Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Cardiac contractility modulation wikipedia , lookup
Remote ischemic conditioning wikipedia , lookup
Jatene procedure wikipedia , lookup
Artificial heart valve wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
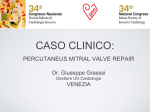
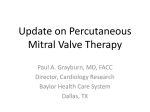
JACC: CARDIOVASCULAR INTERVENTIONS VOL. ª 2015 BY THE AMERICAN COLLEGE OF CARDIOLOGY FOUNDATION -, NO. -, 2016 ISSN 1936-8798/$36.00 PUBLISHED BY ELSEVIER http://dx.doi.org/10.1016/j.jcin.2015.09.039 Cerebral Protection During MitraClip Implantation Initial Experience at 2 Centers Christian Frerker, MD,* Michael Schlüter, PHD,y Oscar D. Sanchez, MD,z Sebastian Reith, MD,x Maria E. Romero, MD,z Elena Ladich, MD,z Jörg Schröder, MD,x Tobias Schmidt, MD,* Felix Kreidel, MD,* Michael Joner, MD,z Renu Virmani, MD,z Karl-Heinz Kuck, MD* ABSTRACT OBJECTIVES This study sought to assess the feasibility and safety of using a filter-based cerebral protection system (CPS) during MitraClip implantation and to report on the histopathologic analysis of the captured debris. BACKGROUND Stroke is one of the serious adverse events associated with MitraClip therapy. METHODS Between July 2014 and March 2015, 14 surgical high-risk patients (age 75 ! 7 years; 7 men; median logistic EuroSCORE 21%) underwent MitraClip implantation employing cerebral protection with a dual embolic filter system. All patients had severe mitral regurgitation of predominantly functional origin. RESULTS All procedures were successfully completed for both CPS deployment/retrieval and MitraClip implantation. A total of 28 filters (2 from each patient) were analyzed. Microscopically, debris was identified in all 14 patients. The most common tissue types were acute thrombus and small fragments of foreign material, which were found in 12 patients (85.7%) each. Organizing thrombus was present in 4 patients (28.6%), valve tissue and/or superficial atrial wall tissue in 9 patients (64.3%), and fragments of myocardium in 2 patients (14.3%). No transient ischemic attacks, strokes, or deaths occurred peri-procedurally or during a median follow-up interval of 8.4 months. CONCLUSIONS In this small study of patients undergoing MitraClip treatment with cerebral protection, embolic debris potentially conducive to cerebrovascular events was found in all patients. Debris was composed most often of acute thrombus, foreign material likely originating from the hydrophilic device coating, and valve/atrial wall tissue. Further studies are warranted to assess the impact of cerebral protection on the incidence of cerebrovascular events after MitraClip therapy. (J Am Coll Cardiol Intv 2016;-:-–-) © 2015 by the American College of Cardiology Foundation. M itral regurgitation (MR) is the second implantation in 2008, several studies have attested most common manifestation of valvular to the safety and effectiveness of this new percuta- heart disease in adults (1). Since the first neous treatment option in patients with moderate- MitraClip (Abbott Vascular, Santa Clara, California) to-severe or severe MR (2–4). Current guidelines From the *Department of Cardiology, Asklepios Klinik St. Georg, Hamburg, Germany; yAsklepios Proresearch, Hamburg, Germany; zCVPath Institute, Inc., Gaithersburg, Maryland; and the xDepartment of Cardiology, University Hospital of the RWTH Aachen, Aachen, Germany. Dr. Frerker reports that he has received lecture honoraria from Abbott Vascular, Inc., and Claret Medical, Inc. Dr. Joner reports that he has received honoraria from OrbusNeich, Abbott Vascular, Boston Scientific, and Biotronik; and research grants from OrbusNeich, Abbott Vascular, BioSensors International, SinoMedical, Terumo Corporation, CeloNova, W. L. Gore, Medtronic, Microport, Boston Scientific, and Biotronik. Dr. Virmani reports that she has served as a consultant to 480 Biomedical, Abbott Vascular, Medtronic, and W.L. Gore; has received honoraria from 480 Biomedical, Abbott Vascular, Boston Scientific, Cordis J&J, Lutonix