Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
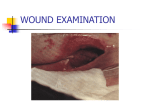
Management of Leg Ulceration for Adults Policy Policy Date: September 2014 Policy Version: (V6.1) September 2014 TARGET AUDIENCE (including temporary staff) People who need to know this document in detail All clinical staff involved in caring for patients with leg ulceration People who need to have a broad understanding of this document All clinical staff caring for patients with leg ulceration People who need to know that this document exists All staff caring for patients with leg ulceration Policy Author: Tissue Viability Nurse Approved by: Trust-wide Clinical Governance Group Date: 25/11/2014 Ratified by: Trust-wide Clinical Governance Group Date: 25/11/2014 Date of next review: November 2016 Management of Leg Ulceration for Adults Policy CONTENTS Page 1. INTRODUCTION 5 1.1 Purpose 5 1.2 Scope 5 1.3 Definitions 5 2. MANAGEMENT OF LEG ULCERATION 5 2.1 Training 5 2.2 Assessment 6 2.3 Aetiology 2.3.1 Venous Ulceration 2.3.2 Arterial Ulceration 2.3.3 Mixed Venous / Arterial Ulceration 6 6 6 6 2.4 Doppler Ultrasound 6 2.5 Use of Bandages 2.5.1 Arterial Disease 2.5.2 Venous Disease 2.5.3 Mixed venous/arterial disease 2.5.4 Measuring the Limb 6 7 7 7 7 2.6 Wound Management 2.6.1 Arterial Ulceration 2.6.2 Venous Ulceration 2.6.3 Mixed Venous / Arterial Ulceration 2.6.4 Wound Cleansing and Skin Care 8 8 8 8 8 2.7 Management of Varicose Eczema 2.7.1 Dry Varicose Eczema 2.7.2 Wet or Weeping Varicose Eczema 8 9 9 2.8 Management of Infection and Infection Control 2.8.1 Diagnosis and Treatment of Wound Infection 2.8.2 Use of Equipment and dressing materials 9 9 10 2.9 Elevation and Exercise 2.9.1 Venous Disease 2.9.2 Arterial Disease 2.9.3 Mixed venous/arterial disease 10 10 10 10 2.10 Referral for Further Advice 11 Excellent care at the heart of the community Page 2 of 32 Management of Leg Ulceration for Adults Policy 2.10.1 Tissue Viability Service 2.10.2 Vascular Surgical Departments 2.10.3 Dermatology Department 11 11 11 2.11 Prevention of Ulcer Recurrence 11 2.12 Smoking 12 3. RESPONSIBILITIES 12 4. ASSOCIATED DOCUMENTS AND REFERENCES 13 5. MONITORING COMPLIANCE 14 6 DISSEMINATION AND IMPLEMENTATION 14 7. CONSULTATION, APPROVAL, RATIFICATION & REVIEW 14 8. VERSION CONTROL 15 APPENDIX A Leg Ulceration Differential Diagnosis Assessment Form 16 APPENDIX B DOPPLER ULTRASOUND PROCEDURE 19 APPENDIX C EXAMPLES OF BANDAGE AND COMPRESSION SYSTEMS ON 23 APPENDIX D FINGER TIP UNITS 24 APPENDIX E ANKLE EXERCISES TO AID LOWER LIMB CIRCULATION 25 9 Equality Analysis 27 10 Ratification Checklist 33 Page 3 of 32 Excellent care at the heart of the community Management of Leg Ulceration for Adults Policy 1. INTRODUCTION 1.1 Purpose This document will outline the Trust’s expectations of staff involved in treating patients with leg ulceration and will offer guidelines on how to approach the patient’s treatment plan. 1.2 Scope This document covers management of venous ulceration, arterial ulceration and mixed venous/arterial ulceration. Guidance on management of diabetic foot ulceration is available in a separate document. 1.3 Definitions Aetiology the cause of the disease Venous leg ulceration disease of the veins resulting in ulceration caused by poor venous return of blood from the lower leg to the heart Arterial leg ulceration disease of the arteries resulting in ulceration from poor arterial flow from the heart to the lower leg Mixed Venous/Arterial leg ulceration disease of both veins and arteries resulting in ulceration which can complicate diagnosis and treatment plan 2. MANAGEMENT OF LEG ULCERATION Clinical staff are required to follow the guidance below in order to provide the optimum treatment for patients with leg ulceration. 2.1 Training All clinical staff involved in assessment and treatment of patients with leg ulceration must attend training and maintain their skills by regular practice. Details of current training programmes are available on the Pulse. An appropriate mentor should assess skills in use of Doppler and compression bandaging before the clinician is involved in patient care and re-assessed every three years. Excellent care at the heart of the community Page 4 of 32 Management of Leg Ulceration for Adults Policy 2.2 Assessment It is essential that all patients presenting with leg ulceration receive a thorough holistic assessment. A Leg Ulcer Assessment form is provided as an aide memoir (see Appendix A). This is to determine a differential diagnosis of either venous or arterial ulceration, or to identify those patients whose treatment is complicated by a mixed aetiology of both venous and arterial disease. Referral for further investigation may be required to determine the exact diagnosis and therefore the most appropriate treatment. Please consider if it is appropriate for the patient to be educated and supported to perform some care of the leg ulcer themselves. This may involve education in cleansing and dressing of the ulcer and the use of compression hosiery garments. 2.3 Aetiology 2.3.1 Venous ulceration Venous ulceration occurs as a result of chronic venous hypertension, which leads to backflow of blood and congestion in the venous system. 2.3.2 Arterial Ulceration Arterial ulcers are the result of occlusion or reduction of blood flow in the arteries. 