Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
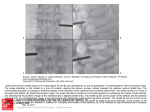
94 J Emerg Crit Care Med. Vol. 24, No. 3, 2013 Vertebral Osteomyelitis with Paravertebral Abscess: A Case Report Cho-Chao Feng Vertebral osteomyelitis usually presents with clinical manifestations, laboratory data and radiographic changes that are non-specific. This makes it difficult to diagnose during the early stages of the disease and consequently this increases morbidity. As a result it is a challenging diagnosis to most clinicians, especially the emergency physician. I report a case of vertebral osteomyelitis associated with paravertebral abscess diagnosed at an emergency department. This patient presented with back pain only and was discharged without complication after conservative treatment. Key words: vertebral osteomyelitis, paravertebral abscess Introduction Ve r t e b r a l o s t e o m y e l i t i s ( V O ) w a s f i r s t described in 1880 by Lannelongue (1) and since then there have been numerous articles published on the subject(2-7). It is usually caused by either direct postoperative inoculation of an infectious agent, by hematogenous spread of such an agent from a distant infectious focus such as the urinary tract infection (UTI) or by spread of a contiguous infection from adjacent soft tissue(3,4). The disease’s insidious clinical presentation, such as back pain, together with a lack of specific laboratory and radiographic findings, have contributed to delays in diagnosis and an increase in comorbidity(4). The most frequent comorbidities are septicemia (27%) and endocarditis (9%)(5,6). Carlos et al. described a complication rate for endocarditis of 30%(6). The mortality rate of VO among hospitalized patients ranges from 2.5% to 3.5% (5,6) . Another study has suggested a fatality rate for VO of 17% (7). Therefore, it is an important and challenging diagnosis for most medical clinicians, especially the emergency physician and this is especially true when the general condition of patient is unstable or there is poor ability to communicate with the patient, such as when the patient is elderly or has dementia. The vague chief complaints of patient and non-specific clinical presentation of this disease can also easily contribute to a misdiagnosis, which may leads to medico-legal issues. Therefore I report a case of vertebral osteomyelitis that was diagnosed at an emergency department (ED) and where the patient was discharged successfully without complication. Case Report A 69-years-old well conscious and oriented afebrile diabetic female patient presented at our ED during the weekend. Generalized weakness for a week without any other systemic symptoms and Received: April 3, 2013 Accepted for publication: December 25, 2013 From the Emergency Department, Hsinchu Cathay General Hospital Address reprint requests and correspondence: Dr. Cho-Chao Feng Emergency Department, Hsinchu Cathay General Hospital 678 Section 2, Zhonghua Road, Hsinchu, Taiwan (R.O.C.) Tel: (03)5278999 ext 1191 Fax: (03)5261499 E-mail: [email protected] Vertebral osteomyelitis with paravertebral abscess 95 signs were complained of by the patient. Physical examination revealed only a marked tenderness of was discharged after 2 weeks hospitalization and no recurrence has been found to have occurred on regularly followed up at an orthopedic department. The laboratory data was within normal limits except Discussion the back and the family stated that this had already lasted for more than six months and had been for the white blood cell count, which was 26920/ uL, a sugar level of 436 mg/dl and a CRP level of 14.38 mg/dl. Increased soft tissue density and vertebral spondylosis were noted when a thoracolumbar spine x-ray study was carried out (Fig. 1). Based on this, a CT scan was arranged, and this showed abnormal soft tissue with bone destruction at T8-10 and osteomyelitis with abscess formation (Fig. 2). A neurosurgeon was then consulted for debridement but conservative treatment was suggested. An MRI was arranged after admission to the ward. This showed pyogenic osteomyelitis with subligamentous spread together with paraspinal abscess formation at T7-9. Blood culture revealed Escherichia coli. A tuberculosis culture and acid fast staining were negative. This patient was treated intravenously with Ceftriaxone Sodium 2g q8h and Metronidazole 500 mg q8h for 10 days. The patient Fig. 1 follow-up. Vertebral osteomyelitis accounts of 3% to 7% of all cases of osteomyelitis(2,8). The incidence increases as the age of the patient increases(9), with rates of 0.3/100000 (<20 years old), 3.5/100000 (5070 years old) and 6.5/100000 (>70 years old)(5). The disease also affects intravenous drugs abusers and other immune compromised patients such as diabetics and cancer patients (10,11). The maleto-female sex ratio is about 1:1.5 (5, 12) . VO is caused by hematogenous dissemination through retrograde flow from the pelvic venous plexus to the perivertebral plexus(8), by a distant infection with an endogenous origin such as urinary tract infection (UTI); alternatively, it may follow direct inoculation from an exogenous origin such as a fixation device after spinal surgery(9,4,3). The most common infectious agents of endogenous origin are Staphylococcus aureus, The presence of increased soft tissue density (arrow) was noted on the thoraco-lumbar spine x-ray study 96 J Emerg Crit Care Med. Vol. 24, No. 3, 2013 Fig. 2 Abnormal soft tissue with bone destruction and abscess formation is present in the paraverterbral space (arrow) followed by E. coli. Coagulase-negative Staphylococcus and Propiopinibacterium acnes are common exogenous causative agents (9,5,11-13). I n a d d i t i o n , P s e u d o m o n a s a e r u g i n o s a (15), brucellosis(3,12,14) and tuberculosis(16) have also been reported as being involved in cases of vertebral osteomyelitis. Pathologically, the bacteria usually lodge in the arteriolar network of the metaphyseal region adjacent to the vertebral disc (8) . The infection begins near the anterior longitudinal ligament of vertebral bodies and then extends into the subligamentous paravertebral area, the epidural space and the contiguous vertebral bodies. Among elderly patients, increases in the length and degree of the arterioles within the cancellous part of the vertebral bodies leads sluggish blood flow, which then contributes to the infection(2). The most common site of vertebral osteomyelitis is the lumbar spine (58%), followed by the thoracic spine (30%) and then the cervical spine. (11%)(10,12). Clinical presentation is nonspecific. Back pain is the most common manifestation and is presented in 85 % of cases(12). In addition, localized tenderness on percussion, muscle spasm and a limited range of motion may also be present (16). Occasionally a local mass, fluctuant mass or kyphosis has been reported(2). Chang et al. reported a VO case that presented with abdominal pain only at the ED(17). Fever is present in only about one third of VO patients(2,12,18). with some studies showing about 23% to 30% of VO patients presenting with fever(10,11). Fever presentation does not seem to be related to the presence or absence of paravertebral abscess formation. Baldwin et al. reported four diabetic cases with vertebral osteomyelitis that had paravertebral abscesses and all were afebrile(19). McHenry et al. indicated that vertebral osteomyelitis may be complicated by epidural abscess in 17% of cases, by paravertebral abscess in 26% of cases and by disk-space abscess in 5 % of cases(7). Approximately 15% to 48% of VO patients may show an association with a neurological deficit including sensory loss and various types Vertebral osteomyelitis with paravertebral abscess 97 of myelopathy, such as quadriplegia and caudaequine syndrome(2,8,9,16). A review study suggested example leukocytosis. Most studies suggest that ESR can be used as a diagnostic marker severity of the neurological deficit depends on the site of vertebral involvement and when the spinal leukocytosis and very high values for ESR and CRP, may be used as diagnostic tools for VO(10). that 36.4% of VO cases had severe neurological deficits involving paraplegia or tetraplegia(6). The epidural abscess developed(2,8,9,16). The longer the diagnosis of VO is delayed, then the more frequent becomes the presence of spinal deformity, which, in turn, results in an increase in consequently neurological deficit(10). The neurological deficit and the frequency of motor dysfunction are closely related to the vertebral level that has been infected. These were found to be highest among patients with infections of the cervical spine (44%), followed by the thoracic spine (32%), the thoracolumbar spine (25%) and the lumbar (17%) spine(7). The relationship between the infectious agent and the neurological deficit resulting from VO remains controversial. Carlos et al. suggested that VO caused by Staphylococcus aureus is associated when a patient has pain and VO is clinically suspected (2,17,19) . Carmero et al. suggested that However, others have suggested that both ESR and CRP are only useful during treatment follow-up and in cases where there is postoperative spinal wound infection(4,20). The case presented here did not have her ESR level checked because CRP and ESR are equally useful when detecting an infection and both are known to increase when similar conditions are present, such as infection, malignancy and tissue trauma(21-24). A plain x-ray film is not a useful diagnostic tool for VO. This is because the disease usually presents nonspecifically and lacks