Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
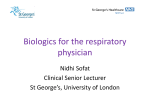
Pyoderma gangrenosum in Crohns disease Infliximab for Treatment of Pyoderma Gangrenosum Associated with Clinically Inactive Crohns Disease. A Case Report George Kouklakis1,2, John Moschos1,3, Grigoris I. Leontiadis3, Savvas Kadis3, Alexandros Mpoumponaris1, Epaminondas Molyvas1, George I. Minopoulos2 1) 424 General Army Hospital, Thessaloniki. 2) Medical School Democritus University of Thrace, Alexandroupolis, Greece. 3) Queen Elizabeth Hospital, Gateshead, UK Abstract We report the case of a 57-year old female patient with refractory to treatment pyoderma gangrenosum associated with clinically inactive Crohns disease. Pyoderma gangrenosum was successfully treated with Infliximab, a chimeric monoclonal antibody that inhibits tumour necrosis factor alpha (TNF-α). Our case report suggests that Infliximab, a therapeutic agent for refractory and fistulizing Crohns disease, may also be safe and effective in the treatment of Crohns disease associated pyoderma gangrenosum, even though the inflammatory bowel disease is clinically inactive and repeated infusions may be required for successful treatment. Key words Crohns disease - pyoderma gangrenosum - Infliximab Rezumat Prezentãm cazul unei femei de 57 de ani cu pyoderma gangrenosum refractar la tratament, asociat cu boalã Crohn clinic inactivã. Pyoderma gangrenosum a rãspuns la administrarea de Infliximab, anticorp monoclonal chimeric care inhibã factorul de necrozã tumoralã alfa (TNF-α). Acest caz sugereazã cã Infliximab, administrat în boala Crohn refractarã ºi complicatã cu fistule, poate fi eficace ºi sigur în boala Crohn asociatã cu pyoderma gangrenosum, chiar dacã boala inflamatorie intestinalã este asimptomaticã. Pentru succesul terapeutic pot fi necesare mai multe administrãri. bowel disease (IBD). The treatment of PG is rather empirical and is based on clinical experience. It includes local therapies and immuno-modulating agents. Infliximab (Remicade ®), a chimeric monoclonal antibody that inhibits tumour necrosis factor alpha (TNF-α), has been successfully used to treat patients with moderate to severe and fistulizing Crohns disease (CD) (1). Several case reports and retrospective reviews of case series suggest that Infliximab may induce healing of PG lesions in patients with IBD. We present a female patient with quiescent CD involving the small intestine that developed refractory PG, but responded favourably to treatment with Infliximab. Case report A 57-year-old female patient was referred to our outpatient clinic by a dermatologist. She had a large lesion of about 5 cm in diameter on her left lower extremity, diagnosed to be PG (Fig.1). The patient did not report previous trauma to the site of the lesion. The lesion had been refractory to local treatment, corticosteroids and azathioprine. She had a history of several episodes of bloody diarrhoea in the past, for which she had not sought medical advice. Introduction Pyoderma gangrenosum (PG) is an inflammatory exulcerative skin lesion that may complicate inflammatory Romanian Journal of Gastroenterology December 2005 Vol.14 No.4, 401-403 Address for correspondence: John Moschos MD PhD Papadimitriou 10 55131, Kalamaria, Greece Email: [email protected] Fig.1 Pyoderma gangrenosum, associated with clinically inactive Crohns disease. 402 She had a normal colonoscopy but the terminal ileum biopsies were diagnostic of Crohns disease. The patient received three i.v. infusions of Infliximab at a dose of 5 mg/kg at 0, 2 and 8 weeks, respectively. Infliximab was administered solely for the PG lesion since she had no active or fistulizing CD. The patient was able to taper off corticosteroids completely and thereafter did not require additional corticosteroid treatment. Infliximab was well tolerated with no adverse effects. Following the first infusion there were signs of improvement and after the third infusion the lesion healed completely. After one year, the lesion