hänsyn tagen till kön, socioekonomiska faktorer, tandvårdsrädsla samt olika aspekter av munhälsa TACK FÖR UPPMÄRKSAMHETEN! METODER • Anamnesintervju: Trauma, huvudvärk, socioekonomiska faktorer • Statusregistrering: Bettavvikelser, karies (DMFS), emaljskador, tandregleringsbehov (IOTN) Enkäter: Livskvalitet mättes med Child Perceptions Questionnaire Impact Short Form (CPQ11-14 ISF:16) • Tandvårdsrädsla mättes med Children´s Fear Survey Schedule - Dental Subscale (CFSS-DS) Confounders - förväxlingsfaktorer • • • • • • Tandvårdsrädsla (CFSS-DS score) Karies (DMFS) Emaljskador (ja/nej) Tandtrauma (ja/nej) Huvudvärk (ja/nej) Socioekonomiska faktorer (föräldrars utbildningsnivå och sysselsättning samt om barnen bodde tillsammans med båda föräldrarna eller ej) RESULTAT 257 barn: 121 pojkar och 136 flickor, deltog Livskvalitetsenkät CPQ – maxscore i vår studie: 33 (0-64) Medelvärde i vår studie: 9 Medianvärde i vår studie: 8 Totalt lågt CPQ total score = Hög livskvalitet i gruppen RESULTAT Cohorten med barn visade en god munhälsorelaterad livskvalitet Betydelsen av bettavvikelser eller ortodontiskt behandlingsbehov för livskvaliteten var begränsad och inkonsekvent Tandvårdsrädsla och huvudvärk var tydligare påverkansfaktorer än bettavvikelser eller ortodontiskt behandlingsbehov KONKLUSIONER tandvårdsrädsla och huvudvärk kan ha större betydelse för livskvaliteten än bettavvikelser och ortodontiskt behandlingsbehov innan barnen kommit in i tonårsperioden en viktig insikt för tandläkaren när man ska bedöma lämplig tidpunkt för start av tandregleringsbehandling så att man hamnar rätt i tiden när det gäller inställning och motivation till behandling hos barnet Posterior or anterior crossbite – is early treatment effective and stable in the long-term? Early versus late treatment • Subject of controversy in orthodontics and often confusing + + + + + + Desirable in special situations Easy to perform Diminish the extent of treatment in the permanent dentition Increases the patient´s self-esteem Improved control of growth Less damage to teeth and tissues Less damage to the teeth/tissues and diminish the extent of treatment Extraction 63 Control after 6 months Less damage to the teeth and tissues – increase the patient´s self-esteem Providing early orthodontic treatment for children with prominent upper front teeth is more effective in reducing the incidence of incisal trauma than providing one course of orthodontic treatment when the child is in early adolescence. Thiruvenkatachari B, Harrison JE, Worthington HV, O’Brien KD. Orthodontic treatment for prominent upper front teeth (Class II malocclusion) in children. Cochrane Database Syst Rev 2013; 11: Art. No.: CD003452. DOI: 10.1002/14651858.CD003452.pub3. Less damage to the teeth and tissues – increase the patient´s self-esteem Over two hundred million injuries to anterior teeth attributable to large overjet: a meta analysis Petti S. Dental Traumatology 2015;31:1-8 Improved control of growth – diminish the extent of treatment • it is claimed that untreated unilateral posterior crossbite may result in facial asymmetry – deviating the mandible to the crossbite side (Pinto et al, 2001; Kecik et al, 2007) • it is also claimed that functional crossbite can progress to a skeletal malocclusion – implying extensive orthodontic and surgical treatment Desirable in special situations – less damage Desirable in special situations – less damage After 4 months of treatment Less damage to the teeth and tissues Less damage to the teeth and tissues – wear of maxillary incisors Early treatment There are several reasons to treat early, but… - is early treatment effective ? - is early treatment stable ? Early treatment - posterior crossbite From an evidence based point of view, the effectiveness of posterior crossbite correction in the mixed dentition is rather well evaluated Petrén S, Bondemark L, Söderfeldt B. A systematic review concerning early orthodontic treatment of unilateral posterior crossbite. Angle Orthod 2003;73:588596. Harrison JE, Ashby D. Orthodontic treatment for posterior cross-bites (Cochrane Review) In: The Cochrane Library, Issue 4, 2001. Oxford: Update Software Early treatment - posterior crossbite From an evidence based point of view, the effectiveness of posterior crossbite correction in the mixed dentition is rather well evaluated Petrén S, Bondemark L, Söderfeldt B. A systematic review concerning early orthodontic treatment of unilateral posterior crossbite. Angle Orthod 2003;73:588596. Harrison JE, Ashby D. Orthodontic treatment for posterior cross-bites (Cochrane Review) In: The Cochrane Library, Issue 4, 2001. Oxford: Update Software Early treatment - posterior crossbite From an evidence based point of view, the effectiveness of posterior crossbite correction in the mixed dentition is rather well evaluated Petrén S, Bondemark L, Söderfeldt B. A systematic review concerning early orthodontic treatment of unilateral posterior crossbite. Angle Orthod 2003;73:588596. Harrison JE, Ashby D. Orthodontic treatment for posterior cross-bites (Cochrane Review) In: The Cochrane Library, Issue 4, 2001. Oxford: Update Software Aim In the mixed dentition determine the costs of correcting posterior crossbites with Quad Helix or expansion plates and to relate the costs to the effects after treatment and 3 years post retention • Petrén S, Bjerklin K, Bondemark L. Stability of unilateral posterior crossbite correction in the mixed dentition: a randomized clinical trial with a 3-year follow-up. Am J Orthod Dentofacial Orthop. 2011;139:e73-81 • Petrén S, Bjerklin K, Marké LÅ, Bondemark L. Early correction of posterior crossbite – a cost-minimization analysis. Eur J Orthod 2013;35:14-21 Inclusion criteria - mixed dentition (8-9 years) Inclusion criteria - mixed dentition (8-9 years) - unilateral posterior crossbite including the 1st permanent molar - no sucking habits - no previous orthodontic treatment Randomized patients N = 40 Allocated to Quad helix N = 20 Allocated to Expansion plate N = 20 Quad helix • bands on maxillary first molars and a lingual arch with four helix (loops) • activation 10 mm before insertion and then, when necessary, reactivated every 6 weeks until normal transverse relationship is achieved • to prevent or compensate for buccal tipping, the appliance is adjusted for buccal root torque • retention with the current appliance for 6 months Expansion plate • made of acrylic with an expansion screw and clasps on the first primary and permanent molars • activation of the screw 0.2 mm once a week until normal transverse relationship is achieved • the patient is instructed to wear the plate night and day, except for meals and tooth brushing (22 hrs/day) • retention with the current appliance for 6 months Methods Five experienced practitioners treated the patients according to a preset standard concept and under the supervision of specialist orthodontists Registrations - outcomes - success rate of crossbite correction - treatment time - maxillary expansion - cost-effectiveness What is considered ”successful treatment”? Normal transverse relation achieved within one year and at the 3-year follow-up Study models on: Crossbite patients before treatment… T0 Age: 8-9 years …after treatment… T1 Age: 9-10 years …at follow-up (3 yrs post retention) T2 Age: 12-13 years Results – success rate after active treatment (T1) Quad Helix: 20 / 20 Expansion plate: 15 / 20 P = 0.045 Treatment time (months) T0 – T1 Appliance Mean SD Quad Helix 4.8 3.52 Expansion plate 9.6 3.04 P=0.0004 Results – long-term stability 3 years post retention (T2) Quad Helix: 19 of 20 patients stable Expansion plate: 15 of 15 patients stable No significant difference between the groups! Transversal width at T2 Patient age: 12-13 years at the 3-year follow-up QH Mean EP SD (mm) mean Sign. NG SD (mm) mean SD (mm) Upper molar width at gingival margin 32,5 2,67 32,5 2,20 35,6 2,60 NG>QH** NG>EP** Upper molar width at mb cusp tip 50,5 2,89 50,1 2,61 52,4 2,22 NG>QH* NG>EP* Upper canine width at gingival margin 23,0 1,84 23,5 2,12 24,8 2,02 NG>QH* Upper canine width at cusp tip 32,5 2,52 32,7 1,65 34,2 1,99 NG>QH* The width of the maxilla in the former crossbite patients never reached that of the normal control subjects Conclusions - for correction of posterior crossbite, Quad-helix offers significant higher success rate over expansion plate treatment - both Quad-helix and expansion plate treatment show good long-term stability - the width of the maxilla in the former crossbite patients never reached that of the normal control subjects Evidence-based evaluation Cornerstones: - effectiveness and long-term effects - cost-effectiveness - patients perception of pain and discomfort Cost analysis • four types of evaluations can be used to gather evidence and compare the expected costs and consequences of different procedures: - cost-effectiveness analysis - cost-minimization analysis - cost-utility analysis - cost-benefit analysis Michael F Drummond, 2005 Cost-minimization analysis • a form of cost-effectiveness analysis • the outcomes of the treatment alternatives have to be identical • e.g. crossbite will be corrected irrespective of which treatment is applied • the costs of each intervention are assessed • the least costly method can be identified Cost-minimization analysis To identify which alternative