Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
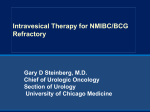
1 1 Development and Spontaneous Resolution of Suppurative Granulomatous Inflammation of Glans Penis Following Intravesical Administration of Bacillus Calmette-Guerin Yu-Hao Chang Chi-Jung Chung Tseng-tong Kuo1 Hong-Shang Hong A 57-year-old male was found to have papillary transitional cell carcinoma of the urinary bladder and underwent a tranurethral resection of the tumor. He suffered from multiple asymptomatic red papules on glans penis after 9 th intravesical therapy with Bacillus Calmette - Guerin ( BCG ). His left inguinal lymph node was enlarged and tender. The skin lesions were found to be due to suppurative granulomatous inflammation. Periodic acid-Schiff stain (PAS) and acid-fast stain (AFS) were negative. The lesions on glans penis and the enlarged inguinal lymph node resolved spontaneously few weeks later. The occurrence of granulomatous cutaneous lesions following BCG therapy is reported. (Dermatol Sinica 22 : 231-234, 2004) Key words: Bacillus Calmette-Guerin (BCG), Glans penis 57 PAS ( AFS 22 : 231 - 234, 2004 ) From the Departments of Dermatology and Pathology,1 Chang Gung Memorial Hospital-Taipei Accepted for publication : February 12, 2004 Reprint requests: Chi-Jung Chung M.D., Department of Dermatology, Chang Gung Memorial Hospital, 199 Tun-Hwa North Road, Taipei, Taiwan TEL: 886-2-27135211 ext. 3397 FAX: 886-2-27191623 231 INTRODUCTION Intravesical therapy with Bacillus Calmette -Guerin (BCG) has proved to be effective in the prophylaxis and treatment of superficial urinary bladder tumors and carcinoma in situ. 1 The increasing use of this treatment has been accompanied by reports of local and systemic complications.2 To our knowledge, only 6 reports of BCG related penile or urethral infection have been published before.3 - 7 We describe a patient with BCG related glans penis granulomatous inflammation following intravesical therapy for a superficial transitional cell carcinoma and review the related literature. CASE REPORT A 57-year-old man with a history of cigarette smoking presented at our outpatient clinic in May 2001 with painless hematuria. Cystoscopy revealed a 0.5 cm papillary tumor at left ureteral orifice. Tranurethral resection of the tumor was performed and the tumor was a grade I transitional cell carcinoma. Intravesical BCG immunotherapy started in June 2001. He received a total of 8 instillations at weekly intervals from June 2001 to September 2001. The course was quite smooth except an episode of cystitis after 7 th instillation. However, several asymptomatic red papules developed on the glans penis 3 days later after the 9 th instillation. The papules were erythematous with 2~3 mm deep - seated white pustules ( Fig. 1 ). Besides, a 2 x 2 cm tender lymph node was noted on the left inguinal area. There were no other abnormalities in physical examinations. A biopsy specimen of the skin lesions showed granuloma with central microabscess in the dermis (Fig. 2a, 2b ). Special stains with Periodic acid - Schiff stain ( PAS ) and acid - fast stain ( AFS ) were negative. His chest X-ray was normal and laboratory tests including a complete blood cell count and blood chemistry were all within normal limits. The test for mycobacterial DNA by polymerase chain reaction was negative. Although only topical antibiotics was prescribed, the lesions spontaneously healed with- Fig. 2a Photomicrography showed a dermal granuloma with central microabscess formation. (H & E, x40) Fig. 1 Fig. 2b The clinical appearance of multiple discrete erythematous papules on the glans penis induced by intravesical immunotherapy with BCG A multinucleated giant cell (arrow) (H & E x400) Dermatol Sinica, September 2004 232 out scarring in two weeks. The left inguinal lymphoadenopathy also resolved later. DISCUSSION BCG is the attenuated strain of bovine bacterium tuberculosis and consists of living bacilli, dead microorganisms and subcellular debris. It is thought to act as a potent stimulator of local cellular immunity.1 Intravesical instillation of BCG has been shown to serve as an effective treatment of and prophylaxis for recurrent stage Ta and T1 tumors and carcinoma in situ. The increased use of this treatment has been accompanied by reports of local and systemic complications. In the study of 2,602 patients by Lamm et al,2 high fever (greater than 39˚C) occurred in 2.9 % of the patients, granulomatous prostatitis in 0.9 %, granulomatous pneumonitis and / or hepatitis in 0.7%, arthralgia in 0.5%, hematuria in 1%, skin rash in 0.3%, ureteral obstruction in 0.3%, epididymitis in 0.4%, contracted bladder in 0.2%, renal abscess in 0.1%, sepsis in 0.4% and cytopenia in 0.1%. In general, 95% of the patients have no serious side effects. Traumatic catheterization or concurrent cystitis is the major risk factor for systemic BCG absorption. BCG related penile or urethral infection was quite rare. To our knowledge only 6 cases have been previously published in the literature. 