early specific changes; these can include disc space narrowing, uneven destruction of adjacent end-plates and with more neurological deficits than other infected reactive changes within the adjacent vertebral body(2). Richard et al. suggested that disk narrowing related vertebral osteomyelitis is associated more often with neurological deficit complication than following the onset of symptoms and is quite frequent at 6-8 weeks into the illness (16). Such agents (6) . However, another comparative study of 219 VO cases concluded that tuberculosis vertebral osteomyelitis caused by other bacteria(10). The case in this article was afebrile and presented with no related neurological clinical manifestation. The diagnosis of VO may have been delayed in the patient because she had been treated with the long term use of oral analgesic medication for control of back pain by an orthopedic department and this may have masked other symptoms such as fever. The back pain had been misdiagnosed and treated as a chronic symptom related to spondylosis. As a consequent, other symptoms may have manifested themselves but were neglected by the care giver. Laboratory findings related to a diagnosis of VO are non specific and lack sensitivity, for is the earliest radiographic findings that can be detected and may occur as early as 2 weeks vertebral changes also may also be related to alternative diagnoses, including bone metastasis and osteoporotic changes(9). Hopkinson suggested that 18% of disc narrowing events are completely normal and that 41%, although abnormal, are agerelated findings only; these may be suggestive of discitis. He also suggested that CT is generally unhelpful(25). However, another study has suggested that CT and MRI are able to show significantly improved sensitivity and specificity compared to plain radiography (12). The CT imaging of VO usually reveals diffuse moth eaten or permeative bone destruction that involves the intervertebral disc as well as paravertebral osseous elements. In addition, there can be some gas associated with 98 J Emerg Crit Care Med. Vol. 24, No. 3, 2013 the bone and soft tissue, which was the situation with the patient presented in this article(4). Today, In addition, it can also be used for identification of the causative organism by carrying out an open make detailed assessments of bone destruction and to detect the exact position of the sequestrum(12). face many senile ED patients with a vague chief complaint such as generalized weakness, poor CT is the methodology of choice for the guidance of needle biopsies(13). In addition, it is also used to MRI has been recommended as a diagnostic tool for vertebral osteomyelitis and shows high sensitivity at the early stages of the disease; this is because there is better definition of the paravertebral and epidural space (13,25) , together with a high diagnostic accuracy of about 90%(9). Furthermore, the higher contrast resolution of MRI is able to detect marrow infiltration and intradural disease(4,12). The median time between the onset of symptoms and performance of MRI has been found to be 1.4 months(7). Unlike CT, MRI is the method of choice for detecting early infection and is able to fully evaluate the extent of the disease, including how it affects the spine, which allows delineating soft tissue involvement, investigating neural structure involvement and visualizing the formed abscess(12). The VO presented in this article showed vertebral spondylosis without destruction and was diagnosed incidentally by CT carried out at the ED after some unrelated vertebral plain film findings. An MRI was not arranged by the ED in the case presented in this article because the patient presented at a weekend. In Taiwan, MRI may not be available in some tertiary hospitals and is mostly can only be arranged during daytime working hours. Therefore, as an emergency physician and based on my experience in the presented case, I would suggest a CT scan is still a useful differential diagnostic tool for any ED patient who is clinically suspected of having VO, either with or without paravertebral abscess complications. The mainstay therapeutic choice when treating VO is conservative treatment. The goal of any surgical treatment is usually to relieve radicular neurological deficit and spinal cord compression(16). biopsy and for the management of severe pain(26). In conclusion, emergency physicians usually appetite or generalized body pain/soreness. These may not be accompanied by fever even if the patient is severely infected, as was the case with the patient presented in this article. Vertebral osteomyelitis can only be ruled out by an astute clinician after a complete history has been taken and a full physical examination has been carried out; these need to be correlated with appropriate