Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
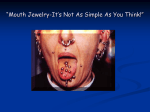
Continuing Education Course Number: 113.1 Bone Loss Associated With the Use of Tongue Piercing: Case Report Authored by Camila Stadiniski Gonçalves, DDS, Marcelo de Faveri, DDS, MS, PhD, Mitsue F. Hayacibara, DDS, MS, PhD, Osvaldo Magro Filho, DDS, MS, PhD and Roberto M. Hayacibara, DDS, MS Upon successful completion of this CE activity 1 CE credit hour may be awarded A Peer-Reviewed CE Activity by Dentistry Today is an ADA CERP Recognized Provider. Approved PACE Program Provider FAGD/MAGD Credit Approval does not imply acceptance by a state or provincial board of dentistry or AGD endorsement. June 1, 2006 to May 31, 2009 AGD Pace approval number: 309062 Opinions expressed by CE authors are their own and may not reflect those of Dentistry Today. Mention of specific product names does not infer endorsement by Dentistry Today. Information contained in CE articles and courses is not a substitute for sound clinical judgment and accepted standards of care. Participants are urged to contact their state dental boards for continuing education requirements. Continuing Education Recommendations for Fluoride Varnish Use in Caries Management Bone Loss Associated With the Use of Tongue Piercing: INTRODUCTION The popularity of wearing body adornments in unconventional places, such as the navel, nipples, eyebrow, lips, and tongue has grown significantly, thus contributing to reports of complications associated with this practice. Inserting metal objects in intraoral sites has become a common practice.1,2 The perforations are usually made in the tongue and lips 3,4, the tongue being the most frequent location,5,6 and they are usually placed anterior to the lingual frenum.1,5,7-9 The first case reported in the literature involving the use of tongue piercing was described by Scully and Chen8 in 1998. Thereafter, other reports in the scientific literature have recorded different complications that involve this body culture practice.3,5,7,10 The most common consequences associated with the use of tongue piercing are pain, swelling, and infection.3,7,8,11 In addition, there may be damage to perioral structures, compromised airway because of aspirating the device, and edema8,9; interference with speech, mastication, and deglutition3,7-9,11; Ludwig’s angina10; hypersensitivity to the metal7,9; obstruction in radiographic images7; galvanic current1; and hemorrhage due to the vascularity of the tongue and probability of blood vessel perforation.1,7 Intraoral structural damage can also occur, such as tooth chipping,1,5,6,9,11,12 gingival recession,1,2,5,11,13,14 and pulpal damage caused by chronic trauma.1,5,9,14 Most of the scientific studies that describe the complications of tongue piercing refer particularly to dental structure damage,1,5,6,9 but few articles have pointed out other damage in the oral cavity. Panagakos, et al13 and Kretchmer and Moriarty2 reported the first cases of loss of periodontal attachment related to the use of tongue piercing. However, there are few articles in the literature that refer to periodontal damage such as gingival recession and bone loss as a consequence of the use of tongue piercing, even with no gingival inflammation caused by dental biofilm. This paper reports a clinical case of tongue piercing which resulted in gingival recession and bone loss at the site of the mandibular central incisors. Case Report LEARNING OBJECTIVES: After reading this article, the individual will learn: • • Complications of tongue piercing. Diagnosis and treatment of bone loss caused by tongue piercing. ABOUT THE AUTHORS Dr. Gonçalves is in private practice in Maringá, PR, Brazil. She can be reached at [email protected]. Dr. Faveri is adjunct professor, Department of Periodontology, Dental Research Division, Guarulhos University, Guarulhos, SP, Brazil. He can be reached at [email protected]. Dr. Mitsue F. Hayacibara is adjunct professor, Department of Dentistry, State University of Maringá, Maringá, PR, Brazil. She can be reached at [email protected]. Dr. Magro-Filho is adjunct professor, Department of Surgery and Integrated Clinic, São Paulo State University “Júlio de Mesquita Filho,” Araçatuba, SP, Brazil. He can be reached at [email protected]. Dr. Roberto M. Hayacibara is assistant professor, Department of Dentistry, State University of Maringá, Maringá, PR, Brazil. He can be reached via