Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
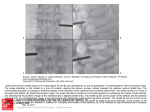
JFoetus-in-foetu: HK Coll Radiol. Imaging 2007;10:34-7 Diagnosis CASE REPORT Foetus-in-foetu: Imaging Diagnosis by the Presence of Organogenetic Differentiation AKP Wu,1 WWM Lam,1 KL Chan2 1 Department of Radiology, and 2Department of Surgery, Queen Mary Hospital, Hong Kong ABSTRACT Foetus-in-foetu is a rare condition in which a vertebrate foetus is enclosed within the abdomen of a normally developing foetus. This report is of a foetus-in-foetu in a newborn boy, in which no vertebral column was identified radiologically or pathologically. The ultrasound and computed tomography features will be discussed. The diagnosis was confirmed by pathology based on the presence of highly developed organogenesis. This patient demonstrates that the presence of a vertebral column is not essential for making the diagnosis. Key Words: Abdomen; Abnormalities; Diagnostic imaging; Fetus INTRODUCTION Foetus-in-foetu is an extremely uncommon cause of an abdominal mass in a neonate, which should be differentiated from the more common retroperitoneal teratoma. Foetus-in-foetu differs from retroperitoneal teratoma by its foetiform aspect and the metameric segmentation of its spinal axis.1 This report is of a foetus-in-foetu in a newborn boy, in which no vertebral column was identified radiologically or pathologically. The ultrasound and computed tomography (CT) findings are discussed. the bowel loops to the periphery (Figure 1). Speckles of calcifications were noted at the lower abdominal and pelvic regions. Ultrasound showed a large well-defined mass enveloped by a sac in the retroperitoneum that displaced the bowel laterally and the kidneys posteriorly (Figures 2a and 2b). This mass consisted of a roundish CASE REPORT A newborn boy was referred for surgery to remove a cystic mass with an internal solid component from the central abdomen. The mass was found by prenatal ultrasound. The boy was born at 38 weeks of gestation after a normal pregnancy. His birth weight was 3375 g. The neonate was asymptomatic. Physical examination showed a 6- to 7-cm firm mass over the central abdomen. His serum α-fetoprotein level was markedly elevated to 138,500 µg/L (normal range, <10 µg/L). Plain X-ray of the abdomen showed the presence of a soft tissue density in the central abdomen displacing Correspondence: Dr AKP Wu, Department of Radiology, Queen Mary Hospital, 102 Pokfulam Road, Hong Kong. Tel: (852) 2855 4900; Fax: (852) 2855 1513; E-mail: [email protected] Submitted: 17 April 2007; Accepted: 21 May 2007. 34 Figure 1. Plain X-ray of the abdomen showing soft tissue density (asterisk) in the central abdomen, displacing bowel loops to the periphery. There were speckles of calcification in the lower abdominal and pelvic regions (arrows). © 2007 Hong Kong Radiologists J HK CollCollege Radiol.of2007;10:34-7 AKP Wu, WWM Lam, KL Chan (a) (b) Figure 2. Ultrasound images taken at an oblique plane showing (a) a well-defined mixed echogenic mass inside a cystic cavity, consisting of a roundish nodular part and a tail-like extension (asterisk) — 2 tubular bony structures (arrow) were noted within the tail-like extension, resembling an undeveloped limb; and (b) at the tip of the tail-like extension, there were a cluster of bony structures (arrow) resembling the phalanges of the distal extremities. nodule with an elongated tail. Within this tail, there were 2 well-developed bony structures resembling the long bones of the extremities. Multiple smaller tubular bones resembling phalanges were noted at the tip of the tail. Several irregular bony structures were also identified within the roundish nodule. large well-defined mass enveloped by a sac in the retroperitoneum that displaced the kidneys posteriorly. The mass contained both cystic and solid portions. Some of the bony components resembled long bones and phalanges, while the rest were more disorganised (Figures 3a and 3b). CT was performed before surgery to better delineate the relationship between the mass and the adjacent organs. A multidetector CT scan (LightSpeed 16; GE Medical Systems, Milwaukee, USA) was used. Contrast-enhanced CT was performed after intravenous injection of omnipaque 2 mL/kg through an angiocatheter. Postprocessing was performed with reformatted images obtained at different planes. There was a The boy underwent surgical exploration 2 weeks after birth and a large retroperitoneal mass was identified. The mass was adherent to the mesenteric vessels, with some common vessels. Dissection of the mass from the mesenteric vessels was performed (Figure 4). (a) Gross examination revealed the mass to be a foetus-infoetu, lying inside a sac containing 60 mL of straw-coloured (b) Figure 3. Reformatted computed tomography images at an oblique plane showing (a) the presence of a heterogenous retroperitoneal mass composed of a roundish nodular mass and a tail-like extension (double arrow) — 2 long bones were identified within the tail-like extension, and more disorganised bony structures (arrow head) were noted within the nodular mass; and (b) phalanges-like structures (arrow) at the tip of the extension. J HK Coll Radiol. 