has the lowest cost: - after treatment and 3 years post retention - all costs were based on 2010 prices Outcome measures Societal costs = direct + indirect costs for: - successful treatments alone - successful and unsuccessful treatment including re-treatment when required Direct costs Staff costs for dentists, dental assistants, dental office Cleaning Laboratory fees and materials Material costs such as impression material, orthodontic bands, orthodontic cement Indirect costs - loss of income (wages + social security costs) incurred by the patients’ parents, assuming that they were absent from work to accompany the patient to the orthodontic appointment Indirect costs - the absence from work was estimated at 90 minutes per appointment, i.e. 30 minutes for the appointment and 60 minutes’ travelling time for parent and child from work and school to the dental clinic - the wages of an average Swedish worker: €30 / h Societal costs = direct + indirect costs per patient/treatment Successful treatments alone QH All treatments including re-treatments Societal costs € 996 € 1047 Direct costs € 598 € 628 Indirect costs € 398 € 419 P < 0.05 Successful treatments alone P < 0.01 All treatments including re-treatments EP Societal costs Direct costs Indirect costs € 1141 € 1417 € 655 € 486 € 813 € 604 Indirect costs at least 30% of societal costs Successful treatments alone QH All treatments including re-treatments Societal costs € 996 € 1047 Direct costs € 598 € 628 Indirect costs € 398 € 419 P < 0.05 Successful treatments alone P < 0.01 All treatments including re-treatments EP Societal costs € 1141 € 1417 Direct costs € 655 € 486 € 813 € 604 Indirect costs Conclusions - for correction of posterior crossbite, Quad-helix offers significant economic benefits over expansion plate treatment - the Quad-helix had lower direct and indirect costs and fewer failures needing re-treatment - even with full co-operation, i.e. when only successful treatments were considered, treatment with expansion plate was more expensive than with Quad-helix ”White Spot Lesions (WSL) vid ortodontisk behandling - Hur undviker vi det?” VILKA ALTERNATIV ERBJUDS? Varnish Miswaks Tandkräm Fluortabletter Munsköljmedel Mjölk med fluor Fluor i bondingmaterial High fluoride toothpaste and White Spot Lesions (WSL) - a Randomized Controlled Trial in adolescents with fixed orthodontic appliance Lars Bondemark, professor, Malmö Sonesson et al., Eur. J. Ortho. 2014 Svante Twetman, professor, Copenhagen Mikael Sonesson, lektor, Malmö Medverkande Susanne Andersson, Krister Bjerklin, Lars Bondemark, Ingrid Carlin, Pia Jensen, Gunilla Jeppsson, Annelie Johansson, Elisabeth Kaiser, Ingela Karlsson, Lars-Göran Lindström, Birgitta Magnusson, Karin Nerbring, Marie Nilsson, Stefan Norén, Marie Rosenlind, Mikael Sonesson, Marita Svensson, Annette Timén, Svante Twetman, Jessica Willén • • • • • Jönköping Värnamo Nässjö Malmö Copenhagen SYFTE Att på ungdomar som behandlas med fast tandställning utvärdera den kariesförebyggande effekten av en tandkräm som innehåller hög fluorhalt och jämföra med tandkräm som innehåller normal koncentration av fluor STUDIEDESIGN • • • • • multicenter RCT med två parallella armar WSL enligt en 4-gradig skala är primärt utfallsmått WSL före och efter behandling med fast apparatur poweranalys - minst 172 patienter per grupp studien godkänd av Regionala etikprövningsnämnden i Lund, (Dnr 417/2007) MATERIAL • 482 konsekutiva patienter, 11-17 år • remitterade till specialistklinikerna för tandreglering i Jönköping, Malmö, Nässjö, Värnamo och TVH, Malmö • fast apparatur (SWA MBT .022) i båda käkarna • planerad behandlingstid - minst 1 år • funktionshindrade patienter som inte själva klarar av sin munhygien utesluts KLINISK PROCEDUR • testgruppen (A) får tandkräm med 5000 ppm fluor (Duraphat®, Colgate-Palmolive, Glostrup, Denmark) • kontrollgruppen (B) får tandkräm med 1450 ppm fluor (Duraphat®, Colgate-Palmolive, Glostrup, Denmark) KLINISK PROCEDUR • alla instrueras att använda en 2 cm lång sträng tandkräm för att borsta tänderna under minst 2 minuter morgon och kväll • alla får två tuber tandkräm vid ”baseline” och sedan var 3:e månad KLINISK PROCEDUR professionell rengöring med fluorfri pasta 3 intraorala foton av incisiver, caniner och premolarer bond för full fast apparatur ök/uk i minst 1 år avlägsnande av apparatur och bortputs av compositrester med långsamtgående karbidborr • professionell rengöring med fluorfri pasta • 3 intraorala foton • • • • REGISTRERING AV WSL Score 1 inga spår av WSL Score 2 tunn rand Score 3 tjockt band Score 4 med kavitet Gorelick et al, 1982 Gorelick et al, 1982 WSL registrering Score 1 inga spår av