e-mail at [email protected]. CASE REPORT Disclosure: The authors report no conflict of interest. The patient was an 18-year-old leukodermal man who 1 Continuing Education Bone Loss Associated With the Use of Tongue Piercing: Case Report had been wearing an orthodontic appliance for 36 months. During routine consultation it was observed that there was a loss of papilla involving teeth Nos. 24 and 25 (Figure 1). The patient was referred to the Periodontal Unit of the State University of Maringá (Brazil), where an intraoral examination showed that the site of the lingual mucosa membrane of the mandibular incisors was swollen and there was lingual gingival recession between teeth Nos. 24 and 25 (Figure 2). Periodontal examination revealed good oral hygiene (oral hygiene index of 22%15) and no other tooth presented any type of periodontal alteration. A barbell-shaped tongue piercing perforating the midline of the tongue was detected (Figure 3). The inferior ball of the piercing was in close contact with the swollen area and the mandibular central incisors (Figure 4). The patient reported that he had been wearing the jewelry for approximately 2 years. In the radiographic exam, bone loss of 5 mm between the mandibular central incisors was observed, involving more than half of the bone support, with characteristics of trauma, such as widening of the periodontal ligament and loss of integrity of the duralamina (Figure 5). The pretreatment orthodontic records showed no alteration in the bone support at the site of the mandibular central incisors (Figure 6). The proposed treatment was to remove the piercing and to follow up the case. A 3-month radiographic follow-up of the site after the piercing was removed showed absence of edema (Figure 7) and complete bone regeneration of the area at the lingual site between the mandibular central incisors (Figure 8). 8 Figure 1. Loss of papilla involving teeth Nos. 24 and 25. Figure 2. Lingual gingival recession between teeth Nos. 24 and 25; the site of the lingual mucous membrane of the mandibular incisors was swollen. Figure 3. Tongue piercing through the tongue, approximately 20 mm long. Figure 4. Tongue piercing through the tongue in close contact with both the area presenting edemas and the inferior mandibular central incisors. DISCUSSION healing period 7 to accommodate the swelling of the tongue that usually occurs in the first few days.3 Approximately 2 weeks after the perforation, the 18 mm temporary piercing is replaced by the permanent metal piercing 3 which can vary in length. There are numerous consequences related to this practice. Among them, 2 concerning damage in the oral cavity have repeatedly been mentioned in the literature: tooth chipping1,5,6,9 and gingival recession.1,2,5,13 Tooth Body piercing has become increasingly fashionable over the years, especially among young adults.5 The intraoral sites may involve lips, cheeks, tongue, and uvula.3 The tongue is the most commonly pierced intraoral site,6 and the perforation is usually made in the midline, in a ventral dorsum or dorsum ventral direction, and anterior to the lingual frenum.6 The procedure is usually performed without anesthesia 9 and in 2 stages.3,7 A temporary plastic stem, larger than the permanent one, is inserted during the 2 Continuing Education Bone Loss Associated With the Use of Tongue Piercing: Case Report chipping occurs mainly in the molars and premolars (61% and 31%, respectively) and 88% of the gingival recessions are present in the mandibular central incisors.5 In this case report the patient presented with buccallingual gingival recession at the site of the mandibular central incisors. The etiological factors related to gingival recession can be attributed to attachment loss due to periodontitis,16,17 presence of calculus,18 and a high lingual frenum.19 In addition, abrasion from toothpastes, excessive pressure when brushing, and horizontal movements of the brush could contribute to gingival injuries.20 However, as the patient presented with good oral hygiene, no gingival inflammation caused by dental biofilm, and a high lingual frenum, some of the possible causes of the recession were excluded. Abrasion from toothpastes and tooth brushing trauma were also excluded, since the recessions were restricted to 2 teeth, mainly at the lingual face. The other areas of the periodontium did not present with any disorder. The constant trauma caused by the tongue piercing