2.3.3 Mixed Venous/Arterial Ulceration Patients with venous disease may also have concurrent arterial disease and vice versa, giving rise to a mixed venous/arterial aetiology. When patients have mixed aetiology leg ulceration, the advice contained in these guidelines needs to be considered and appropriately applied depending on the primary problems encountered. Determining treatment for patients with mixed venous/arterial disease can be complex and advice can be sought from the Tissue Viability Service if required. See appendix B for referral form. 2.4 Doppler Ultrasound For clinical assessment of patients with leg ulceration, Doppler ultrasound compares the brachial systolic pressure with the ankle systolic pressure, thereby determining the severity of any impairment of arterial blood flow to the feet. This results in a ratio number known as the Ankle Brachial Pressure Index (ABPI). The use of Doppler is an important part of the assessment process and must be performed on all patients presenting with leg ulceration following appropriate informed consent guidance. Doppler assessment must be carried out by a practitioner who has undertaken appropriate training. See appendix C for procedure of obtaining and interpreting ABPI measurements. 2.5 Use of Bandages Selection of bandages should be from the current Brighton & Hove (ONPOS) or West Sussex Wound Care Formulary, unless clinical reasoning for variance can be justified in the patient record. When any degree of compression is used, the patient’s ankle Page 5 of 32 Excellent care at the heart of the community Management of Leg Ulceration for Adults Policy circumference must be measured first and then the correct kit or size of bandage chosen, depending on the ankle measurement. Under-bandage padding must always be used to avoid pressure damage to bony prominences. The under bandage padding can also be used to reshape a limb where the calf is either too narrow or too wide. In bedded units, if compression therapy is required and staff are not trained to do this, please contact the patient’s community nursing team or the TVN service for advice. See appendix D for examples of bandage systems. 2.5.1 Arterial Disease Patients with arterial disease should have dressings secured by light, cotton or crepe bandages applied without tension to avoid the risk of further arterial occlusion. 2.5.2 Venous Disease Patients with venous disease must be offered full compression as the mainstay of treatment for venous hypertension. This is usually in the form of bandaging systems in the active phase of ulceration, although hosiery may also be utilised. It has been demonstrated by extensive research that sustained compression of 35-40 mmHg at the ankle, graduated to 17-20mmHg just below the knee enhances healing of venous leg ulcers by reversing venous hypertension. This level of compression is achieved by using one of the high compression bandaging systems in the Brighton and Hove or West Sussex Wound Formularies. High compression must only be applied to a patient with an ABPI of between 0.8 and 1.3, as determined by Doppler assessment. It is imperative that the bandages that achieve these high rates of compression are correctly applied. It is the responsibility of the practitioner applying the bandages to ensure their competence in bandaging techniques through appropriate training, regular practice and updating of skills. Inappropriate or inexpert bandaging can lead to limb loss. Any delegation of bandage application to non-registered practitioners remains the responsibility of the registered practitioner, therefore competencies must be reviewed on a regular basis. 2.5.3 Mixed Venous/Arterial Disease For patients with mixed aetiology leg ulceration and ABPI readings of between 0.7 – 0.8, it may be helpful to apply reduced compression of 15-25 mmHg to control oedema and leakage of fluid from the tissues. For readings between 0.5 – 0.7 there needs to be a clear discussion with the Tissue Viability Service or the Vascular Services before a decision to apply reduced compression is started. Reduced compression can be achieved by varying the approach to bandaging systems, e.g. by omitting either the 3rd or 4th layer of the multilayer bandaging systems, or by utilising a bandage designed for this purpose. Shortstretch bandages cannot be used to achieve reduced compression. 2.5.4 Measuring the Limb Before commencing compression therapy, refer to the manufacturer’s instructions of the chosen bandage system. The patient’s ankle circumferences must then be measured with a disposable single use measuring tape. Excellent care at the heart of the community Page 6 of 32 Management of Leg Ulceration for Adults Policy • If the ankle circumference is <18cm, apply extra padding. • If the ankle circumference measures >25cm, a different bandage system or additional bandages may be required. • Seek advice from the Tissue Viability Service if required. 2.6 Wound Management The approach to wound management can vary depending on the aetiology of the leg ulceration. 2.6.1 Arterial Ulceration Arterial ulcers may need to be dressed as frequently as daily to facilitate the regular viewing of the limb because of the high risk of wound infection and/or rapid deterioration. In this group of wounds, the usual approaches to maintaining a moist wound healing do not always apply as this can increase the risk of infection by making the surrounding tissue too moist. The care plan should aim to achieve a wound bed that is dry rather than wet. Allow dry necrotic tissue to auto-debride rather than adding Hydrogel to moisten. 2.6.2 Venous ulceration It is more important to provide appropriate compression than to be concerned about the primary wound contact layer; therefore, usually a non or low adherent primary dressing will suffice. Dressing changes can be once weekly or more frequently if exudate level is high. 2.6.3 Mixed Venous/Arterial Ulceration The choice of wound management will vary depending on the degree of arterial involvement. Refer to the Tissue Viability Service if advice required. 