WSL WSL registrering Score 2 tunn rand WSL registrering Score 3 tjockt band WSL registrering Score 4 med kavitet MÄTPROCEDUR • • • • digitala foton bilder före och efter behandling analyseras på datorskärm i mörkt rum två vana och kalibrerade observatörer observatörerna är inte involverade i behandlingarna MÄTPROCEDUR • • • blindad analys – omedvetna om vilken grupp patienterna tillhör oskarpa foton utgår (bortfall) 50 slumpmässigt utvalda fall upprepas för analys för att bestämma intra- och interindividuell variation av bedömningarna STATISTISKA METODER • Chi2-test med Yates korrektion för kategoriska data • ANOVA med Tukey´s post-hoc test för att detektera gruppskillnader av numeriska data • signifikansnivå 5% (p<0.05) • Cohen´s kappa för att bestämma intra- och interindividuell variation av bedömningarna RESULTAT • intra-individuell variation: kappa 0.698 och 0.800 (bra – mycket bra) • inter-individuell variation: kappa 0.744 (bra) 482 eligible patients 58 no consent 424 enrolled and randomized patients 211 allocated to test toothpaste (5.000 ppm) 213 allocated to reference toothpaste (1.450 ppm) 21 23 drop-outs drop-outs -10 did not comply -7 relocated -6 missing or poor photos - 8 did not comply - 3 relocated - 10 missing or poor photos 188 available at debonding 192 available at debonding Resultat Ålder start (år) medel Test 14.8 Kontroll 14.6 SD 1.70 1.65 range 11.2 - 19.0 11.0 - 19.0 NS Behandlingslängd (år) medel Test 1.8 Kontroll 1.9 SD 0.51 0.55 range 1.0 - 3.0 1.0 - 3.0 NS Resultat Prevalens WSL (%, individ nivå) WST Test (n = 188) Kontroll (n = 192) P Test/Ref. Start 16.5 18.7 0.66 Debond 34.6 45.3 0.04 Resultat WSL (yta) – debond Score Test Kontroll 1 1511 88.3 % 1483 86.7 % 2 180 10.5 % 188 11.0 % 3 19 1.1 % 39 2.3 % 4 1 0.06 % 0 0.00% Resultat WSL (yta) – debond Score Test Kontroll 1 1511 88.3 % 1483 86.7 % 2 180 10.5 % 188 11.0 % 3 19 1.1 % 39 2.3 % 4 1 0.06 % 0 0.00% Resultat WSL, tandtyp Premolar Canine Lateral Central Total Test 29 32 49 24 134 Kontroll 31 36 64 23 154 Resultat WSL, tandtyp Premolar Canine Lateral Central Total Test 29 32 49 24 134 Kontroll 31 36 64 23 154 DISKUSSION - STYRKA • • • • • studiedesign – RCT stort material – litet bortfall bedömare inte involverade i behandlingen bedömare omedvetna om vilken grupp man granskar bra Kappa-värden – liten intra- och interindividuell variation vid bedömning DISKUSSION - SVAGHETER • granskning på foton • hellre ”fria än fälla” då oklart vilken score det är fråga om – underdiagnostik KONKLUSIONER Vid behandling med fast tandställning, och för att förebygga WSL, är det mer effektivt att dagligen använda hög- än normalkoncentrerad fluortandkräm KONKLUSIONER Högkoncentrerad fluortandkräm resulterar i: - Färre WSL på individnivå - Färre grava WSL - Lateralen är den tand som oftast drabbas av WSL oavsett vilken fluormängd som tillförs STUDIEN HAR FÅTT FINANSIELLT STÖD FRÅN • Stiftelsen Patentmedelsfonden för Odontologisk Profylaxforskning • Collgate donerade tandkräm Nytt forskningsprojekt VAD ÄR EVIDENSEN FÖR OLIKA METODER ATT UNDVIKA WSL? • "Enligt den senaste Cochrane uppdateringen, visst underlag för att fluorlack kan minska risken för att utveckla emaljkaries runt brackets vid behandling med fast apparatur, men bevisvärdet bedöms som måttligt då antalet relevanta studier var litet. Man efterlyste fler randomiserade kontrollerade kliniska studier för att få ett säkrare vetenskapligt underlag och det är en sådan som nu genomförs". Benson PE et al. Cochrane Database Syst Rev. 2013 Dec 12; 12:CD003809. Epub 2013 Dec 12. “Efficacy of a novel fluoride varnish formula in preventing white spot lesions during treatment with fixed orthodontic appliances” Medverkande Salem Asad, Ingrid Carlin, Lars Bondemark, Mikael Sonesson, Karin Nerbring, avdelningen för ortodonti, Malmö högskola, Malmö Helsingborg Hässleholm Köpenhamn Malmö Anna Brechter, Mats Bernhold, Karin Lindestam, Carina Svensson, Ulla Bertilsson, Margareta Persson, Anna Lönnberg, Bernhold Ortodonti, Helsingborg Rolf Lindman, Petter Lindahl, Ortodonti Syd, Hässleholm Svante Twetman, Köpenhamns Universitet, Köpenhamn SYFTE utvärdera den kariesförebyggande effekten av ett fluorlack innehållande ammonium fluorid (AmF) och jämföra med ett placebolack hos ungdomar som behandlas med fast tandställning STUDIEDESIGN • Dubbel-blindad randomiserad kontrollerad multicenter studie (RCT), två parallella armar • Behandlas vid tre specialistkliniker för tandreglering i Helsingborg, Hässleholm och odontologiska fakulteten i Malmö. • WSL före och efter behandling med fast apparatur • Studien godkänd av Regionala etikprövningsnämnden i Lund (Dnr 2014/183) MATERIAL • • • • Power-analys - minst 