during the tongue protrusion movements on the mandibular central incisors, associated with the significant size of the ball attached to the end of the metal piercing stem, were clearly indicated as the etiological factor of the problem.4,14 Gingival recession appears to be related to time of use and length of the piercing stem, with 15.9 mm or longer stems being associated with recessions, and shorter stems with tooth chipping.5 These 2 factors probably compounded the damage, considering the length of the piercing stem (20 mm) and the period of its use (2 years) (Figure 5). In this clinical case, the radiographic exam showed a horizontal bone loss of 5 mm between the mandibular central incisors. In agreement with current research, the possible factors related to bone resorption that occurs in the dental support tissues are an inflammatory lesion associated with dental plaque21 and/or occlusal trauma.22,23 Considering that intraoral examination of this patient did not reveal periodontal pocketing or bleeding on probing, the possibility of an inflammatory lesion associated with dental plaque was excluded. A clear explanation for such bone resorption and gingival recession was the presence of the piercing, a traumatic factor which probably caused the lesion to develop. This could be verified, as removal of the tongue piercing itself promoted regeneration of the Figure 5. Periapical radiograph. Bone loss in the mandibular central incisors area. Increase in periodontal thickening and discontinuity in the dental lamina. Figure 6. The pretreatment orthodontic records without alteration in the bone support at the site of the mandibular central incisors. Figure 7. Absence of edema at the inferior site after removing the piercing. Figure 8. Periapical radiograph. Bone regeneration in the lingual area of the inferior incisors, accentuated after removal of the tongue piercing. 3 Continuing Education Bone Loss Associated With the Use of Tongue Piercing: Case Report REFERENCES traumatized area. According to Panagakos, et al,13 who first described a case of loss of periodontal attachment related to a tongue piercing, the constant pressure applied in the area during functioning and as part of a parafunctional habit, along with gingival inflammation, led to the development of a severe loss of attachment. Kretchmer and Moriarty 2 also reported a situation in which the gingiva and alveolar bone were reduced because of the inflammation caused by dental biofilm associated with the constant trauma caused by a piercing. When compared with occlusion trauma, piercing trauma alone can lead to bone loss, but it cannot cause loss of periodontal attachment. When associated with dental plaque, trauma can increase the speed of periodontal disease progression, acting as a co-factor in the destructive process.24 Therefore, Choe, et al 11 agreed that tongue piercing can be a periodontal risk factor.12 Another important aspect to consider in this case is the possibility that the trauma caused by the piercing could result in an oral pathologic tooth migration of the central incisors, as a reaction to the aggression. As the alveolar bone is usually remodeled to adapt to functional changes, this situation could have occurred if the patient had not worn an orthodontic appliance. Thus, it is likely that the orthodontic appliance acted to contain the trauma, and the bone reacted through a pathological resorption. When such devices are seen by clinicians, they should be removed or the patient should be advised of the risk of retaining such a device. If the patient declines to have it removed, he/she should sign a release form to be added to the chart stating: “I have been been advised of the risks of having an oral device in my mouth, decline to have the oral device removed, and accept all risks associated with retaining it.” 1. De Moor RJ, De Witte AM, De Bruyne MA. Tongue piercing and associated oral and dental complications. Endod Dent Traumatol. 2000; 16:232-237. 2. Kretchmer MC, Moriarty JD. Metal piercing through the tongue and localized loss of attachment: a case report. J Periodontol. 2001;72:831-833. 3. Farah CS, Harmon DM. Tongue piercing: case report and review of current practice. Aust Dent J. 1998;43:387-389. 4. Zadik Y, Sandler V. Periodontal attachment loss due to applying force by tongue piercing. J Calif Dent Assoc. 2007;35:550-553. 