2.6.4 Wound Cleansing and Skin Care • Wash hands with liquid soap and water/use alcohol gel prior to undertaking any wound care and wear disposable latex-free gloves and disposable plastic apron. • Cleanse the lower limb by immersion in warm tap water in an appropriate clean bucket or bowl with a plastic liner. Run the tap for 15 seconds before filling the bucket or bowl to avoid contamination from the tap. Emollient can be added to the water if required. Refer to the Brighton and Hove or West Sussex Wound Formularies for product details. • Pat dry with a clean paper towel. Do not rub or traumatise the wound. • If immersion is not possible, irrigate the wound with warmed normal saline. • Gently remove any plaques of skin that may otherwise act as pressure points below compression bandaging. • Apply emollient to lower leg and foot to moisturise skin, e.g. 50% white soft paraffin/50% liquid paraffin (50:50 ointment), or Cetraben cream. • Refer to section 2.8.1 on Infection for decontamination of equipment details. Page 7 of 32 Excellent care at the heart of the community Management of Leg Ulceration for Adults Policy 2.7 Management of Varicose Eczema Avoid use of soap when washing the limb and apply emollients regularly to moisturise the skin. Apply emollients in the direction of hair growth to avoid folliculitis. Refer to the Tissue Viability Team for advice if the following strategies are not successful. 2.7.1 Dry Varicose Eczema This can usually be resolved by appropriate wound cleansing, regular application of ointments and regular removal of dry skin plaques. 2.7.2 Wet or Weeping Varicose Eczema The objective is to return skin to normal through excellent skin care, using bath oil, topical emollients and steroids. Refer to the Brighton and Hove and West Sussex Wound Formularies for further information on products available for skin care. • If Potassium Permanganate is to be used: Soak the affected area daily for a maximum of 10-15 minutes in a solution of potassium permanganate, for up to 2 weeks. Tablet should be diluted 1:10,000 (i.e. 1 tablet in 4 litres of warm water). As the tablet takes a long time to dissolve it is helpful to dilute this first in a small quantity of hot water before adding the remaining water. The final solution should be pale pink in colour. If no improvement has occurred in the first week of treatment, or if deterioration occurs, discontinue treatment. See Waste Management policy at http://thepulse/downloads/trustwide-policies-procedures/estatesfacilities/waste-management.pdf or flow chart at http://thepulse/downloads/trustwidepolicies-procedures/estates-facilities/waste-management.pdf Topical Steroids can be helpful to calm irritation and should be used as a treatment over several weeks with a care plan to reduce the frequency of application to avoid a rebound effect. Apply emollient to the limb and allow this to absorb for a while. Apply three fingertip units (FTU) over the lower leg (add 1 fingertip unit if the foot also affected). Use a moderate potency ointment (e.g. Eumovate™ or Betnovate RD™) daily for 1 week, alternate days for 1 week, twice weekly for 1 week then once the following week before discontinuing. See appendix E for details of FTU dosage measurement. 2.8 Management of Infection and Infection Control Refer to the current Infection Prevention & Control Policy and associated procedures on the Pulse for advice on prevention of spread of infection. Ensure Standard Infection Control principles are used. See the procedure at http://thepulse/downloads/trustwide_policies_procedures/infection_prevention_control/ipc1 _standardinfectioncontrol.pdf 2.8.1 Diagnosis and Treatment of Wound Infection The majority of bacteria found in venous ulcers are simply commensal organisms that do not cause clinical infection. Patients can be inappropriately prescribed antibiotics if clinical infection is not present leading to less effective use of antibiotics when needed or Clostridium difficile infection (Cdiff). Only if clinical signs of infection of the wound or leg Excellent care at the heart of the community Page 8 of 32 Management of Leg Ulceration for Adults Policy are observed (redness, increased pain, increased exudate, pyrexia and/or inflammation) would a wound swab be required, unless there are any other good reasons for suspecting a hidden clinical infection, e.g. wound deterioration or failure to progress despite appropriate holistic management. N.B. All bedded units undertake routine MRSA screening of patients on admission. Prescribed systemic antibiotics should be used to treat diagnosed infection. Short courses are sometimes inadequate due to the poor perfusion of the drug into infected tissue. Topical antibiotics can lead to contact sensitivity and resistance. It may be appropriate to use topical antimicrobial dressings (e.g. iodine, silver or honey) in conjunction with systemic antibiotics. These dressings must be reviewed at regular intervals. Refer to the Brighton and Hove or West Sussex Wound Formularies for further details. 2.8.2 Use of Equipment and dressing materials Scissors • Cutting primary dressings – must be sterile single use and dispose of into sharps container. • Cutting outer bandaging – non-sterile single patient use – cleanse with detergent wipe followed by alcohol wipe. Store dry. Leg ulcer buckets - must be lined with a plastic bag and cleaned with detergent and water/detergent wipe after every use. • In leg ulcer clinics, decontaminate buckets with 1000 ppm available chlorine i.e. Chlorclean wipes. Discard bucket if surface becomes scratched and difficult to clean. • Water must be disposed of down a designated sink or toilet, taking care to avoid splashing. Never dispose of down a hand washing sink. • Clean dry buckets need to be stored upside down in accordance with infection control guidelines. 2.9 Elevation and Exercise All patients should be advised to improve their calf muscle pump (see appendix F for details). 