85 patienter per grupp 190 konsekutiva patienter, 11-18 år Fast apparatur (SWA MBT .022) i båda käkarna Planerad behandlingstid - minst 1 år KLINISK PROCEDUR • grupp A (test) vid ordinarie återbesök var sjätte vecka, fluorlack med 7,700 ppm ammonium fluorid (AmF) applicerat runt tandställningsfästena i överkäken. Borstar som vanligt hemma • grupp B (placebo) också vid ordinarie återbesök var sjätte vecka, fluorlack med samma komponenter som i testgruppens lack, utan ammonium fluorid (AmF). Borstar som vanligt hemma Undersökningsvariabler • Utfallsmåtten är incidens och svårighetsgrad av karies (WSL), registrerade på digitala foton enligt Gorelicks index 1 2 3 4 Gorelick et al, 1982 VILKEN VÄG KAN VI VÄLJA RESULTAT? FÖR ATT UNDVIKA WHITE SPOT LEASION (WSL)? SÅ… I dagsläget: Begränsat vetenskapligt underlag för att: - daglig användning av tandkräm med hög fluorkoncentration, reducerar WSL Måttligt vetenskapligt underlag för att: - kontinuerlig applicering av varnish, reducerar risken för WSL i samband med ortodontisk behandling Treatment of functional anterior crossbite – evidence-based evaluations of treatment effects, cost-effectiveness and patients´ perceptions Background • anterior crossbite with functional shift, i.e. inter-incisal contact is possible when the mandible is in the centric relation (pseudo Class III) Early treatment - anterior crossbite • more than 12 methods for correcting anterior crossbite affecting one or more incisors (Systematic review - Borrie and Bearn, 2011) • the best level of evidence currently available is from retrospective studies, which advocate use of fixed appliance (Systematic review - Borrie and Bearn, 2011) • there is need of high quality clinical trials to identify the most effective treatment for anterior crossbite (Systematic review - Borrie and Bearn, 2011) Aims • to compare the effectiveness between fixed and removable orthodontic appliances after treatment of anterior crossbite with functional shift in the mixed dentition (Wiedel and Bondemark, Eur J Orthod 2014) • to evaluate the stability 2 years post retention (Wiedel and Bondemark, Angle Orthod 2014) • to evaluate and compare the costs of correcting anterior crossbite with fixed or removable appliances using cost-minimization analysis (Wiedel and Bondemark, Eur J Orthod 2015) • to analyze patients’ perceptions of fixed and removable appliance therapy with special reference to perceived pain, discomfort and impairment of jaw function vs Inclusion criteria • healthy patients with no previous orthodontic treatment • early to late mixed dentition • anterior crossbite with functional shift affecting one or more incisors • ANB angle >0o • moderate space deficiency in the maxilla (up to 4 mm) • nonextraction treatment plan Removable appliance • • • • • • acrylic palatal plate protrusion springs bilateral occlusal coverage of the posterior teeth activation of the springs every 4 weeks instruction to use the appliance 22h/day the occlusal coverage removed as soon as the anterior crossbite was corrected • 3 months retention with inactive appliance and without the lateral occlusal splints Fixed appliance • 8-10 bonded brackets (.022 SWA) to incisors and deciduous canines and molars • archwire sequence: .016 HANT, .019x.025 HANT and .019x.025 ss • to prevent vertical interlock between the maxillary and mandibular incisors composite was bonded to occlusal surfaces of both the mandibular second deciduous molars • progress evaluated every 4 weeks • 3 months retention with the fixed appliance serving as a passive retainer Main outcome measures • success rate of anterior crossbite correction (yes/no) • treatment time in months, from insertion to date of appliance removal • overjet and overbite in millimeters • arch length in millimeters • cost measures - direct + indirect costs = societal costs • 26 questions for self-reporting regarding pain, discomfort and functional jaw impairment 64 eligible children with anterior crossbite Declined to enter the study (N = 2) Randomized children with anterior crossbite (N = 62) Failure to comply (N = 1) Allocated to treatment with removable appliance (N = 31) Allocated to treatment with fixed appliance (N = 31) Outcome analysis and completed treatment (N = 30) Outcome analysis and completed treatment (N = 31) Results – after treatment Removable Fixed appliance appliance (n = 31) Success rate 30/31 Mean treatment time (months) 6.9 (n = 31) 31/31 N.S. 5.5 <0.05 Discussion • in this study higher success rate of removable appliance compared to the removable expansion plate for correction of posterior crossbite • conceivably, patients with anterior crossbite are more aware of their