Bard, Medtronic, Merck, Terumo Corporation, W.L. Gore, CSI, Meril Life Sciences, and Spectranetics; and has received institutional grants/ research support from 480 Biomedical, Abbott Vascular, Atrium, BioSensors International, Biotronik, Boston Scientific, Cordis J&J, GSK, Kona, Medtronic, MicroPort Medical, CeloNova, OrbusNeich Medical, ReCore, SINO Medical Technology, Terumo Corporation, W.L. Gore, Spectranetics, CSI, Lutonix Bard, Surmodics, and Meril Life Sciences. Dr. Kuck reports that he has received consultant fees and research grants from St. Jude Medical, Medtronic, and Edwards Lifesciences; and has received research grants from Abbott Vascular, Inc. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose. Manuscript received August 5, 2015; revised manuscript received September 14, 2015, accepted September 24, 2015. 2 Frerker et al. JACC: CARDIOVASCULAR INTERVENTIONS VOL. -, NO. -, 2016 Cerebral Protection During MitraClip Implantation ABBREVIATIONS consider the MitraClip system to be a treat- AND ACRONYMS ment option for high-surgical-risk patients ACT = activated clotting time CPS = cerebral protection (evidence class IIb) (5,6). Occurrence of a stroke or a transient ischemic attack (TIA) is one of the potential complications during system a MitraClip procedure. Incidences of 0.2% to IQR = interquartile range 2.6% have been reported (2,3,7). Blazek et al. MR = mitral regurgitation MRI = magnetic resonance imaging Academic Research Consortium TAVR = transcatheter aortic valve replacement T A B L E 1 Baseline Patient Characteristics (N ¼ 14) Men 7 (50) Age, yrs 75 ! 7 Body mass index, kg/m2 resulted in new ischemic cerebral lesions on Cerebral embolic protection devices for 5,673 (1,603–12,160) Left ventricle End-systolic diameter, mm studied. 21 (18–28) NT-proBNP, pg/ml End-diastolic diameter, mm aging (MRI) in 23 (85.7%) of 27 patients 26 ! 4 Logistic EuroSCORE, % (8) showed that the MitraClip procedure diffusion-weighted magnetic resonance im- MVARC = Mitral Valve - 2016:-–- 61 ! 9 48 ! 15 Ejection fraction, % 37 ! 16 NYHA functional class III 8 (57) IV 6 (43) Arterial hypertension 11/13 (85) the prevention of cerebrovascular events Hyperlipidemia have been introduced for transcatheter aortic Diabetes mellitus 5 (36) valve replacement (TAVR) procedures (9). Van Mie- COPD 5 (36) ghem et al. (10) reported on the histopathologic Pulmonary hypertension 7 (50) TIA = transient ischemic attack characteristics of debris captured and retrieved from a filter-based cerebral embolic protection device in 30 (75%) of 40 patients undergoing TAVR. The present study assessed the feasibility and safety of using a 9 (64) Atrial fibrillation 8 (57) Chronic renal insufficiency 7 (50) Coronary artery disease 7 (50) Previous cardiac surgery 2 (14) Peripheral arterial disease 3 (21) filter-based cerebral protection device during Mitra- Prior stroke 2 (14) Clip implantation and reports on the histopathologic MR etiology analysis of the debris captured. METHODS PATIENTS. Between July 2014 and March 2015, a total of 14 surgical high-risk patients underwent a MitraClip procedure that employed cerebral protection with the dual-filter Sentinel system (Claret Medical, Santa Rosa, California) at two German sites (Hamburg [n ¼ 10] and Aachen [n ¼ 4]). The Hamburg patients were treated consecutively in 2 series of 6 and 4 pa- tients; the Aachen patients were selected according to the patient’s propensity for thromboembolic events due to echocardiographically detected thrombus material on pacemaker or defibrillator leads. Four Degenerative 3 (21) Functional 11 (79) MR severity Severe 14 (100) Values are n (%), mean ! SD, or median (interquartile range). COPD ¼ chronic obstructive pulmonary disease; EuroSCORE ¼ European System for Cardiac Operative Risk Evaluation; MR ¼ mitral regurgitation; NT-proBNP ¼ N-terminal pro-brain natriuretic peptide; NYHA ¼ New York Heart Association. of the anticoagulation during the MitraClip intervention; 5 patients had dual antiplatelet therapy with aspirin and clopidogrel. Patients on dual