2.9.1 Venous Disease To reduce oedema and improve the venous circulation, patients should be advised to elevate their limbs to above the height of their hip when sitting or lying. Wherever possible, patients should have the foot of the bed elevated on blocks for night use and be encouraged to rest on the bed during the day. The prescription of riser recliner chairs is not deemed an appropriate solution to achieve the recommended level of elevation. Consideration needs to be given to the impact on raising the foot of the bed on functional abilities to transfer in and out.For iCES Brighton and Hove follow this link http://thepulse/downloads/patient-care/clinical-services/ices/ices/catalogue/criteria-riserreclinerchairprovision.pdf Page 9 of 32 Excellent care at the heart of the community Management of Leg Ulceration for Adults Policy Walking with normal heel/toe gait and regular exercises to improve the calf muscle pump function are also helpful and the patient should be encouraged to practice these several times daily.See Appendix E. 2.9.2 Arterial Disease Patients with arterial disease will find it more comfortable to have their legs dependent and it may be helpful to consider raising the head of the bed. If the patient experiences pain that wakes them during the night, then hanging the limb(s) from the side of the bed will help to alleviate this pain. 2.9.3 Mixed Venous/Arterial Disease When there is mixed venous/arterial disease present, positioning of the limb will be determined by patient comfort and the degree of oedema present. It may be necessary to advise a mixture of elevation and dependency determined by the patient’s pain levels. 2.10 Referral for Further Advice 2.10.1 Sussex Community NHS Trust Tissue Viability Service • North and Coastal localities – in the first instance refer via One Call • Brighton and Hove – Refer by faxing a referral form to 01273 242214 or by e-mail to [email protected]. A patient should be referred to Tissue Viability if: • The aetiology is unclear. • The patient is not able to follow the best practice advice given in this document. • There is no improvement in the leg ulcer after 12 weeks of appropriate treatment. • Any support or advice about wound care is required. Brighton & Hove Leg Ulcer Clinics – ambulant patients, suffering from venous leg ulcers only, who are registered with a Brighton & Hove GP practice can be referred to the Community Leg Ulcer Clinics in the city if their own practice does not provide a leg ulcer service under the Local Enhanced Service agreement with the commissioners. Referral via fax to 01273 265899. Brighton Vascular Assessment Unit (VAU) – patients who are registered with a Brighton & Hove GP practice can be referred to the VAU for investigations if: • Doppler readings are unobtainable in the home or clinic environment and/or the patient requires further investigation in the Vascular Assessment Unit. • There is evidence of arterial calcification demonstrated by incompressible or falsely high (>1.3) ABPI readings. • N.B. The VAU will only accept referrals from GPs, Tissue Viability Service and Leg Ulcer Clinic Lead Nurses. The VAU will not accept a referral for ABPI’s if the patient Excellent care at the heart of the community Page 10 of 32 Management of Leg Ulceration for Adults Policy has been assessed by them in the previous 12 months and a normal ABPI was reported. • SCT Venous Leg Ulcer Service (VLUS) – refer via One Call North. Clinics held in a number of locations. Refer by GP/Practice Nurse/Podiatrist or any other health care professional. 2.10.2 Vascular Surgical Departments A patient can be referred for consultant vascular advice via the GP if: • Clinical assessment and Doppler readings of between 0.5 and 0.8 suggest arterial disease – routine referral. • Clinical assessment and Doppler readings of <0.5 suggest severe arterial disease – urgent referral. • Critical limb ischaemia is suspected – emergency referral via A&E. • Doppler readings show an ABPI above 1.3 and further advice is required. • There is marked or sudden deterioration in either the condition of the foot or leg, or the ulcerated area. • There is uncontrolled pain where other causes of pain have been eliminated. • The patient has venous disease that may be improved by venous surgery i.e. with competent deep veins and incompetent superficial veins. Determine whether the patient wishes to be considered for surgery prior to making this referral. 2.10.3 Dermatology Department It is recommended that a patient should be referred for consultant dermatology advice via the GP if: • The patient has venous disease that is not improving after 6 months of appropriate compression therapy and Tissue Viability advice has been sought. • The ulcer appears abnormal or is in an unusual site (i.e. other than the gaiter region). A biopsy may be necessary to exclude skin cancer. • There is marked or sudden deterioration in the condition of the leg, or the ulcerated area, and the ABPI does not indicate arterial disease. • The patient has associated varicose eczema, allergy, or other skin problems that are complicating treatment – patch testing may be required. 2.11 Prevention of Ulcer Recurrence • Surgical correction or sclerotherapy of superficial venous reflux can prevent recurrence – refer for Vascular opinion. • Measure the patient for prescription of compression hosiery. Ideally, class II should be used, but if not tolerated by the patient, try class I or liners. If the measurements do not fit into the normal range of ready-made stockings, prescribe made to measure hosiery. Page 11 of 32 Excellent care at the heart of the community Management of Leg Ulceration for Adults Policy • Hosiery is available in British Standard and European classifications on prescription. The level of compression differs between these classifications therefore consider this when recommending a prescription. • Hosiery can be worn day and night, or be removed at night if preferred. • Stockings should be replaced every three - six months as they lose some of their elasticity after this time. This is an ideal opportunity to reassess the limb, check the skin and reinforce advice. • Continue to elevate the leg at night with bed blocks. 