laboratory findings. Finally, in order to diagnose vertebral osteomyelitis, the physician needs to get to the bottom of the problem and establish the true origin of the disease, as well as the underlying cause of the patient’s clinical presentations. There needs to be correlation between the patient’s laboratory findings and their radiographic changes, which are far more important than their MRI results and their ESR level. In addition, an early CT scan study should be arranged at ED for any patient who is suspected of vertebral osteomyelitis, whether this is complicated by paravertebral abscess or not. References 1. Ralph ZK, Joseph BH. Pyogenic vertebral osteomyelitis: diagnosis and management. Can Med Assoc J 1984;130:1025-7. 2. Jan L. pyogenic vertebral osteomyelitis/disc infection. Bailleiere’s. Clinical Rheumatology 1999;13:59-75. 3. Torda AJ, Gottlied T, Bradbury R. Pyogenic vertebral osteomyelitis: analysis of 20 cases and review. Clin Infect Dis 1995;20:320-8. 4. Jaramillo-de la Torre JJ, Bohinski RJ, Kuntz C.Vertebral osteomyelitis. Neurosurg Clin Am 2006;17:339-51. Vertebral osteomyelitis with paravertebral abscess 5. Grammatico L, Baron S, Rush E, et al. Epidemiology of vertebral osteomyelitis (VO) in France: analysis of hospital-discharge data 2002-2003. Epidemiol Infect 2008;136:653-60. 6. Carlos P, Benito A, Xaier F, et al. Spontaneous pyogenic vertebral osteomyelitis and endocarditis: Incidence, risk factors, and outcome. Am J Med 2005;118:128.e17-24. 7. M c H e n r y M C, E a s l e y K A, L o c k e r G A. Vertebral osteomyelitis: long-term outcome for 253 patients from 7 Cleveland-area hospitals. Clin Infect Dis 2002;34:1342-50. 8. Govender S. Spinal infections. The Journal of Bone and Joint Surgery 2005;87-B:1454-8. 9. Werner Z. Vertebral osteomyelitis. N Engl J Med 2010;362:1022-9. 10. Colmenero JD, Jimenez-Mejias ME, Sanchez –Lora FJ, et al. Pyogenic, tuberculous, and brucellar vertebral osteomyelitis: a descriptive and comparative study of 219 cases. Ann Rheum Dis 1997;56:709-15. 11. Judith L, Martin M. Spinal osteomyelitis: a review of 10 years’ experience. Orthopedics 1995;18:561-5. 12. Myolna E, Samarkos M, Kakalou E, et al. Pyogenic vertebral osteomyelitis: a systemic review of clinical characteristics. Semin Arthritis Rheum 2008,39:10-7. 13. Nolla JM, Ariza J, Gomez-Vaquero C, et al. Spontaneous pyogenic vertebral osteomyelitis ub nondrug users. Semin Arthritis Rheum 2002;31:271-8. 14. Chua F. Clinical picture. Lancet 2001;357:168. 15. Wa n g C C . P s e u d o m o n a s a e r u g i n o s a costovertebral arthritis in association with spontaneous cervical spondylodiscitis and epidural abscesses in the elderly. J Clin Gerontol Geriatr 2012;3:82-6. 16. R i c h a r d K O, P a t r i c k W H, A r n o l d H M. Pyogenic vertebral osteomyelitis in adults. 17. 18. 19. 20. 21. 22. 23. 24. 25. 99 Surg Neurol 1990;33:266-75. C h a n g T C, H u a n g M N, C h e n J C, e t a l Infectious spondylodiscitis with abdominal pain in ED. Am J Emerg Med 2011;29:133. e1-e3. Priest DH, Peacock JE jr. Hematogenous vertebral osteomyelitis due to Staphylococcus aureus in the adult: clinical features and t h e r a p e u t i c s o u t c o m e s. S o u t h M e d J 2005;98:854-62. Baldwin N, Scott AR, Heller SR, et al. Vertebral and paravertebral sepsis in diabetes: an easily missed cause of backache. Diabetic Medicine 1985;2:395-7. Khan MH, Smith PN. Rao N, et al. Serum C-reactive protein levels correlate with clinical response in patients treated with antibiotics for wound infections after spinal surgey. Spine J 2006;6:311-5. D e o d h a r S D. C-r e a c t i v e p r o t e i n: t h e best laboratory indicator available for monitoring disease activity. Cleve Clin J Med 1989;56:126-30. Kenny RA, Saunders AP, Coll A, Harrington MG, et al. A comparison of the erythrocyte sedimentation rate and serum C-reactive protein concentration in elderly patients. Age Ageing 1985;14:15-20. Osei-Bimpong A, Meek JH, Lewis SM. ESR or CRP? A comparison of their clinical utility. Hematology 2007;12:353-7. C o s t e n b a d e r K H, C h i b n i k L B, S c h u r P H. D i s c o r d a n c e b e t w e e n e r y t h r o c y t e sedimentation rate and C-reactive protein measurements: clinical significance. Clin Exp Rheumatol 2007;25:746-9. Hopkinson N, Stevenson J, Benjamin S. A case ascertainment study of septic discitis: clinical, microbiology and radiological features. Q J Med 2001;94:465-70. 100 J Emerg Crit Care Med. Vol. 24, No. 3, 2013 脊椎骨髓炎合併椎旁膿腫:個案報告 馮卓超 椎體骨髓炎通常是以非特異性的臨床表現、實驗數據和放射線的變化。因而難以早期診斷,因而使 得死亡率增加。所以,它對許多臨床醫師,特別是急診醫師而言是一個具有挑戰性的診斷。我要報告一 例在急診室診斷出合併有椎旁膿腫的椎體骨髓炎。病患僅以背部疼痛方式表現,經由保守治療後,在無 併發症狀況下出院。 關鍵詞: 脊椎骨髓炎,椎旁膿腫 收件:102年4月3日 接受刊載:102年12月25日 新竹國泰綜合醫院 急診科 通訊及抽印本索取:馮卓超醫師 新竹市中華路2段678號 新竹國泰綜合醫院急診科 電話:(03)5278999轉1191 傳真:(03)5261499 E-mail: [email protected]