malocclusion, unlike posterior crossbite Results 2 years post retention 64 eligible children with anterior crossbite Declined to enter the study (N = 2) Randomized children with anterior crossbite (N = 62) Failure to comply (N = 1) Relapse (N = 1) Not reachable (N = 2) Allocated to treatment with removable appliance (N = 31) Allocated to treatment with fixed appliance (N = 31) Outcome analysis and completed treatment (N = 30) Outcome analysis and completed treatment (N = 31) Analyzed and completed 2 years follow-up (N = 27) Analyzed and completed 2 years follow-up (N = 29) Relapse (N = 1) Not reachable (N = 1) Results – 2 years post retention Removable appliance (n = 31) Success rate 27/31 Fixed appliance (n = 31) 29/31 N.S. Conclusions • 2 years post retention almost all subjects had good Class I occlusion with normal overjet/overbite and with no functional shift • the transition to the permanent dentition had occurred in most of the subjects in both groups • the prognosis was favourable for the post retention results to be stable in the future • either type of appliance can be recommended Cost-minimization analysis To identify which treatment alternative has the lowest cost: - after treatment and 2 years post retention vs - all costs were based on the Consumer Price Index for 2013 Wiedel AP, Norlund A, Petrén S, Bondemark L. Eur J Orthod. 2015 March. In press. Outcome measures Societal costs = direct + indirect costs for: - successful treatments alone - successful and unsuccessful treatment including re-treatment when required Mean societal costs, direct costs of materials, direct costs for treatment time and indirect costs in Euros. Successful patients only. Fixed appliance (FA) n=31, removable appliance (RA) n=30 FA Mean 630 32 323 275 SD RA Mean SD 198 3 102 101 945 227 371 346 302 79 135 104 Group difference p-value Successful patients only Societal costs Direct costs – material Direct costs – treatment time Indirect costs NS = not significant 0.000 0.000 N.S. 0.006 Including re-treatment - mean societal costs, direct costs of materials, direct costs for treatment time and indirect costs in Euros. Fixed appliance (FA) n=33, removable appliance (RA) n=33 FA Mean 678 35 351 293 SD RA Mean SD 361 15 197 153 1031 231 417 383 511 82 262 200 Group difference p-value Including re-treatment Societal costs Direct costs – material Direct costs – treatment time Indirect costs 0.000 0.000 N.S. 0.008 NS = not significant Conclusions - the analysis disclosed significant economic benefits for fixed over removable appliance - even when only successful outcomes were assessed, treatment with RA was more expensive Smärta och obehag? Pain and discomfort • 95 % of patients report pain during orthodontic treatment - Bergius et al. J Orofac Orthop 2000;61:125-37 - Krishnan V. Eur J Orthod;29:170-9 Aims • to compare the effectiveness between fixed and removable orthodontic appliances after treatment of anterior crossbite with functional shift in the mixed dentition (Wiedel and Bondemark, Eur J Orthod 2014) • to evaluate the stability 2 years post retention • to evaluate and compare the costs of correcting anterior crossbite with fixed or removable appliances using cost-minimization analysis (Wiedel and Bondemark, Eur J (Wiedel and Bondemark, Angle Orthod 2014) Orthod 2015) • to analyze patients’ perceptions of fixed and removable appliance therapy with special reference to perceived pain, discomfort and impairment of jaw function vs Methods • the assessment included self-report questions, from a previous study, in which reliability and face validity of the questions found to be acceptable Feldmann I, List T, Feldmann H, Bondemark L. Angle Orthod 2007;77:578-85 • evaluations of pain and discomfort (VAS), analgesic consumption, limitations in daily activities, and functional jaw impairment (4-point scale) Results vs • pain and discomfort intensity during the first 3 days were somewhat higher for the fixed appliance • pain and discomfort scores overall peaked on day two • adverse effects on school and leisure activities were reported more frequently in the removable than in the fixed appliance group • the fixed appliance group reported more difficulty eating different kinds of hard and soft food, while the removable appliance group experienced more speech difficulties • no significant intergroup difference was found for self-estimated disturbance of appearance between the appliances. Wiedel AP, Bondemark L. Angle Orthod. 