2.12 Smoking Smoking can affect the wound healing process regardless of aetiology. Patients with arterial disease are particularly affected by the effects of smoking and should be encouraged to cease smoking as part of their treatment plan. 3. RESPONSIBILITIES The Chief Executive has ultimate responsibility for the organisation and is supported by the Executive Directors. The policy author is responsible for ensuring the policy follows the appropriate Trust format and complies with the recognised development, consultation, approval and ratification process. Service managers/team leaders are responsible for promoting and implementing the policy. All staff are required to complete in full and as directed any templates or proformas as instructed, for use as part of this policy. 4. ASSOCIATED DOCUMENTS AND REFERENCES • Best Practice Compression therapy Available at http://www.wounds-uk.com/bestpractice-statements/best-practice-statement-compression-hosiery-1 (February 29th 2012) • Britton, J. 2003. The use of emollients and their correct application. Journal of Community Nursing. 17(9):22-25 • Best Practice in Emmolient Therapy 2007. A statement for Healthcare Professionals.Dermatology UK. • Elson D.20009. Potassium Permanganate revisited. Leg Ulcer Forum Journal Issue 23 Autumn 2009. • European Wound Management Association. 2003. Position Statement – Understanding compression. Medical Education Partnership.Ltd London. Excellent care at the heart of the community Page 12 of 32 Management of Leg Ulceration for Adults Policy • Moffatt, C. 2004. Four-layer bandaging: from concept to practice part 1: The development of the four-layer system. Available from http://www.worldwidewounds.com/2004/december/Moffatt/Developing-Four-LayerBandaging.html (February 29th 2012) • Moffatt, C. 2005. Four-layer bandaging: from concept to practice part 2: Application of the four-layer system. Available from http://www.worldwidewounds.com/2005/march/Moffatt/Four-Layer-Bandage-SystemPart2.html (February 29th 2012) • Moffatt, C. 2006. Four-layer bandaging: from concept to practice part 3: Evidence base for treating venous leg ulcers. Available from http://www.worldwidewounds.com/2006/june/Moffatt/Four-Layer-Bandage-SystemPart3.html (February 29th 2012) • Royal College of Nursing. 2006. Clinical Practice Guidelines – The nursing management of patients with venous leg ulcers. London • The National Eczema Society. 1998. Topical Steroids. London. • Thomas, S. 1997. Compression bandaging in the treatment of venous leg ulcers • World Wide Wounds. http://www.worldwidewounds.com (February 29th 2012). • Thomas, S. 2002. The use of Laplace equation in the calculation of sub-bandage pressure. World Wide Wounds. Available from http://www.worldwidewounds.com/2003/june/Thomas/Laplace-Bandages.html (February 29th 2012) • Thomas, S. 2003. An evaluation of a new type of compression bandaging system. Available from http://www.worldwidewounds.com/2003/september/Thomas/NewCompression-Bandage.html February 29th 2012) • Vowden, P. and K. Vowden. 2001. Doppler assessment and ABPI: Interpretation in the management of leg ulceration. Available from http://www.worldwidewounds.com/2001/march/Vowden/Doppler-assessment-andABPI.html (February 29th 2012) • World Union of Wound Healing Societies (WUWHS) Principles of best practice: Compression in venous leg ulcers. A consensus document. London MEP Ltd 2008. • Flanaghan Madeleine. Wound Healing and Skin Integrity. 2013 Wiley-Blackwell. • NICE clinical guidance, 2013. Varicose veins in the legs. Available from http://www.nice.org.uk/guidance/cg168 5. MONITORING COMPLIANCE The Tissue Viability Service in conjunction with the Clinical Service Managers will carry out audit at regular intervals to monitor compliance Page 13 of 32 Excellent care at the heart of the community Management of Leg Ulceration for Adults Policy 6. DISSEMINATION AND IMPLEMENTATION This policy will be made available on the intranet, and publicised through Contact (the Trust internal electronic newsletter). 7. CONSULTATION, APPROVAL, RATIFICATION & REVIEW Trust Community Nursing Team leaders, Tissue Viability Team and The Infection Prevention Team have been consulted The policy will be reviewed 2 yearly 8. VERSION CONTROL Record of Changes Date Version 12/011/14 6.0 27.11.14 6.1 Changes / Comments Changes in response to feedback Excellent care at the heart of the community Page 14 of 32 Management of Leg Ulceration for Adults Policy APPENDIX A Patient label or name LEG ULCERATION DIFFERENTIAL DIAGNOSIS ASSESSMENT FORM Date of Assessment Time of Assessment Name of Assessor Signature of Assessor Date of Birth ID Number Medical alert/allergies/hypersensitivities Venous Risk Factors Abdominal surgery Multiple pregnancies (3+) Sedentary occupation Pulmonary embolism Deep vein thrombosis Thrombophlebitis Leg/hip/foot fracture Cellulitis Leg vein surgery Previous venous leg ulceration Venous Signs & Symptoms Varicose veins Pigmentation (staining) Induration (hardness in skin) Lipodermatosclerosis Oedema Atrophe blanche Ankle flare Cellulitis Palpable pedal pulses Fixed ankle joint Itching over varices Eczema Ulcer in gaiter area Aching / heaviness in legs Warm foot Random Blood Sugar Wound swab YES R R R R R R NO L L L L L L R R R R R R YES R R R R R R R R R R R R R R R L L L L L L NO L L L L L L L L L L L L L L L R R R R R R R R R R R R R R R Arterial Risk Factors Diabetes Ischaemic heart disease Myocardial infarction Transient