remains completely healed. Discussion Pyoderma gangrenosum (PG) is an inflammatory condition that is characterized by development of chronic ulcerative skin lesions preferentially on the lower extremities. About 36-50% of patients with PG have IBD. Conversely, PG occurs in about 1-2% of patients with IBD and may bear no relation to the clinical activity of the intestinal disease as in our patient, in whom the IBD was clinically inactive (2) . However, clinical experience implies that PG associated with CD heralds active intestinal inflammation, even if symptoms of the gut are not overt initially (3). The pathogenesis of PG is unknown. It is suggested that an aberrant immune system is central to the pathogenesis of this disease and thus, effective long term management of PG will involve sustained control of systemic and local inflammation by alteration of the immune system. PG treatment includes local wound care in conjunction with systemic treatment with immunomodulating agents. Local therapies comprise topical pharmacological treatment, dressings and intralesional injection of corticosteroids or cyclosporine. Systemic immuno-modulating agents include corticosteroids, azathioprine, 6-MP, alkylating agents and cyclosporine. The high doses of corticosteroids needed to treat PG have been associated with significant side effects (4). A variety of other agents have been used, including tacrolimus, hyperbaric oxygen, mycophenolate mofetil, dapsone and plasmapheresis. There have been no prospective randomised controlled trials on any treatment. For extreme intractable cases of PG, surgical intervention may be required (5). Infliximab, a monoclonal antibody that blocks and neutralizes TNF-α. has demonstrated rapid improvement of moderate to severe CD (6) and healing of fistulae in randomised controlled trials (7). It induces endoscopic, clinical as well as histological improvement and has been approved by the FDA for the management of moderate to severe CD and fistulizing CD. Improvement of CDs associated skin lesions and spondylo-arthropathy have also been suggested. There have been several case reports and retrospective studies that suggest that Infliximab may induce healing of PG lesions in patients with CD (4,8-11). There are also reports of successful treatment of ulcerative colitis as- Kouklakis et al sociated PG with Infliximab (12,13). In these reports both skin lesions and bowel disease responded well to Infliximab administration. Improvement of skin lesions occurred soon after the administration of Infliximab, and complete or nearly complete healing was achieved in less than 3 months after the first infusion (14). Whether the positive effect of Infliximab on PG is a result of effective treatment of the intestinal inflammation or of the skin disease is not clear. The outcome of Infliximab treatment in 8 patients with PG associated with IBD was reported by Ljung et al (3). Three of the patients responded with complete healing of PG, defined as skin covering completely the lesion. Three partially responded to Infliximab treatment, which was defined as at least 50% reduction of the diameter of the lesion and two had transitory improvement to Infliximab. Adverse effects as skin rash, pneumonia and diarrhoea were seen in three patients. The authors concluded that the majority of patients with PG benefit from Infliximab treatment with an acceptable occurrence of adverse reactions. In order to achieve full remission, however, repeated treatment is needed (3). In a retrospective study, 13 patients with IBD and medically refractory PG were treated with Infliximab. In three of these patients PG lesions responded to the first Infliximab infusion and did not require additional treatment, but most of the patients required repeated infusions and were ultimately maintained on Infliximab (4). Tan et al reported two patients with PG and fistulizing CD and impressive improvement after the first infusion of Infliximab. PG did recur in both patients but responded to additional