5. Campbell A, Moore A, Williams E, et al. Tongue piercing: impact of time and barbell stem length on lingual gingival recession and tooth chipping. J Periodontol. 2002;73:289-297. 6. Bassiouny MA, Deem LP, Deem TE. Tongue piercing: a restorative perspective. Quintessence Int. 2001;32:477-481. 7. Price SS, Lewis MW. Body piercing involving oral sites. J Am Dent Assoc. 1997;128:1017-1020. 8. Scully C, Chen M. Tongue piercing (oral body art). Br J Oral Maxillofac Surg. 1994;32:37-38. 9. Reichl RB, Dailey JC. Intraoral body-piercing: a case report. Gen Dent. 1996;44:346-347. 10. Perkins CS, Meisner J, Harrison JM. A complication of tongue piercing. Br Dent J. 1997;182:147-148. 11. Choe J, Almas K, Schoor R. Tongue piercing as risk factor to periodontal health. NY State Dent J. 2005;71:40-43. 12. De Moor RJ, De Witte AM, Delmé KI, et al. Dental and oral complications of lip and tongue piercings. Br Dent J. 2005;199:506-509. 13. Panagakos FS, Linfante J, Pascuzzi JN. Attachment loss associated with the presence of a tongue bar: a case report. Gen Dent. 2000;48:454-456. 14. Levin L. Alveolar bone loss and gingival recession due to lip and tongue piercing. NY State Dent J. 2007;73:48-50. 15. Lindhe J, Okamoto H, Yoneyama T, et al. Longitudinal changes in periodontal disease in untreated subjects. J Clin Periodontol. 1989;16:662-670. CONCLUSION 16. Löe H, Anerud A, Boysen H. The natural history of periodontal disease in man: prevalence, severity, and extent of gingival recession. J Periodontol. 1992;63:489-495. Under certain circumstances, the extensive use of tongue piercing can lead to bone loss and gingival recession in the area of the mandibular central incisors. 17. Yoneyama T, Okamoto H, Lindhe J, et al. Probing depth, attachment loss and gingival recession. Findings from a clinical examination in Ushiku, Japan. J Clin Periodontol. 1988;15:581-591. 4 Continuing Education Bone Loss Associated With the Use of Tongue Piercing: Case Report 18. van Palenstein Helderman WH, Lembariti BS, van der Weijden GA, et al. Gingival recession and its association with calculus in subjects deprived of prophylactic dental care. J Clin Periodontol. 1998;25:106-111. 22. Lindhe J, Ericsson I. The effect of elimination of jiggling forces on periodontally exposed teeth in the dog. J Periodontol. 1982;53:562-567. 19. Ewart NP. A lingual mucogingival problem associated with ankyloglossia: a case report. NZ Dent J. 1990;86:16-17. 23. Lindhe J, Svanberg G. Influences of trauma from occlusion on progression of experimental periodontitis in the beagle dog. J Clin Periodontol. 1974;1:3-14. 20. Holmstrup P, van Steenbergue D. Non-plaque induced inflammatory gingival lesions. In: Lindhe J, Karring T, Lang NP, eds. Clinical Periodontology and Implant Dentistry. 4th ed. Oxford, England: Blackwell Munksgaard; 2003:289. 24. Lindhe J, Nyman S, Ericsson I. Trauma from occlusion. In: Lindhe J, Karring T, Lang NP, eds. Clinical Periodontology and Implant Dentistry. 4th ed. Oxford, England: Blackwell Munksgaard; 2003:352. 21. Kinane DF, Berglundh T, Lindhe J. Host-parasite interactions in periodontal disease. In: Lindhe J, Karring T, Lang NP, eds. Clinical Periodontology and Implant Dentistry. 4th ed. Oxford, England: Blackwell Munksgaard; 2003:150. 5 Continuing Education Bone Loss Associated With the Use of Tongue Piercing: Case Report 3. In tongue piercing, the perforation is usually made: a. in the midline. b. in a ventral-dorsum or dorsum-ventral direction. c. anterior to the lingual frenum. d. all of the above. POST EXAMINATION INFORMATION To receive continuing education credit for participation in this educational activity you must complete the program post examination and receive a score of 70% or better. Traditional Completion Option: You may fax or mail your answers with payment to Dentistry Today (see Traditional Completion Information on following page). All information requested must be provided in order to process the program for credit. Be sure to complete your “Payment”, “Personal Certification Information”, “Answers” and “Evaluation” forms, Your exam will be graded within 72 hours of receipt. Upon successful completion of the post-exam (70% or higher), a “letter of completion” will be mailed to the address provided. 