antiplatelet therapy received a 300-mg loading dose of clopidogrel after the MitraClip procedure. Written informed consent was obtained from all patients. patients (29%) had an internal cardiac defibrillator CEREBRAL (2 of them as a cardiac resynchronization therapy) Cerebral Protection System (CPS) comprises 2 bag- and 1 patient (7%) had a two-chamber pacemaker. like embolic filters attached back-to-back to the tip No patient had a porcelain aorta. Pertinent baseline of a single 6-French compatible catheter, which is patient characteristics are given in Table 1. delivered from the right arm via radial or brachial PROTECTION DEVICE. The Sentinel All patients had severe MR of predominantly artery access over a standard 0.014-inch coronary functional origin. Left ventricular function was guidewire (Figure 1). The filter bags are made of impaired, with a mean ejection fraction of 37%, and polyurethane film with 140-m m laser-drilled holes, all patients presented with reduced physical capacity and each filter is mounted on a self-expanding (New York Heart Association functional class III or nitinol wire loop. The system is advanced under IV). A history of atrial fibrillation and prior stroke was fluoroscopic guidance such that the larger proximal present in 8 (57%) and 2 (14%) patients, respectively. filter (loop diameter: 9 to 15 mm) is deployed in the No patient was found to have a thrombus in the left brachiocephalic trunk, and the smaller distal filter atrial appendage or the left ventricle. Nine patients (loop diameter: 6.5 to 10 mm), which is in an artic- were on oral anticoagulation (phenprocoumon, n ¼ 4; direct oral anticoagulants, n ¼ 5) without interruption ulating sheath inside the proximal filter, is placed in the left common carotid artery. JACC: CARDIOVASCULAR INTERVENTIONS VOL. Frerker et al. -, NO. -, 2016 Cerebral Protection During MitraClip Implantation - 2016:-–- F I G U R E 1 The Cerebral Protection Device Used in This Study (A) Photograph of the Sentinel Cerebral Protection System (CPS) consisting of 2 filters for simultaneous protection of both the right side (proximal filter) and the left side (distal filter) of the brain. (B) Schematic of the CPS in place, with the proximal filter deployed in the brachiocephalic trunk and the distal filter in the left common carotid artery. MITRACLIP IMPLANTATION. A standardized anti- examined grossly for visible debris, then cut open; all coagulation regimen with heparin was initiated with a contents were filtered through a 40-m m nylon cell loading dose of 70 IU/kg aiming at an activated clot- strainer (BD Falcon/Corning, Durham, North Car- ting time (ACT) between 250 and 300 seconds. The olina). The majority of particles detected were bolus of heparin was given after the puncture of all adherent to the filter, with only a small number of peripheral vessels. Deployment of the cerebral pro- immersed particles retrieved from the fixative. The tection device was subsequently performed in all cell-strainer disc was photographed to document patients via right radial access—that is, before the successful debris transfer, and measurements of the transseptal puncture required for MitraClip implan- retrieved debris were performed. The specimens were tation. Left heart catheterization was not performed dehydrated in a graded series of alcohols and after placement of the CPS. embedded in paraffin, and sections of 5 to 6 mm The procedural details of percutaneous mitral thickness were cut, with 2 sections mounted on each valve repair using the MitraClip have been described glass slide. The sections were stained with hematox- before (2). All procedures were performed under ylin and eosin and Movat’s pentachrome. general anesthesia in a hybrid operating room. Procedural success was defined as discharge MR of maximally moderate severity. Procedural details are given in Table 2. After MitraClip implantation, the embolic filters T A B L E 2 Procedural Details and Outcome Parameters (N ¼ 14) Hospitalization, days ICU stay, days were withdrawn into the catheter and removed from Activated clotting time, s the patient. Outside, the filters were cut and stored in Contrast agent, ml 10% neutral buffered formalin solution and shipped Tamponade to the CVPath Institute (Gaithersburg, Maryland) for Severe bleeding analysis. HISTOPATHOLOGIC ASSESSMENT OF CAPTURED DEBRIS. A total of 28 filters (2 from each patient) were analyzed. The filters were photographed (Canon EOS Rebel XSi; Canon U.S.A., Melville, New York), 7.4 ! 