Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Page 1 of 6
View this article online at: patient.info/health/scabies-leaflet
Scabies
Scabies is an extremely itchy skin disorder that can be passed from one person to another. It is
caused by an infestation with a parasite - the scabies mite. The mite lives on the skin and burrows
into it. Scabies is spread to others through close skin-to-skin contact. It is easily treated with an
insecticide lotion applied to the skin. Two applications of treatment are needed, one week apart.
What is scabies?
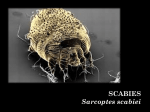
Scabies is caused by a mite (like a tiny insect) called Sarcoptes scabiei. The mite is a parasite, meaning it lives
off the host (a human) with no benefit to the host.
Scabies mites are tiny. They have a cream-coloured body, bristles and spines on their back, and four pairs of
legs. The female mite is bigger (about 0.4 mm x 0.3 mm) compared with the male (0.2 mm x 0.15 mm). With the
naked eye you might be able to see them as a speck. The female mites tunnel into the skin and lay eggs. About
40-50 eggs are laid in the lifetime of a mite. The eggs hatch into larvae after 3-4 days; these then grow into adults
within 10-15 days.
Most of the symptoms of scabies are due to your immune system's response to the mites, or to their saliva, their
eggs or their poo (faeces). In other words, the rash and the itching are mostly caused by your body's allergic-like
reaction to the mites, rather than the mites themselves.
The average number of mites on an infested person is 12.
How common is scabies?
Scabies is common. In the UK, about 1 in 1,000 people develop scabies each month. Scabies is more common
in town (urban) areas, in women and children, in the winter, and in the North of the country. It is very common
worldwide, particularly where there is poverty and overcrowding. There may be outbreaks in overcrowded places
such as refugee camps.
How do you get scabies?
You need close skin-to-skin contact with an infected person to catch scabies. This is because the scabies mite
cannot jump or fly.
Most cases of scabies are probably caught from prolonged hand-holding with an infected person. The hand is the
most common site to be first affected.
Close skin-to-skin contact when having sex is another common way of catching scabies.
The skin-to-skin contact needs to be for a reasonable time to catch the mite. You usually need to be in skin
contact for 15-20 minutes to catch scabies. Therefore, you are unlikely to catch scabies from an infected person
by casual short contact such as a handshake or a hug. The more mites there are, the faster they can spread to
another person.
The mites live in skin and can survive away from the host human for about 24-36 hours. You are unlikely to catch
scabies from bedding and towels unless you use them immediately after being used by someone with scabies.
However, just in case, it is best to treat bedding and towels by hot washing (described later).
Page 2 of 6
Sometimes outbreaks of scabies occur in places such as nurseries and residential homes, where people are in
regular close contact.
What are the symptoms of scabies?
Itching. This is the main symptom of scabies. This is often severe and tends to be in one place at first
(often the hands), and then spreads to other areas. The itch is generally worse at night and after a hot
bath. You can itch all over, even with only a few mites, and even in the areas where the mites are not
present.
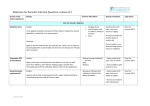
Mite tunnels (burrows). These may be seen on the skin as fine, dark, or silvery lines about 2-10 mm
long. They most commonly occur in the loose skin between the fingers (the web spaces), the inner
surface of the wrists, and the hands. However, they can occur on any part of the skin. You may not
notice the burrows until a rash or itch develops.
Rash . The rash usually appears soon after the itch starts. It is typically a blotchy, lumpy red rash that
can appear anywhere on the body. The rash is often most obvious on the inside of the thighs, parts of
the tummy (abdomen) and buttocks, armpits, and around the nipples in women. The appearance of
the rash is often typical. However, some people develop unusual rashes which may be confused with
other skin conditions.
Scratching. Scratching due to intense itching can cause minor skin damage. In some cases the
damaged skin becomes infected by other germs (bacteria). This is a secondary skin infection. If skin
becomes infected with bacteria it becomes red, inflamed, hot, and tender.
Aggravation of pre-existing skin conditions. Scabies can worsen the symptoms of other skin
conditions, particularly itchy skin problems such as eczema, or problems such as psoriasis. Scabies
can be more difficult to diagnose in these situations too.
Note: the itch and rash of scabies are due to a reaction (allergy) to the mites (or their saliva, poo (faeces) or
eggs). Scabies symptoms usually take 2-6 weeks to occur after you are first infected. The itch and rash can
develop on any part of the skin, away from where the mites are actually burrowing. This means that you are
infectious and can spread scabies before you even know you have scabies.
The picture above shows some typical mite tunnels (burrows) either side of the wrist skin crease. The picture
below shows the typical rash that occurs as a reaction to the mites, in this case on the leg.