2007;10:34-7 35 Foetus-in-foetu: Imaging Diagnosis mass can be completely resected, with no recurrence, and malignant degeneration is extremely rare.2 The distinction between the 2 conditions is based on Willis criteria, which stress the development of an axial skeleton with a vertebral axis, indicating that the foetal development of the included twin must have advanced at least beyond the primitive streak stage (12 to 15 days’ gestation) for a notochord — the precursor of the vertebral column — to have developed.1 To be determined as foetus-in-foetu, true organogenesis must be demonstrated.4 Figure 4. The mass (asterisk) was dissected from the mesenteric vessels. fluid. The mass was nodular and included a rudimentary limb. At the tip of the limb, there was a row of 5 digits with phalanx-like bony structures inside. Bony structures were also seen at the centre of the nodular mass. Microscopically, the membrane covering the sac had an amnionic membrane lining. The surface of the nodular mass showed skin covering. Pieces of cartilage and formed bone with haemopoetic bone marrow were contained within the nodular mass. Other components included neuroglial tissue, neural ganglia, nerve bundles, and immature skeletal muscles. No vertebral column was identified. The postoperative course was uneventful. The αfetoprotein decreased from 138,500 µg/L to 16,000 µg/L 1 week after operation. The patient was discharged on the seventh postoperative day. DISCUSSION The differential diagnoses of an intra-abdominal mass containing calcification includes foetus-in-foetu, teratoma, and meconium peritonitis. The term foetusin-foetu was first used by Meckel in the early nineteenth century to describe the condition in which a malformed parasitic twin is found inside the body of its partner, usually in the abdominal cavity. This is a rare abnormality secondary to abnormal embryogenesis in a diamniotic monochorionic pregnancy, an unusual condition in which a vertebrate foetus is enclosed within the abdomen of a normally developing foetus.2 However, teratoma is an accumulation of pluripotential cells in which there is neither organogenesis nor vertebral segmentation.3 Foetus-in-foetu differs from teratoma in that it carries an excellent prognosis for the host. The 36 If bony structure resembling vertebral column can be identified within the intra-abdominal mass by imaging study, the diagnosis of foetus-in-foetu will be straightforward. Review of the literature shows that in approximately 9% of cases of foetus-in-foetu, there was no vertebral column, even at pathologic examination.1 In this patient, no vertebral column-like structure was identified by imaging study or pathological examination. The demonstration of organogenetic differentiation in imaging is therefore crucial for the preoperative diagnosis to be made. By identifying long bones and phalanges within the tail-like extension of the mass, the presence of limbs and organogenesis was suggested. Limbs have been present in 82.5% of the reported cases.1 Foetus-in-foetu is an extremely uncommon cause of an abdominal mass in a neonate. The most common site of presentation is the retroperitoneum, as in this patient. A wide range of age of presentation has been document, varying from newborn to 27 years.5 Approximately 90 cases have been documented in the literature to date.1,2,6,7 The preoperative diagnosis of foetus-in-foetu was made in only 16.7% of the cases reported before 1980, which may be explained by the fact that CT was not widely available.2 It is only recently that reformed CT images at different planes have been possible due to the wide availability of multidetector CT. For this patient, although no vertebral column–like structure was identified, ultrasound and reformatted CT enabled images to be obtained at any plane so that the presence of the long bones and the phalanges-like structures could be demonstrated. REFERENCES 1. Hoeffel CC, Nguyen KQ, Phan HT, et al. Fetus in fetu: a case report and literature review. Pediatrics. 2000;105:1335-44. 2. Patankar T, Fatterpekar GM, Prasad S, Maniyar A, Mukherji J HK Coll Radiol. 2007;10:34-7 AKP Wu, WWM Lam, KL Chan SK. Fetus in fetu: CT appearance — report of two cases. Radiology. 2000;214:735-7. 3. Kim OH, Shinn KS. Postnatal growth of fetus-in fetu. Pediatr Radiol. 1993;23:411-2. 4. Hopkins KL, Dickson PK, Ball TI, Ricketts RR, O’Shea PA, Abramowsky CR. Fetus in fetu with malignant recurrence. J Pediatr Surg. 1997;32:1476-9. J HK Coll Radiol. 2007;10:34-7 5. Massad MG, Kong L, Benedetti E, et al. Dysphagia caused by a fetus-in-fetu in a 27-year-old man. Ann Thorac Surg. 2001;71 (4 Suppl):1338-41. 6. Taori KB, Khurana SD, Dhomne SP, Rathi V. Fetus in fetu — a rare case. Indian J Radiol Imag. 2003;13:85-7. 7. Phatak SV, Kolwadkar PK, Phatak MS. Fetus in fetu: a case report. Indian J Radiol Imag. 2003;13:93-4. 37