5.0 1 (1–2) [n ¼ 6] 289 ! 48 12.5 (10–20) [n ¼ 10] 0 (0) 0 (0) Vascular complication 1 (7) Stroke 0 (0) TIA 0 (0) Values are mean ! SD, median (interquartile range), or n (%). ICU ¼ intensive care unit; TIA ¼ transient ischemic attack. 3 4 Frerker et al. JACC: CARDIOVASCULAR INTERVENTIONS VOL. Cerebral Protection During MitraClip Implantation - 2016:-–- The sections were evaluated for the presence of thrombus, valve and atrial wall tissue, vascular structures with or without atherosclerotic changes, myocardial fragments, -, NO. -, 2016 calcification, and the clip delivery system from the left atrium— amounted to 58 ! 31 min (range: 15 to 130 min). There were no peri-procedural TIAs or strokes. foreign A single vascular complication occurred in a patient material. Thrombus was classified as acute if it in whom the supra-aortic arteries were insufficiently showed platelets and fibrin with entrapped red blood visualized by angiography; the patient experienced cells and acute inflammatory cells, or as chronic if the bleeding from a small thyroid artery, which was thrombus showed the presence of spindle-shaped treated conservatively by administration of prot- cells with or without macrophages that lined the amine at the end of the procedure. During a median thrombus, infiltrated it, or had any organization with follow-up period of 8.4 months (IQR: 3.5 to 10.3 matrix deposition interspersed between the fibrin/ months), no patient died or experienced out-of- platelet thrombus. Two pathologists reviewed the hospital TIA or stroke. slides independently, and the final diagnosis was based on unanimous agreement. Histopathologic slides were scanned using a digital slide scanner (Axion Scan.Z1, Carl Zeiss, Thornwood, New York), and the morphometric analysis was performed using HALO digital image analysis software (Version 1, Indica Labs, Corrales, New Mexico). Quantitative measurements were performed on the 20 largest particles identified in each cross section. The cumulative area of debris was quantitated in each cross section using an internal algorithm for automated particle detection and was expressed as the cumulative area per case. Minimum and maximum diameters of individual particles were also determined. HISTOPATHOLOGY. Microscopically, debris was identified in all 14 patients. The morphometric analysis of a total of 515 sections (242 from proximal, 273 from distal filters) revealed a median cumulative particle area per patient of 2.46 (IQR: 0.44 to 3.67) mm 2 and a median maximum particle diameter of 295 (IQR: 104 to 509) m m; cumulative areas of debris captured in proximal and distal filters were 1.35 (0.30 to 2.09) mm 2 and 1.07 (IQR: 0.13 to 2.21) mm 2, respectively, with maximum diameters of 346 (IQR: 211 to 555) mm and 217 (IQR: 63 to 442) m m, respectively (p < 0.0001). The most common tissue types were acute thrombus (Figure 2A) and small fragments of nonpolarizable basophilic foreign material (Figure 3) that was morphologically consistent with STATISTICAL ANALYSIS. Continuous variables are hydrogel, which were found in 12 patients (85.7%) described as mean ! SD if normally distributed, or as each. Organizing thrombus (Figure 2B) was present in median (interquartile range [IQR]) if not. The Mann- 4 patients (28.6%), and 2 patients were devoid of any Whitney U test was used to assess between-group thrombus. differences in maximum particle diameter, with p < deposition, consistent with either valve tissue and/or 0.05 considered statistically significant. Categorical superficial atrial wall tissue (Figure 4), was found in a variables are described with absolute and relative total of 9 patients (64.3%). Two patients (14.3%) frequencies. showed minute fragments of myocardium. Tissue Fibroelastic tissue with proteoglycan particles exhibiting calcification were not observed in RESULTS any of the filters. PROCEDURAL OUTCOMES. The mean ACT in the 14 cording to the number of clips implanted and the procedures was 289 ! 