3-7 The clinical presentations include painful erythematous papules, crusty ulcers, palpable dorsal penile nodules combine with coronal abscess and penile edema associate with meatal ulceration. These cutaneous lesions were noted between 7~15 days following intravesical BCG instillation. Enlarged inguinal lymph nodes were most often noted. Only three cases underwent skin biopsy. Tuberculoid granuloma was the common histopathologic finding. But none of them demonstrated acid - fast bacilli. M. bovisBCG was identified by tissue culture only in two cases and M. tuberculosis was found in the case reported by Konohana et al.3, 5, 7 Under the treatment of combinative antituberculous chemotherapy, the lesions of these 6 cases resolved gradually in few months later. The clinical picture and histopathologic 233 finding in our patient was similar to the case reported by Ribera et al.5 Asymptomatic erythematous papules with central whitish pustules on the glans penis combined with inguinal lymphadenopathy following intravesical immunotherapy were characteristic clinically sufficient to suggest the diagnosis. Because the patient refused another skin biopsy for tissue culture, we tried to examine mycobacterial DNA by polymerase chain reaction. However, the result was negative. According to the study concerning the fate of bacillus Calmette-Guerin after intravesical instillation by Durek et al,8 mycobacterial DNA was found only in 31.8 % bladder biopsies obtained within one week after the last installation. Purified protein derivative (PPD) skin test was not performed in this case unfortunately. The conversion from a negative to positive tuberculin skin test can help to confirm a recent mycobacteria infection. With the clinical charateristics and pathological findings, we favor this is a case of BCG related balanitis after intravesical immunotherapy. The differential diagnosis of similar penis lesions must include lichen nitidus, ectopic sebaceous gland and papulonecrotic tuberculid. Lichen nitidus is composed of discrete smooth, flat, round papules with flesh-colored and glistening appearance. Each papule consists of a well - circumscribed mixed - cell granulomatous infiltrate in an expaned dermal papilla. Ectopic sebaceous glands are asymptomatic yellowish papules on the inner aspect of the prepuce and rarely on the glans penis. Each globoid lesion consists of a group of small but mature sebaceous lobules situated around a small sebaceous duct leading to the surface epithelium. Isrealewicz et al. reported a case of papulonecrotic tuberculid with penis involvement. Penile lesions combined with multiple punchedout scars on the leg was the clinical finding.9 Classically, the infectious complications of BCG therapy were treated with isoniazid 300mg daily. If there was no response, rifampicin 600mg daily was added. The previous 6 reports of BCG related penile or urethral infection were all treated with combination antituberculous Dermatol Sinica, September 2004 chemotherapy. The skin lesions and inguinal lymphadenopathy all resolved gradually. In our case, the lesions healed spontaneously in two weeks although only topical antibiotic was prescribed. Following the management of adverse reactions to BCG vaccination in literature reviews, conservative therapeutic approach is usually adequate. Prescription of isoniazid for the benefit in local abscess resolution is still controversial. Such therapy is only considerated unless there is clear evidence of suppurative reaction associated lymphadenopathy. 10 In a review of incidence and treatment of complications of BCG intravesical therapy of 2602 patients, 300mg isoniazid orally was recommened for 3 months in patients with persistent fever for 12 ~ 24 hours. The combination of 300mg isoniazid , 600mg rifampin and 1200mg ethembutol for 6 months is indicated in patients with systemic side effects or sepsis.2 We report a case of BCG - related balanitis resolved spontaneously without using antituberculous chemotherapy. According to the definition in textbooks, tuberculosis of the skin is caused by M. tuberculosis and M. bovis, including bacillus CalmetteGuerin ( BCG ).11 Although different titles were used in the previous 6 reports of BCG related penile infection, 3 - 7 penile tuberculosis after intravesical bacillus Calmette-Guerin treatment may be a more accurate description. For lacking direct evidence to prove the presence of mycobacteria bovis in skin rash of this case, our title was mainly according to the histopathologic finding. REFERENCE Mechanisms of action of intravesical bacille Calmette-Guerin: Local immune mechanisms. Clin Infect Dis 31: 91-93, 2000. 2. Lamm DL, Morales A, Brosman SA, et al.: Incidence and treatment of complications of bacillus Calmette-Guerin intravesical therapy in superficial bladder cancer. J Urol 147: 596-600, 1992. 3. Konohana A, Noda J, Shoji K, et al.: Primary tuberculosis of the glans penis. J Am Acad Dermatol 26: 1002-1003, 1992. 4. Erol A, Ozgur S, Tahtall N, et al.: Bacillus Calmette-Guerin(BCG) balanitis as a complication of intravesical BCG immunotherapy. Int Urol Nephrol 27: 307-310, 1995. 5. Ribera M, Bielsa J, Manterola JM, et al.: Mycobacterium bovis-BCG infection of the glans penis: a complication of intravesical administration of bacillus Calmette-Guerin. Br J Dermatol 132: 309-310, 1995. 6. Baniel J, Lev Z, Engelstein D, et al.: Penile edema and meatal ulceration after intravesical instillation with bacillus Calmette-Guerin. Urology 47: 932934, 1996. 7. Latini JM, Wang DS, Forgacs P, et al.: Tuberculosis of the penis after intravesical bacillus Calmette -Guerin treatment. J Urol 163: 1870, 2000. 8. Durek C, Richter E, Basteck A, et al.: The fate of bacillus Calmette-Guerin intravesical Installation. J Urol 165: 1765-1768, 2001. 9. Isrealewicz S, Dharan M, Rosenman D, et al.: Papulonecreotic tuberculid of the glans penis. J Am Acad Dermatol 12: 1104-1106, 1985. 10. FitzGerald JM: Management of adverse reaction to bacille Calmette-Guerin vaccine. Clin Infect Dis 31: 75-76, 2000. 11. Tappeiner G, Wolff K: Tuberculosis and other mycobacterial infections. In: Freedberg IM, Eisen AZ, Wolff K et al., eds. Dermatology in General Medicine. 5th ed. New York: McGraw-Hill, 22742292, 1999. 1. Prescott S, Jackson AM, Hawkyard SJ, et al.: Dermatol Sinica, September 2004 234