ischaemic attack Stroke Smoker Angina Hypertension Arterial surgery Rheumatoid arthritis Intermittent claudication Peripheral vascular disease Arterial Signs & Symptoms Loss of hair on leg Muscle wasting Atrophic / shiny skin Thickened toe nails Cool / cold foot Foot / toes blanche when Pain in foot when elevated Pain relieved when dependent Red / blue / purple colour Delayed capillary refill time Ulcers on toes / foot Gangrene on toes / foot Palpable pedal pulses Oedema L L L L L L L L L L L L L L L Other Investigations FBC x-ray HbA1c General Assessment Issue Does the patient go to bed at night? Is the foot of the bed elevated? Is the head of the bed elevated? Does the patient elevate their legs during the day? Does the patient have to hang legs out of the bed during the night? Does the patient have mobility issues? Is the patient able to walk heel to toe (i.e. normal gait)? Can the patient dorsiflex / planterflex the ankle? Can the patient circle the ankle? Page 15 of 32 Excellent care at the heart of the community YES NO R R R R R R R R L L L L YES R R R R R R R R R R R R R R U/E Other YES L L L L L L L L L L L L L L L L L L NO R R R R R R R R R R R R R R L L L L L L L L L L L L L L NO Management of Leg Ulceration for Adults Policy Patient label or name Date of Assessment Time of Assessment Date of Birth Name of Assessor Signature of Assessor ID Number Arterial Assessment using Doppler Ultrasound Length of resting prior to procedure Position during procedure 20 mins Flat Locate pulses and record quality of sound Identify both brachial pulses and two pedal pulses on each foot (use highest for calculation) Pulse Name Brachial Artery Dorsalis Pedis Artery Posterior Tibial Artery Anterior Tibial Artery Peroneal Artery Right Ankle Brachial Pressure Index (ABPI) < 5 mins Upright Sound = Triphasic (T); Biphasic (B); Monophasic (M) Palpable Y N Y N Y N Y N Y N Right 15 mins 10 mins Semi-recumbent Sound T B T B T B T B T B Left M M M M M Palpable Y N Y N Y N Y N Y N Sound T B T B T B T B T B M M M M M Left Nursing Diagnosis of Leg Ulcer Aetiology Venous Arterial Mixed Venous / Arterial Other (assess further) Treatment Decision Full Compression Reduced Compression (10 R L R L No Compression R L (40mmHg) – 30mmHg) Ankle circumference Right cm Left cm Limb Measurements for Compression Hosiery Right Leg centimetres Left Leg centimetres Length of foot Length of foot Ankle circumference (narrow point) Ankle circumference (narrow point) Calf circumference (widest point) Calf circumference (widest point) Thigh circumference (widest point) Thigh circumference (widest point) Back of knee to bottom of heel Back of knee to bottom of heel Further Action Needed For Pulse Oximetry For referral to Tissue Viability Specialist For referral to Vascular Specialist For referral to Dermatology Other Information Patient information leaflet given Yes / No Verbal information given Excellent care at the heart of the community Yes / No Page 16 of 32 Management of Leg Ulceration for Adults Policy LEG ULCERATION – WOUND ASSESSMENT FORM Patient label or name Date of Assessment Time of Assessment Date of Birth Name of Assessor Signature of Assessor ID Number Medial View Map Position of Ulcers Posterior View Anterior View Lateral View Left Leg Right Leg Record description Sloping/Beached Rolled over Deep/Cliff of ulcer edge Record condition of Dry eczema Wet Eczema Macerated surrounding skin Use generic wound assessment form for details of size, wound tissue, odour, exudate level etc. Page 17 of 32 Excellent care at the heart of the community Management of Leg Ulceration for Adults Policy APPENDIX B DOPPLER ULTRASOUND PROCEDURE This procedure must be carried out only by clinical staff that have been trained to undertake it, have been assessed as competent and have knowledge of how to interpret the results. Equipment • Couch or bed to enable patient to lie down. • Cover any existing wounds with a sterile dressing. • Appropriate sized blood pressure cuff, single patient use or disposable advised if used over a wound and is available. • Sphygmomanometer. • Ultrasound Gel. • Hand-held Doppler. • 8 mHz probe. • 5 mHz probe for oedematous limbs. • Calculator or ABPI reference chart. • Liquid soap and water • Disposable latex-free gloves and disposable plastic apron Use the Doppler ultrasound machine to measure brachial and ankle systolic pressures (do not use a stethoscope). An 8 mHz probe will be adequate in most circumstances but it may be necessary to use a 5 mHz probe for those patients with oedematous feet. Pedal Pulses The pulses commonly located for ABPI measurement are the dorsalis pedis and the posterior tibial but either the anterior tibial or the peroneal could be used if the other two are difficult to locate. It should be noted, however, that the dorsalis pedis and the anterior tibial are different pulse locations on the same artery. Excellent care at the heart of the community Page 18 of 32 Management of Leg Ulceration for Adults Policy Preparation of the Patient • Ensure the patient is lying flat (or as flat as possible) and is rested. • If the patient is not able to lie completely flat, elevate the legs to the level of the heart. • Explain the purpose of carrying out this procedure and what will be happening to them. • Ensure that a full leg ulcer assessment has been carried out to obtain information about the patient’s medical history, signs and symptoms and presenting factors. Measure the brachial systolic blood pressure • Wash hands with liquid soap and water • Put on disposable latex-free gloves and disposable plastic apron if wound present • Place an appropriately sized cuff around the upper arm (the bladder part of the cuff should cover ¾ of the arm circumference). • Ensure the equipment and arms are at heart level, with the patient rested and