therapy with Infliximab (10) . Mimouni et al described their experience in three patients with IBD - associated peristomal PG. Two of them had complete healing of the lesion and one partial response to the drug (15). A 41-year old woman with known CD had a severe and rapidly extensive corticosteroid resistant PG on the leg. Infliximab 5mg/kg was given at weeks 0, 5 and 9. A complete healing was achieved at week 11 (16). Infliximab should be considered for treating PG and other extraintestinal dermatological manifestations in CD even in children (17). The durability of the response to Infliximab remains to be established, and it is uncertain whether the best method of treatment with infliximab is on demand or regularly. The efficacy of Infliximab in many inflammatory diseases has already been reported, but its use in PG has only been seen in a few cases. Our case report suggests that Infliximab is effective and safe therapy for refractory CD-associated PG and should be included in the armamentarium of medicines used to treat this skin lesion. References 1. Baert FJ, Rutgeerts PR. Anti-TNF strategies in Crohns disease: mechanisms, clinical effects, indications. Int J Colorectal Dis 1999;14:4751. 2. Callen JP. Pyoderma gangrenosum. Lancet 1998; 351:581585. Pyoderma gangrenosum in Crohns disease 3. Ljung T, Staun M, Grove O, Fausa O, Vatn MH, Hellström PM. Pyoderma gangrenosum associated with Crohn disease: effect of TNF-alpha blockade with Infliximab. Scand J Gastroenterol 2002;37:1108 1110. 4. Regueiro M, Valentine J, Plevy S et al. Infliximab for treatment of Pyoderma gangrenosum associated with inflammatory bowel disease. Am J Gastroenterol 2003; 98:1821-1826. 5. Alam M, Grossman ME, Schneiderman PI, et al. Surgical management of Pyoderma gangrenosum: case report and review. Dermatol Surg 2000;26:1063-1066. 6. Targan SR, Hanauer SB, van Deventer SJ et al. A short term study of chimeric monoclonal antibody cA2 to tumor necrosis factor alpha for Crohns disease. Crohns Disease CA2 Study Group. N Engl J Med 1997;337:1029-1035. 7. Present DH, Rutgeers P, Targan S et al. Infliximab for the treatment of fistulas in patients with Crohns disease. N Engl J Med 1999;340:1398-405. 8. Zaccagna A, Bertone A, Puiatti P, et al. Anti-tumor necrosis factor alpha monoclonal antibody (infliximab) for the treatment of pyoderma gangrenosum associated with Crohns disease. Eur J Dermatol 2003;13:258-260. 9. Van der Schaar P, Wensveen C, Bavink JNB, et al. Treatment with anti-TNF alpha (Remicade) for Pyoderma gangrenosum in Crohns colitis [Case Report]. Gut 2000;32:Suppl 1, A245. 10. Tan MH, Gordon M, Lebwohl O, George J, Lebwohl MG. Improvement of Pyoderma gangrenosum and psoriasis 403 associated with Crohns disease with anti-tumor necrosis factor alpha monoclonal antibody. Arch Dermatol 2001;137:930 933. 11. Hong JJ, Merel NH, Hanauer SB. Treatment of Pyoderma gangrenosum complicating Crohns disease with Infliximab. Gastroenterolog y 2001;120: Suppl 1, P. A-621. 12. Botros N, Pickover L, Das K. Image of the Month. Pyoderma gangrenosum caused by ulcerative colitis. Gastroenterology 2000;118:654, 809 . 13. Ardizzone S, Bollani S, Colombo E, Bianchi Porro G, et al. Infliximab for the treatment of Pyoderma gangrenosum in steroid dependent ulcerative colitis. Gut 2001;49 Suppl III, Abstr 3190. 14. Triantafillidis JK, Cheracakis P, Sklavaina M, Apostolopoulou K. Favorable response to Infliximab treatment in a patient with active Crohn disease and Pyoderma gangrenosum . Scand J Gastroenterol 2002;37:863865. 15. Mimouni D, Anhalt GJ, Kouba DJ et al. Infliximab for peristomal pyoderma gangrenosum Br J Dermatol. 2003;148:813816. 16. Grange F, Djilali-Bouzina F, Weiss AM et al. Corticosteroid resistant pyoderma gangrenosum associated with Crohns disease: rapid cure with infliximab. Dermatology 2002;205:278-280. 17. Kugathasan S, Miranda A, Nocton J, et al. Dermatologic manifestations of Crohn disease in children: response to Infliximab. J Pediatr Gastroenterol Nutr. 2003;37: 150154.