Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
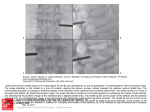
Xray Rounds- CLEARING THE C-SPINE Gaetano P. Monteleone, Jr., M.D. Dept of Family Medicine Division of Sports Medicine West Virginia University School of Medicine I. Standard C-spine series: Anteropasterior (AP) view Lateral (cross-table) view Open mouth view (Fuch's, Water’s) II. Additional views: Obliques Lateral flexion/extension Swimmer's view III. Injuries: Fractures, instability (ligaments), cervical stenosis IV. General A. In children, cervical spine injuries generally affect C1, C2 or the atlanto-occipital articulation. In adults, most injuries involve C3 C7. V. Some Specifics A. Lateral view- this is the most important view. All seven cervical vertebrae and the superior portion of the first thoracic vertebra must be visualized before proceeding. If these vertebrae are not seen, repeat lateral with downward traction on the arm or obtain the swimmer's view (humerus in 170-180° forward flexion). • Four lines should be roughly parallel: anterior and posterior vertebral bodies, spinolaminar line and the spinous process line. • Atlantodens interval (ADI) < 3 mm adults ( < 5mm, children). Distance between atlas and dens of the axis. AKA atlantoaxial interval. 3-5mm = torn transverse ligament and possible atlantoaxial instability; Atlantoaxial dislocation more common in rheumatoid arthritis and Downs . • The retropharyngeal space (B) in upper vertebrae should not exceed 7 mm, may be indirect evidence for injury. Similarly, the prevertebral fat stripe (C) should not be blurred or displaced. • Disc spaces should be maintained, facet joints and interspinous distances should be 1 Xray Rounds- CLEARING THE C-SPINE Gaetano P. Monteleone, Jr., M.D. Dept of Family Medicine Division of Sports Medicine West Virginia University School of Medicine • • • • • • • symmetrical. Assymetry of interspinous distances may reflect rupture of posterior longitudinal ligament. Vertebral body height should be checked. Vertebral canal measurements: normal > 13 mm, usually measured at C5 typically the most narrow part of the canal. Because of magnification factors and radiographic technique, a ratio method described by Torg and Pavlov was also suggested. Ratio of a (measure posterior vertebral body to spinolaminar line) to b (measure width of vertebral body). a/b < 0.80 suggestive of cervical spinal stenosis. Cantu, Herzog, Odor and others find this ratio method inaccurate in diagnosis of spinal stenosis. The ave. AP diameter of the canal is ≈ 22 mm at C1, 20 mm at C2, and 17 mm at C3 - C7. Studies have demonstrated the normal sagital diameter of the spinal cord ranges from ≈ 0.5 to 11.5 mm. Proposed that more important to assess "functional" cervical spinal stenosis via MRI. MRI may demonstrate impingement of the cord, ablation of the normal CSF fluid around the cord. B. AP view: offers less information than lateral view. Parallel lines at spinous processes and pedicles. Disc spaces equal and maintained. Vertebral bodies checked for fracture. C. Open-mouth view (Fuch's): Odontoid fractures-the overlapping shadows of base of skull and incisor teeth may simulate fx. Lateral masses- Medial aspect of C1 lateral masses should be equidistant to the odontoid. In addition, these lateral masses should be perfectly aligned with lateral masses of C2. The normal distance between C1 lateral masses is < 7mm (figure 5). If greater distance, indicates ruptured transverse ligament or Jefferson fx (burst fx of C1). 1 A Water's view also looks at the odontoid from under chin to vertex of head. 1 Jefferson fx is usually NOT associated with severe neurologic deficits and may not be obvious at first glance. 2 Xray Rounds- CLEARING THE C-SPINE Gaetano P. Monteleone, Jr., M.D. Dept of Family Medicine Division of Sports Medicine West Virginia University School of Medicine • D. Additional views: Lateral flexion/extension views- Have patient actively flex and extend neck to obtain this view. Severe hyperflexion may produce injury to disruption of posterior ligaments. Hyperextension may produce teardrop fx2 (figure 18) or anterior ligament injury. Check angle produced by lines drawn at inferior vertebral bodies of two adjacent vertebrae. Angle > 11° indicates ligamentous instability. Instability also demonstrated with horizontal translation of one vertebral body on another of > 3.5 mm. 2 Teardrop fx involves the anteroinferior portion of the vertebral body with hyperextension. Most commonly affects C2. 3