supine. • Locate the brachial pulse and apply ultrasound contact gel. • Angle the Doppler probe at 45º and move it to obtain the best signal. • Inflate the cuff until the signal is abolished; then deflate the cuff slowly and record the pressure at which the signal returns, being careful not to move the probe from the line of the artery. • Repeat the procedure on the other arm. • Use the higher of the two values as the best estimate of central systolic pressure to calculate the ABPI. • Measure the ankle systolic pressure. • Place an appropriately sized cuff around the ankle above the malleoli, having first protected any ulcer or fragile skin that may be present with a sterile dressing. • Examine the foot, locate the dorsalis pedis pulse and apply contact gel. • Angle the Doppler probe at 45º and move it to obtain the best signal. • Inflate the cuff until the signal is abolished; then deflate the cuff slowly and record the pressure at which the signal returns, being careful not to move the probe from the line of the artery. • Repeat on the posterior tibial artery, and if required, the peroneal and / or anterior tibial arteries. • Use the highest reading obtained to calculate the ABPI for that leg. • Repeat on the other leg regardless of where ulcers are located to obtain a complete picture. • Remove protective clothing and wash hands with liquid soap and water • Calculating the Ankle Brachial Pressure Index (ABPI). Page 19 of 32 Excellent care at the heart of the community Management of Leg Ulceration for Adults Policy The ABPI is then calculated by dividing the ankle systolic pressure by the brachial systolic pressure using a chart or calculator: ABPI = Highest pressure recorded at the ankle for that leg Highest brachial pressure obtained for both arms Interpretation of Doppler readings • A ratio of 1.3 or above could indicate arterial calcification (see paragraph below). National and European guidelines recommend: Do not compress. • A ratio of 1.0 indicates normal arterial blood flow, full compression can be applied safely. • A ratio of 0.9 or 0.8 indicates a mild degree of arterial disease, but full compression can still be applied. • A ratio of < 0.8 indicates significant arterial disease. Referral to the Vascular Department for further investigation is recommended. Do not use compression therapy unless reduced compression is prescribed by a specialist nurse or medical practitioner. • A ratio of 0.5 indicates severe arterial disease. An urgent referral to the Vascular Department is required. Do not use compression therapy. Frequency of Reassessment of Ankle Brachial Pressure Index Ideally it is recommended that the Doppler procedure is repeated for all patients with leg ulceration at 3 monthly intervals as there is evidence that significant reductions in ABPI can occur over relatively short periods of time (3-12 months) and ABPI will also fall with age. However, this standard can be reduced to 6 monthly intervals for those patients who show no clinical signs of developing or deteriorating arterial disease. Arterial Calcification Accurate calculation of ABPI is dependent on the ability to compress the artery with the cuff during the procedure. If the arteries are calcified they will be rigid and therefore not compressible. This may give rise to a false high reading. Small vessel arterial disease may be present and compression therapy may not be appropriate. Brighton and Hove Further investigation is indicated and this can be requested via the Non-Invasive Vascular Laboratory at Royal Sussex County Hospital (664650 or ext. 4084). West Sussex: Patients should be referred via their GP to the Vascular Service. Excellent care at the heart of the community Page 20 of 32 Management of Leg Ulceration for Adults Policy Problems and Errors Problems and errors can arise if: • The cuff is repeatedly inflated or inflated for long periods – this can cause the ankle pressure to fall. • The cuff is not placed at the ankle – the pressure recorded may be higher than the true ankle pressure. • The pulse is irregular or the cuff is deflated too rapidly – the true systolic pressure may be missed. • The vessels are calcified, the legs are large, fatty or oedematous, the cuff size is too small, or the legs are dependent – an inappropriately high reading will be obtained. Difficult to obtain Doppler readings On a small number of patients it may not be possible to obtain accurate readings using this procedure in the patients normal care environment or with the hand-held equipment. In these cases further investigation is indicated and a referral should be made as below. Brighton and Hove Non-Invasive Vascular Laboratory specifying the aetiology as determined from clinical assessment and the difficulties encountered with the Doppler procedure. Vascular Assessment Unit – Royal Sussex County Hospital (664650 or ext. 4084). West Sussex Referral should be made to the Tissue Viability Service. Page 21 of 32 Excellent care at the heart of the community Management of Leg Ulceration for Adults Policy APPENDIX C EXAMPLES OF BANDAGE AND COMPRESSION SYSTEMS ON BRIGHTON AND HOVE AND WEST SUSSEX WOUND CARE FORMULARY 1. Full Compression – 40 mmHg at ankle Four-Layer Bandage System Ankle measurement 18-25cm • K-Four Bandage Kit. • K-Soft, K-Lite, K-Plus and Co-Flex. Two-Layer Bandage Systems • K-Two Bandage System –measure ankle circumference to ensure the correct kit is chosen. Short-stretch Bandage System Ankle measurement 18-25cm • K-Soft/Flexiban and Actico Cohesive (100% tension). Hosiery System • 2. Activa 40 mmHg Hosiery Kit. Reduced Compression – 17 – 23 mmHg at ankle • K-Soft, K-Lite and K-Plus = 17 mmHg pressure at ankle. • K-Soft, K-Lite and Ko-Flex – 23 mmHg pressure at ankle. 