48 seconds. All procedures were study site are given in Tables 3 and 4, respectively. No successfully completed for both CPS deployment/ difference in the distribution of debris type was retrieval and MitraClip implantation; 6 patients were apparent in either analysis. However, the maximum discharged with no or trace residual MR, 5 had mild particle diameters were statistically significantly MR, and 3 patients were discharged with moderate larger in patients treated with 2 clips (median 402 vs. MR. A single clip was implanted in 7 patients (Hamburg 134 m m [1 clip], p < 0.0001) and in patients treated Differentiations of histopathologic findings ac- n ¼ 5, Aachen n ¼ 2); the other 7 patients received 2 clips each. The mean transmitral pressure gradient after clip implantation was 3.3 ! 1.4 mm Hg (range: 1 to 6 mm Hg). in Aachen (median 411 vs. 262 mm [Hamburg], p < 0.0001). The various combinations of types of debris as found in the individual patients are shown in Figure 5. The procedures lasted for a mean of 91 ! 43 min The debris was composed of thrombus, valve/atrial (range: 40 to 200 min), with a fluoroscopy time of wall tissue, and foreign material in 8 patients (57%), 30 ! 16 min (range: 11 to 70 min). The total device time— and of thrombus plus foreign material without any the time from transseptal puncture to withdrawal of valve/atrial wall tissue in 3 patients (21%). In 1 patient JACC: CARDIOVASCULAR INTERVENTIONS VOL. Frerker et al. -, NO. -, 2016 Cerebral Protection During MitraClip Implantation - 2016:-–- F I G U R E 2 Type of Thrombus (A) Acute thrombus with platelet and fibrin (hematoxylin and eosin stained section). (B) Organizing thrombus with matrix deposition of proteoglycan (yellow arrowheads) (Movat’s pentachrome stained section). each the constituents of debris were thrombus and DISCUSSION myocardial fibers, foreign material and myocardial fibers, and valve/atrial wall tissue only. The debris was contained in all 14 proximal and all 14 distal filters. The type of debris captured at the 2 filter locations is shown in Figure 6. Note the similarity of the distributions, with most filters at both locations containing acute thrombus and foreign material, followed by valve/atrial wall tissue. Two filters at either location contained organizing MAIN FINDINGS. The main findings of this small study of using a dual-filter CPS during MitraClip implantation are as follows: # Using the CPS during a MitraClip procedure is feasible and safe. # Debris was found in all patients, with larger parti- cles identified in proximal filters, in patients thrombus, and myocardial fibers were detected only treated with 2 clips, and in patients at an increased in 2 distal filters. risk of thromboembolic events. F I G U R E 3 Foreign Material (A, B) Basophilic foreign material (yellow arrows) intermingled with acute fibrin-rich thrombus, rare neutrophils, and thrombocytes (hematoxylin and eosin stained sections). 5 6 Frerker et al. JACC: CARDIOVASCULAR INTERVENTIONS VOL. Cerebral Protection During MitraClip Implantation -, NO. -, 2016 - 2016:-–- F I G U R E 4 Valve Tissue (A and C) Fibroelastic tissue with proteoglycan deposition corresponding to valve tissue and foreign material (blue arrows). (B) High-power magnification of the boxed area in A. (D) High-power magnification of the boxed area in C. (A, B, C: hematoxylin and eosin stained section; D: Movat’s pentachrome stained section). # The most prevalent types of debris were acute of new peri-procedural cerebral ischemic events (11). thrombus and foreign material consistent with In a recent consensus document, the Mitral Valve hydrogel coating. Academic Research Consortium (MVARC) stated