2015 April. Submitted Day 0 Day 1 Day 2 Day 3 Day 4 Day 5 Day 6 Day 7 4 weeks 8 weeks VAS scale Removable appliance Fixed appliance Conclusions - the general levels of pain and discomfort were low to moderate in both groups - there were some statistically significant differences between the groups, but these were minor and deemed to be clinically unimportant - as both appliances were generally well accepted by the patients, either fixed or removable appliance therapy can be recommended vs Förankring - smärta och obehag? Orthodontic anchoring techniques and its influence on pain, discomfort and jaw function - a randomized controlled trial Feldmann I, List T, Bondemark L. Eur J Orthod. 2012;34:102-8 The article won the EJO Beni Solow award 2012 Aim during a standardized orthodontic treatment to evaluate and compare perceived pain, discomfort and limitation in daily life between orthodontic treatment combined with skeletal anchorage and treatment using conventional anchorage with headgear or transpalatal bar Subjects adolescents, 12-15 years of age permanent dentition Class I or II with severe crowding no previous experience of orthodontic treatment premolar extraction therapy in the maxilla followed by fixed appliances in both jaws • reinforced anchorage on the maxillary first molars considered necessary • • • • • Eligible patients N = 168 Denied to enter the trial N = 48 Randomized patients N = 120 60 Skeletal anchorage; 7 drop-outs: 30 Headgear; 30 Transpalatal bar Patients fullfilled the trial N = 113 Skeletal anchorage N = 54 1 moved (Skeletal) 1 poor oral hygiene (Skeletal) 1 serious ill (Transpalatal bar) 4 surgical failures (Skeletal) Headgear N = 30 Transpalatal bar N = 29 Conventional anchorage - headgear • straight pull • initial force - 400 g • the force was checked every sixth week Conventional anchorage – transpalatal bar • bands 16,26 • soldered stainless steel bar (2.0 x 1.0 mm) Osseointegrated anchorage – Orthosystem • Straumann, titanium implant 3.3 mm x 4 mm • 16 weeks healing period Osseointegrated anchorage – Orthosystem • Straumann, titanium implant 3.3 mm x 4 mm • 16 weeks healing period • bonded stainless steel bar (diameter 1.3 mm) Questionnaires to assess • • • • • pain intensity discomfort analgesic consumption limitations in daily activities functional jaw impairment Evaluations: • • • • • before treatment (base-line) during the first seven days in treatment after 6 weeks treatment after the leveling/aligning after the space-closure phase Daily activities • 3 questions with binary response (yes/no): “did you stay at home from school the last week because of pain from the appliance?” “did you refrain from your leisure activities the last week because of pain from the appliance?” “has your sleep been disturbed in the last week because of pain from the appliance?” Jaw function impairment • the scale includes 18 items related to jaw function: - 8 were related to mandibular function - 3 to psychosocial activities - 7 to eating specific foods • each item was assessed on a 4-point scale with the alternatives - not at all - slightly - much - extremely difficult Results: median values, interquartile ranges, and ranges concerning incisor pain intensity from base-line to the end of space-closure. Skeleta l a nchora ge group A Hea dgea r group B TPB group C 100 Pain intensity on VAS 80 60 40 20 0 A-C P= 0.033 Ba seline sep da y 1 da y 2 da y 3 da y 4 da y 5 da y 6 da y 7 6 w lev/a lign 8.2 months No significant difference in pain between the groups spa ce closure 17.4 months Pain level similar as before treatment Results: median values, interquartile ranges, and ranges concerning molar pain intensity from base-line to the end of space-closure. Skeleta l a nchora ge group A Hea dgea r group B TPB group C 100 Pain intensity on VAS 80 60 40 20 0 Ba seline sep A-C P= 0.09 A-C P= 0.046 B-C P= 0.049 A-C P= 0.025 A-C P= 0.012 da y 1 da y 2 da y 3 da y 4 Significant more pain in the transpalatal bar group A-C P= 0.013 da y 5 da y 6 da y 7 6 w lev/a lign 8.2 months spa ce closure 17.4 months Pain level similar as before treatment Results • significant higher pain scores from the palate and tongue in the skeletal and transpalatal bar groups compared to the headgear group • analgesic consumption followed the pain curve but no significant difference between the groups Results • throughout the trial period the limitation in daily life and jaw function impairment were low or negligible – no significant differences between the groups • gender differences were few – but between day 3 and 7, the girls complained significantly more about pain, discomfort and difficulty to eat hard food than the boys RCT: mini-screws vs conventional tooth supported anchorage RCT: mini-screws vs conventional tooth supported anchorage • adolescents, 12-15 years of age, with permanent dentition • no previous experience