3. Retention Bandage – no compression • K-Soft and K-Lite –West Sussex. • K-Soft and Elastocrepe – Brighton and Hove. • K-Soft and Setocrepe – Brighton and Hove. • K-Band – West Sussex. Excellent care at the heart of the community Page 22 of 32 Management of Leg Ulceration for Adults Policy APPENDIX D FINGER TIP UNITS One finger tip unit is equal to the amount of cream which is placed on the tip of the finger as illustrated below:- Please note: Ungloved hand for demonstration purposes only Topical Steroids can be helpful to calm irritation and should be used as a treatment over several weeks with a care plan to reduce the frequency of application to avoid a rebound effect. Wash hands/use alcohol gel and apply gloves. Apply patient designated emollient to the limb and allow this to absorb for a while. Do not use the same pot/tube for multiple patients. Dispense steroid to a tray or single use spatula and apply three finger tip units over the lower leg (add 1 finger tip unit if the foot also affected). Use a moderate potency ointment (e.g. Eumovate™ or Betnovate RD™) daily for 1 week, alternate days for 1 week, twice weekly for 1 week then once the following week before discontinuing. Page 23 of 32 Excellent care at the heart of the community Management of Leg Ulceration for Adults Policy APPENDIX E ANKLE EXERCISES TO AID LOWER LIMB CIRCULATION When sitting or lying – flexing the foot. When sitting or lying – rotating the ankle. When standing – move up and down on your toes. Excellent care at the heart of the community Page 24 of 32 Equality Analysis 9. EQUALITY ANALYSIS The Trust aims to design and implement services, policies & other procedural documents and measures that meet the diverse needs of our service, population and workforce, ensuring that none are placed at a disadvantage over others. Under the Equality Act 2010, policy or other procedural document authors have a statutory duty to give “due regard” to issues of race, disability, gender (including transgender), religion or belief, age, sexual orientation and human rights when developing their policy or other procedural document. This means that policy or other procedural document authors have to assess the potential for their document to discriminate on any of these grounds. Alternatively, the impact of the policy or other procedural document on these groups might be positive or the same for everyone. 1 Name of Policy or Service Management of Leg Ulceration for Adults Policy 2 Service and Tissue Viability. Adult Services Directorate 3 Objectives This document will outline the Trust’s expectations of staff involved in treating patients with leg ulceration and will offer guidelines on how to approach the patient’s treatment plan. What is the purpose of this policy or service? Page 25 of 32 Excellent care at the heart of the community 4 Analysis completed By a) Name b) Title Jane Saunders Tissue Viability Nurse Specialist 5 Does the policy or service have an effect on Staff and/or the Public? (please √) Staff Yes No Public Yes No Excellent care at the heart of the community Page 26 of 32 Equality Analysis Equality law protects people on the following grounds: Is your policy or service relevant to this area of equality or human rights? Yes No If relevant, is the effect positive or negative Positive Evidence of the effect (e.g. statistics, research, surveys, results of engagement, etc) Negative effect Is further action required? *Yes No effect Age Disability Gender (including pregnancy and maternity) Transgender Race and Ethnicity Page 27 of 32 Excellent care at the heart of the community The effect of this policy is the same on all groups Religion and Belief Sexual Orientation (including civil partnership) Human Rights * Complete the following Equality Analysis Action Plan only for equality grounds marked: *Yes further action required. Excellent care at the heart of the community Page 28 of 32 Equality Analysis Equality Analysis Action Plan Equality grounds Does your policy or service: Any action taken Action to be taken to date Target date ticked *Yes Discriminate? requiring further action: Page 29 of 32 Eliminate discrimination or promote equality? Promote good relations between groups? Excellent care at the heart of the community Responsible Person(s) Expected Outcome (including monitoring arrangeme nts) Equality Analysis: Equality and Diversity Lead sign off Signed Jourdan Durairaj (Equality and Diversity Lead) Date 26 November 2014 Excellent care at the heart of the community Page 30 of 32 10. RATIFICATION CHECKLIST Trustwide Clinical Governance Group. Agenda Item: The meeting administrator should be able to provide this Policy Title Management of Leg Ulceration for Adults Policy Policy Author Jane Saunders Presented By Purpose Ratification Checklist for Ratification 1 Format Yes Has the standard SCT template been used? 2 Comments: Consultation Please identify who has been consulted in the writing of this document :Clinical Nurse Mangers Senior Locality Nurses Community Nursing Team Leaders Tissue Viability Nurses Infection Prevention team 3 Does the committee agree that the right people been consulted with? Yes/No (please delete) Comments Does anybody else need to be consulted prior to ratification: No Please state who: Approval Please state the name of the Group that has approved this document? Date of Group Approval Trustwide Clinical Governance Group. th Date: 25 November 2014 Page 31 of 32 4 Equality Analysis Has the Equality Impact Assessment been completed? 5 Yes Comments Review Please state the timescale for review: 2 yearly For completion by the Chair of the Committee Policy Ratified Yes / No (please delete) Signature of Chair (Executive Director) (Print Name): Dr Richard Quirk – Medical Director / Susan Marshall – Chief Nurse Additional actions required for ratification: Excellent care at the heart of the community Page 32 of 32