that CLINICAL RELEVANCE. It has been shown that percutaneous interventional procedures bear the risk T A B L E 3 Histopathologic Analysis According to Number of Clips Implanted stroke and TIA are “clinical endpoints to be collected in all trials of mitral valve therapies” (12). The incidence of stroke or TIA after a MitraClip procedure of up to 2.6% (7) justifies any attempt to prevent such complications. In this study, the Claret Sentinel device was 1 Clip (n ¼ 7) 2 Clips (n ¼ 7) Thrombus 6 (86) 6 (86) Acute 6 (86) 6 (86) CPS. The overall procedure duration of 91 min Organizing 2 (29) 2 (29) compares favorably with procedure times reported Foreign material 6 (86) 6 (86) in the Pilot European Sentinel MitraClip Registry Valve/atrial tissue 4 (57) 5 (71) Myocardium 2 (29) 0 (0) (138 min), the MitraClip post-approval ACCESS-EU 0.81 (0.36–2.06) [n ¼ 7] 3.45 (2.80–6.80) [n ¼ 7] Type of debris in filters Morphometry Cumulative particle area, mm2 Maximum particle diameter, mm 134 (56–336) [n ¼ 261] Values are n (%) or median (interquartile range). 402 (275–589) [n ¼ 254] used for cerebral protection during MitraClip procedures. Except for one minor vascular complication, no complications occurred while using this registry (100 min), and the German transcatheter mitral valve interventions (TRAMI) registry (103 min) (3,4,13). In our series of patients without any periprocedural cerebrovascular events, the filters captured debris in all patients. A recent diffusionweighted MRI study of patients after MitraClip JACC: CARDIOVASCULAR INTERVENTIONS VOL. Frerker et al. -, NO. -, 2016 Cerebral Protection During MitraClip Implantation - 2016:-–- T A B L E 4 Histopathologic Analysis According to Study Site Hamburg (n ¼ 10) F I G U R E 6 Type of Captured Debris by Filter Location Aachen (n ¼ 4) Type of debris in filters Thrombus 9 (90) 3 (75) Acute 9 (90) 3 (75) 3 (30) 1 (25) Foreign material Organizing 8 (80) 4 (100) Valve/atrial tissue 8 (80) 1 (25) Myocardium 1 (10) 1 (25) 2.24 (0.44–3.45) [n ¼ 10] 5.00 (1.13–8.47) [n ¼ 4] Morphometry Cumulative particle area, mm2 Maximum particle diameter, mm 262 (89–442) [n ¼ 374] 411 (206–647) [n ¼ 141] Values are n (%) or median (interquartile range). implantation without cerebral protection revealed an 86% incidence of newly acquired microembolic cerebral lesions (8), suggesting a strong relationship between embolic debris captured in filters during MitraClip implantation with cerebral protection and ischemic cerebral lesions detected by MRI after MitraClip implantation without cerebral protection. (A) Debris found in the 14 proximal filters protecting the brachiocephalic trunk. The majority of filters (12 [86%] and 9 F I G U R E 5 Distribution of Debris Captured in 14 Patients [64%], respectively) contained acute thrombus and foreign material; valve/atrial wall tissue was present in 7 filters (50%), and organizing thrombus was identified in 2 filters (14%). (B) Debris found in the 14 distal filters protecting the left common carotid artery. As in the proximal filters, the majority of distal filters (11 [79%] and 10 [71%], respectively) contained acute thrombus and foreign material; valve/atrial wall tissue was present in 5 filters (36%), and organizing thrombus and myocardial fibers were identified in 2 filters (14%) each. Although most of the MRI-detected embolic lesions remained clinically silent, other studies have shown that clinically silent cerebral lesions were associated with neurocognitive impairment and the development of dementia (14,15). Debris was captured by the cerebral protection system’s filters in all patients. Pie chart segments represent numbers (and POTENTIAL ORIGINS OF EMBOLI DURING TRANSCATHETER MITRAL VALVE REPAIR. Feld et al. (16) percentages) of patients with different compositions of debris. have shown that the Brockenbrough transseptal Most often found was a combination of thrombus, valve/atrial needle generates particles when advanced through wall tissue, and foreign material (n ¼ 8; light blue segment) the dilator and transseptal sheath. The