of orthodontic treatment • premolar extraction therapy in the maxilla followed by fixed appliances in both jaws • reinforced anchorage on the maxillary first molars considered necessary RCT: mini-screws vs conventional tooth supported anchorage In both groups: • extraction of premolars • leveling phase: a standard straight-wire concept (MBT, .022) with the arch-wire sequence: .016 HANT, .018 SS, .019 x .025 HANT Eligible patients N = 92 Randomized patients N = 80 Denied to participate N = 12 Allocated to miniscrews N = 40 Allocated to conventional anchorage N = 40 Extractions and registration 1 Extractions and registration 1 Fixed appliance and levelling, registration 2 Fixed appliance and levelling, registration 2 Miniscrews, space closure, registration 3 Tiebacks, space closure, registration 3 Space closure, ended registration 4 Space closure, ended registration 4 Fixed appliance removed, registration 5 Fixed appliance removed, registration 5 Post retention registration 6 Post retention registration 6 ”Utvärdering av olika användningstider för van Beek aktivatorn - En randomiserad kontrollerad studie” SAMARBETE ÖREBRO - MALMÖ Örebro Malmö Farhan Bazargani Odont. Dr., Centrum för Specialisttandvård, Avd. för Ortodonti, Örebro Mikael Sonesson Lektor, Avd. för Ortodonti; Malmö högskola Lars Bondemark Professor, Avd. för Ortodonti; Malmö högskola Fahad Alqabandi Internationell master, Avd. för Ortodonti; Malmö högskola Carita Strindberg Ortodonti assistent, Avd. för Ortodonti; Malmö högskola SYFTE • Undersöka samband användningstid och behandlingseffekt NOLLHYPOTES • Det är inte någon skillnad i behandlingseffekt mellan enbart nattanvändning och nattanvändning kombinerat med användning under kvällen (12 timmar) MATERIAL OCH METOD • Barn i växelbettet (8-10 år) med stort överbett • Folktandvårdens kliniker i Örebro samt Allmän Barn- och Ungdoms Tandvårdskliniken (ABUT), TVH, Malmö, erbjuds medverka • Runt 100 individer beräknas ingå MATERIAL OCH METOD Efter inlämnat samtycke kommer barnen att randomiseras (slumpas) i tre grupper: Grupp 1: Enbart nattetid Grupp 2: Kväll och natt (>12 timmar) Grupp 3: Ingen behandling (avvakta 18 mån.) MATERIAL OCH METOD • Samtliga Van Beek aktivatorer elektroniskt chip (TheraMon®) • Återbesök var 6-8:e vecka • Utvärdering efter 12 och 18 månader; undersökning, gipsmodeller, profilröntgen, extra – och intraorala foton • Blindat material vid mätningar • Utfallsmått; förmåga att sluta läpparna, reducerat överbett (mm), proflröntgen THERAMON® Sensor Van Beek aktivator THERAMON® VI HAR TESTAT ”CHIPET” I EN PILOTSTUDIE.. (TheraMon®) “COMPLIANCE DURING ORTHODONTIC TREATMENT WITH REMOVABLE APPLIANCES USING TWO TYPES OF REMINDERS, ASSESSED BY TIMER MODULES - A PILOT STUDY” Erik Frilund, Lisa Widegren Mikael Sonesson SYFTE Att undersöka om påminnelse med hjälp av mobiltelefon eller kalender påverkar användningstiden vid behandling med avtagbar apparatur MATERIAL OCH METOD • 18 patienter, avdelningen för ortodonti, MAH, • 9-14 års ålder • Patienterna placerades slumpmässigt i en av tre grupper; a) alarm; b) kalender; c) kontrollgrupp • Följdes mellan 65 och 120 dagar • Användningstid registrerades med TheraMon® Patients awaiting treatment with removable appliances agreeing to participate in study; n=18 Patients removed from study by own request; n=2 Patients in treatment with removable appliance, n=16 Patient removed from stuy due to time restraints: n=1 (control group) Patient removed from stuy due to technical failure: n=1 (alarm group) Patients in Alarm group; n=4 Patients in Calendar group; n=5 Patients in Control group; n=5 Box plot 1: Medel användningstid första 65 dagarna. Grupp 1 alarm, 2 kalender, 3 kontroll FINNS ÄVEN ANDRA SÄTT ATT REGISTRERA ANVÄDNINGSTIDEN KONKLUSION • TheraMon® användarvänlig och tillförlitlig • Van Beek aktivator med TheraMon® • känns smidig • Indikerar att påminnelse i form av ett mobilmeddelande ökar patienters compliance vid behandling med avtagbar apparatur ÅTER TILL STUDIEN OM ANVÄNDNINGSTID… STUDIENS BETYDELSE • Om det räcker att använda van Beek aktivatorn endast nattetid förenklas behandlingen för barn och föräldrar • Kunskap om optimal användningstid baseras på bristfälligt vetenskapligt underlag • Kunskap om ansiktstillväxt över tid är otillräcklig • Ökad kunskap är till förmån för patienter och vårdgivare SAMVERKAN Falun Gävle Örebro Stenungsund Östergötland Jönköping Halland Helsingborg Köpenhamn Växjö Östersund Hässleholm Lund Företag: Ivoclar – Lichtenstein; MC Tecchnology – Tyskland; Enzymatica – Lund; Sweorto - Framgångsfaktorer för forskning Samverkan Kompetens Entusiasm Forskning kommer att SKE !! Tack för att ni lyssnade på oss!