Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
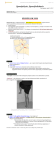
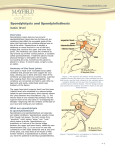
Spondylolysis and Spondylolisthesis Normal Anatomy • Pars interarticularis – Part of vertebra between inferior and superior articular process of the facet joint Pathophysiology • Spondylolysis – A fracture in the pars articularis – Usually a fatigue fracture • Spondylolisthesis – A displacement of one vertebrae over another – Usually L5 anteriorly – Although can be any level and any direction – Usually occurs due to spondylolysis Classification Spondylolisthesis: Classification • • • • • Grade 1: 0-25% vertebral slippage Grade 2: 25-50% vertebral slippage Grade 3: 50-75% vertebral slippage Grade 4: 75-100% vertebral slippage Grade 5: Complete slippage of the vertebral disc. Mechanism of Injury • Insidious • Insidious – Isthmic – Pathological • Repeated microtrauma usually into extension – – – – – – Wrestling Weightlifting Gymnastics Dancing Carrying a heavy back pack Athletics – Degenerative • Intervertebral disc degenerates changing joint orientation • Period of instability • Can cause excessive motion of the segment • Causing tipping or compression of vertebrae • Weakening of posterior elements e.g metastasis – Dysplastic • Congenital genetics – common in spina bifida occulta • Traumatic – Hyperflexion with compression and rotation – Hyperextension Associated Pathologies • • • • • Spondylolisthesis Spondylolysis Degenerative Disc Disease Stenosis Spina Bifida Occulta Pathophysiology • Continued excessive mechanical stress (or trauma/pathology/congenital) on the posterior elements of the vertebra • Causes fracture in weakest part of vertebra (pars) (Spondylolysis) • Shear forces throughout the vertebral column can result in displacement (Spondylolisthesis) Subjective • Most commonly aged 10 – 15, Female > Male • History of mechanical stress into extension – Gymnastics, dancing, athletics, weightlifting, diving • • • • • Localised paraspinal pain Pain with prolonged standing and hyperextension Pain on compression +/- Radiculopathy if neural compression Leg symptoms may switch sides if central neural compression Objective • • • • Hyperlordotic Pain extremes ROM Extension and Rotation Hypermobile and Vertebral Hinging • Step Deformity • Tight hamstrings (80%) Special Tests • One Legged hyperextension manoeuvre Further Investigation • Standing lateral oblique X ray (Scotty Dog with Collar) • CT and MRI to rule out other pathologies Further Investigation • Standing lateral oblique X ray (Scotty Dog with Collar) • CT and MRI to rule out other pathologies General Management • Activity modification avoiding positions of extension • Manual Therapy for pain relief ONLY • Treat instability • Refer if neurological symptoms present without prior investigations or worsening of neurological symptoms with previous investigations Conservative - Management • Pain Relief – Massage, NSAID’s, Ice, Activity Modification • Restore Normal Mobility – Hamstrings, Hip Extension, upper lumber and thoracic extension • Restore Normal Motor Control – Anterior Core (Anti Extension) • Dead Bug • Over Head Pallof Press • etc – Glutes, Anti Rotational Core • Restore Dynamic Stability • Return to Sport Specific Plan B - Management • Epidural steroid injection if radiculopathy is present • Surgical after 6 months of conservative treatment – Decompressive lumbar laminectomy in posterior fusion