Page 3 of 6
Symptoms of recurring infection
The itch and rash normally take 2-6 weeks to develop when you have a first scabies infection. However, if you
have scabies and it is cleared with treatment, and then you catch it again, the symptoms may be slightly different.
In such instances the rash and itching develop much more quickly - often within a day or two. This is because the
first scabies infestation has already sensitised your immune system. It then reacts much more quickly with this
second bout of scabies.
How is scabies diagnosed?
Scabies is usually diagnosed just by looking at the rash. A doctor will often be able to recognise the typical
appearance of the scabies rash.
Often, a doctor will find one or more mite tunnels (burrows) on the skin to confirm the diagnosis. Sometimes the
doctor will rub some ink on the skin, and then wipe it off. If there are burrows in that area of skin, the ink will move
along the burrow under the skin. It will be visible as a line after the rest of the ink has been wiped away.
It is sometimes difficult to tell the difference between the rash caused by scabies and the rashes of some other
skin conditions. Therefore, a scraping from the skin is sometimes sent to the laboratory to look for mites under
the microscope if there is doubt about the diagnosis.
If itching and a rash develop in several people who live in the same home at about the same time then scabies is
a likely cause.
Who should be treated?
Scabies can stay in your skin for ever if not treated. Treatment is needed for:
Anybody who has scabies; AND
All household members, close contacts, and sleeping/sexual partners of the affected person - even if
they have no symptoms. This is because it can take up to six weeks to develop symptoms after you
become infected. Close contacts may be infected, but have no symptoms, and may pass on the mite.
Note: everyone who is treated should be treated at the same time - that is, on the same day.
Page 4 of 6
How is scabies treated?
Scabies is curable. The usual scabies treatment is with permethrin cream. Permethrin is an insecticide that kills
the mites. This is known to be the treatment that works the best. If permethrin cannot be used, an alternative is to
use a lotion called malathion liquid. (For example, some people may be allergic to permethrin.)
You can buy both of these products from pharmacies. You can also obtain them on prescription. They are easy to
apply and normally work well if used properly.
Re-apply the same treatment seven days after the first application. This helps to make sure that all the mites are
killed.
Daily hot baths, and scrubbing with soap and water will NOT cure a scabies infestation. Insecticide MUST be
used.
Tips for successful treatment
Read the leaflet that comes with the product, for exact instructions as to where to apply. Usually
treatment is applied to the whole body including the scalp and face, whilst others are to be applied just
from the neck down. Remember to include awkward places such as the back, soles of the feet,
between fingers and toes, under fingernails, and the genitals. Pay special attention to the areas where
mite tunnels (burrows) most commonly occur. That is, in between the fingers, the front of the wrists
and elbows, beneath the breasts, the armpits, and around the nipples in women.
An adult needs at least 30 g of cream or 100 ml of lotion to cover the whole body. So, for two
applications you will need at least 60 g of cream or 200 ml of lotion per adult.
Apply cream or lotion to cool dry skin (not after a hot bath).
The cream or lotion should be left on for the full recommended time. Permethrin cream should be left
on for 8-12 hours. Malathion lotion should be left on for 24 hours.
Children should stay off school until the first application of treatment has been completed.
If you wash your hands or any other part of your body during the treatment period, you should re-apply
the cream or lotion to the washed areas.
Breast-feeding mothers should wash off the lotion or cream from the nipples before breast-feeding,
and re-apply treatment after the feed.
Permethrin cream is not usually used for babies under the age of 2 months, and malathion is not
usually used under the age of 6 months.
Put mittens on babies to stop them licking the cream or lotion off their hands.
Clothes, towels, and bed linen should be machine-washed at 50°C or above after the first application
of treatment. This kills the scabies mites. Keep any items of clothing that cannot be washed, in plastic
bags for at least 72 hours to contain the mites until they die. Alternative options to kill any mites on
clothes and linen are ironing the item with a hot iron, dry cleaning, or putting items in a dryer on the hot
cycle for 10-30 minutes. It is not necessary to fumigate living areas or furniture, or to treat pets.
Some people who develop a secondary skin infection may also need antibiotics. If you suspect this is
the case, you should consult a doctor.
See a doctor if the itch persists longer than 2-3 weeks after treatment. Sometimes the first treatment does not
work, and a different one is then needed. The most common reasons why treatment fails, and scabies returns
(recurs), are:
The cream or lotion is not applied correctly for the recommended time.
A close contact is not treated at the same time, and the infection is passed back.
Note: you will still be itchy for a while after successful treatment. It is normal to take up to 2-3 weeks (and
sometimes up to six weeks) for the itch to go completely after the mites have been killed by treatment.