4. The tongue piercing procedure is usually performed without anesthesia. The procedure is usually performed in 3 stages. a. First statement is false, second is true b. First statement is true, second is false c. Both statements are false d. Both statements are true Online Completion Option: Use this page to review the questions and mark your answers. Return to dentalCEtoday.com and signin. If you have not previously purchased the program select it from the “Online Courses” listing and complete the online purchase process. Once purchased the program will be added to your User History page where a Take Exam link will be provided directly across from the program title. Select the Take Exam link, complete all the program questions and Submit your answers. An immediate grade report will be provided. Upon receiving a passing grade complete the online evaluation form. Upon submitting the form your Letter Of Completion will be provided immediately for printing. 5. With tongue piercing _____ % of tooth chipping occurs in the molars. a. 31 b. 42 c. 61 d. 75 6. _____% of the gingival recessions associated with tongue piercing are present in the mandibular central incisors. a. Thirty-one (31) b. Sixty-one (61) c. Seventy-five (75) d. Eighty-eight (88) General Program Information: Online users may login to dentalCEtoday.com anytime in the future to access previously purchased programs and view or print “letters of completion” and results. 7. Metal stems 15.9 mm or longer are associated with gingival recessions. Shorter stems are associated with tooth chipping. a. First statement is false, second is true b. First statement is true, second is false c. Both statements are false d. Both statements are true POST EXAMINATION QUESTIONS 1. The most frequent intraoral site for inserting metal objects is: a. lips. b. cheeks. c. tongue. d. uvula. 8. When compared with occlusion trauma piercing trauma can lead to bone loss. When associated with dental plaque, piercing trauma can increase the speed of periodontal disease progression. a. First statement is false, second is true b. First statement is true, second is false c. Both statements are false d. Both statements are true 2. The most common consequence(s) associated with tongue piercing is/are: a. pain. b. swelling. c. infection. d. all of the above. 6 Continuing Education Bone Loss Associated With the Use of Tongue Piercing: Case Report PROGRAM COMPLETION INFORMATION PERSONAL CERTIFICATION INFORMATION: If you wish to purchase and complete this activity traditionally (mail or fax) rather than Online, you must provide the information requested below. Please be sure to select your answers carefully and complete the evaluation information. To receive credit you must answer at least six of the eight questions correctly. Last Name (PLEASE PRINT CLEARLY OR TYPE) First Name Profession / Credentials Complete online at: www.dentalcetoday.com Street Address TRADITIONAL COMPLETION INFORMATION: Suite or Apartment Number Mail or Fax this completed form with payment to: City License Number State Zip Code Dentistry Today Daytime Telephone Number With Area Code Department of Continuing Education 100 Passaic Avenue Fairfield, NJ 07004 Fax Number With Area Code Fax: 973-882-3662 E-mail Address PAYMENT & CREDIT INFORMATION: ANSWER FORM: COURSE #: 113.1 Examination Fee: $20.00 Credit Hours: 1.0 Note: There is a $10 surcharge to process a check drawn on any bank other than a US bank. Should you have additional questions, please contact us at (973) 882-4700. Please check the correct box for each question below. 1. o a o b o c o d 5. o a o b oc od o I have enclosed a check or money order. 2. o a o b o c o d 6. o a o b oc od o I am using a credit card. 3. o a o b o c o d 7. o a o b oc od 4. o a o b o c o d 8. o a o b oc od My Credit Card information is provided below. o American Express o Visa o MC o Discover Please provide the following PROGRAM EVAUATION FORM (please print clearly): Please complete the following activity evaluation questions. Rating Scale: Excellent = 5 and Poor = 0 Exact Name on Credit Card / Credit Card # Expiration Date Content was useful and benefited your clinical practice. Review questions were clear and relevant to the editorial. Signature Dentistry Today is an ADA CERP Recognized Provider. Course objectives were achieved. Approved PACE Program Provider FAGD/MAGD Credit Approval does not imply acceptance by a state or provincial board of dentistry or AGD endorsement. June 1, 2006 to May 31, 2009 AGD Pace approval number: 309062 Illustrations and photographs were clear and relevant. Written presentation was informative and concise. How much time did you spend reading the activity & completing the test?