Also, even after successful treatment, in a small number of cases there remain some itchy brownish-red lumps
(nodules) up to 2 cm in diameter. If these remain, they most commonly occur on the genitals and armpits. These
lumps are neither infectious, nor mean that the mite is still present. They occur in some cases as a prolonged
skin reaction to the scabies mite. If they occur, they usually go within three months, but occasionally last up to
one year.
Page 5 of 6
Treatment for itching
Itching can be a distressing symptom. It can be eased either with topical treatments that you apply to the skin
(such as creams or lotions), or with medication taken by mouth. Your GP or pharmacist can usually give advice
regarding suitable products. Even cold moisturisers (emollients), especially if they contain menthol, can provide
temporary relief. Avoid applying strong steroid creams, especially if the diagnosis of scabies is uncertain.
Crotamiton cream or lotion has soothing qualities and may help to relieve itch. Apply crotamiton 2-3
times a day (but only once a day for children under 3 years old).
Hydrocortisone cream. This is a mild steroid cream that may ease any inflammation and help to ease
itch. It can be bought from the chemist, or obtained by prescription. It can be applied once or twice per
day, for up to a week.
An antihistamine medicine that makes you drowsy, such as chlorphenamine (brand name Piriton®).
This does not ease the itch directly, but can help you to sleep if itching is a problem at night
(particularly for children). It is not licensed for this use, but can be safely used under the direction of a
doctor.
Crusted scabies ('Norwegian' scabies)
This type of scabies is unusual, and most people who develop scabies do not get 'Norwegian' scabies.
It is a more severe form of scabies with a hyperinfestation of lots of scabies mites. This means that there are
thousands or millions of the mites, causing excessive scaling and flaking of the skin. Because there are so many
mites, and because the skin is flaking off, scabies can be spread to others extremely easily. The rash is crusting
(and looks a bit like psoriasis). It can be very extensive and can, if severe, lead to serious secondary bacterial
skin infections.
Crusted scabies mainly occurs in people who have a poor immune system (are immunocompromised). The
types of people who might get crusted scabies include:
People with HIV/AIDS.
People having chemotherapy.
Frail people who are elderly or ill due to other conditions.
Are poorly fed (malnourished).
Have learning difficulties (because they cannot comprehend or respond to the itch).
Have nerve-related problems (because they cannot feel the itch).
Crusted scabies is more easily transmitted through contact with towels, bedding and upholstery. In crusted
scabies, the mites can survive for a few days away from their host. Even minimally exposed people, such as
cleaners and laundry personnel, are at risk from crusted scabies and need insecticide treatment if they are
working in an institution with an outbreak. An outbreak in an institution with many vulnerable people, such as a
nursing home, can be extremely challenging. It is likely that all residents and all staff would require treatment.
A healthy person with a normal immune system would develop 'normal' scabies if infested with the scabies mite
following contact with someone who had crusted scabies.
Crusted scabies may be impossible to eradicate in people with HIV infection, and recurrences are common.
Further reading & references
Scabies; DermNet NZ
Scabies, DermIS (Dermatology Information System)
Scabies; NICE CKS, December 2011 (UK access only)
Strong M, Johnstone PW; Interventions for treating scabies. Cochrane Database Syst Rev. 2007 Jul 18;(3):CD000320.
Gunning K, Pippitt K, Kiraly B, et al; Pediculosis and scabies: treatment update. Am Fam Physician. 2012 Sep
15;86(6):535-41.
FitzGerald D, Grainger RJ, Reid A; Interventions for preventing the spread of infestation in close contacts of people with
scabies. Cochrane Database Syst Rev. 2014 Feb 24;2:CD009943. doi: 10.1002/14651858.CD009943.pub2.
Engelman D, Kiang K, Chosidow O, et al; Toward the global control of human scabies: introducing the International
Alliance for the Control of Scabies. PLoS Negl Trop Dis. 2013 Aug 8;7(8):e2167. doi: 10.1371/journal.pntd.0002167.
eCollection 2013.
Page 6 of 6
Disclaimer: This article is for information only and should not be used for the diagnosis or treatment of medical
conditions. EMIS has used all reasonable care in compiling the information but make no warranty as to its
accuracy. Consult a doctor or other health care professional for diagnosis and treatment of medical conditions.
For details see our conditions.
Original Author:
Dr Tim Kenny
Current Version:
Dr Mary Harding
Peer Reviewer:
Dr Helen Huins
Document ID:
4325 (v43)
Last Checked:
28/10/2014
Next Review:
27/10/2017
View this article online at: patient.info/health/scabies-leaflet
Discuss Scabies and find more trusted resources at Patient.
© EMIS Group plc - all rights reserved.