particles in and of thrombus and foreign material without valve/atrial wall tissue (n ¼ 3; light brown segment). Thrombus plus myocar- dium, foreign material plus myocardium, and valve/atrial wall tissue only was found in 1 patient each. that study were not examined further for the type of material generated. In our study, foreign particles found in the filters consisted of nonpolarizable basophilic material that was morphologically consistent with hydrogel. To date, no evidence has 7 8 Frerker et al. JACC: CARDIOVASCULAR INTERVENTIONS VOL. -, NO. -, 2016 Cerebral Protection During MitraClip Implantation - 2016:-–- been found of foreign material arising from the Both methodological additions to the study protocol Sentinel filter itself and/or its coating. Even after we as well as a comparison with a matched cohort of manually scraped the surface of filters, no foreign patients undergoing MitraClip implantation without material was observed under high-magnification cerebral protection would have been desirable. microscopy. Hydrophilic coating is frequently used on medical CONCLUSIONS devices for interventional procedures to decrease friction between sheaths or catheters and vessel In this study of 14 patients undergoing MitraClip walls (17). Mehta et al. (18) identified hydrophilic treatment using a CPS, embolic debris potentially polymer emboli in conducive to cerebrovascular events was found in all various vascular 9 patients who underwent different patients. The debris was composed most often of coated devices. Furthermore, multiple findings of acute thrombus, foreign material likely originating hydrophilic-coating organs from the hydrophilic device coating, and valve/atrial have been described (19–21). For the MitraClip pro- wall tissue. No peri- or post-procedural strokes or cedure several catheters coated with hydrophilic TIAs occurred. Further studies are warranted to materials are used, such as the transseptal sheath assess the impact of cerebral protection on the inci- for transseptal puncture and the guide catheter for dence of cerebrovascular events after MitraClip the MitraClip system. However, it is unknown from therapy. interventions material in using different which catheter the majority of foreign material originated. The MVARC stated that transcatheter mitral valve therapies may predispose patients to the formation of ACKNOWLEDGMENT The authors thank Torie Samuda, PA, for her assistance in the histopathologic analyses. thrombus (12). Acute thrombus could develop at the REPRINT REQUESTS AND CORRESPONDENCE: Dr. transseptal sheath as well as at the guiding catheter Christian Frerker, Department of Cardiology, Asklepios and the clip delivery system due to their thrombo- Klinik St. Georg, Lohmühlenstr. 5, 20099 Hamburg, Ger- genic nature. Maleki et al. (22) reported up to 9% many. E-mail: [email protected]. thrombus formation on regular transseptal sheaths despite adequate anticoagulation. In our study, anticoagulation was adequate (as reflected by a mean ACT PERSPECTIVES of 289 s throughout the procedures). In a cohort of 81 patients who underwent TAVR, thrombotic material WHAT IS KNOWN? MitraClip implantation is a was found in 74% of patients (23). However, in that valid therapeutic option to relieve symptoms in trial the ACT was suboptimal at a mean of 230 seconds elderly patients with significant MR who are (23). deemed inoperable or at high surgical risk. The origin of the valve and atrial wall tissue Stroke has been observed, if rarely, in associa- captured in 9 patients (64%) could be the dislodge- tion with MitraClip therapy, and diffusion- ment of such material during the transseptal punc- weighted MRI studies have revealed a high ture and the advancement of the MitraClip into the incidence of new cerebral ischemic lesions after left ventricle across the mitral valve. Furthermore, the intervention. during grasping of the mitral leaflets some valve tissue might be embolized. Calcific debris was not found in any of the filters analyzed in our study. This finding appears to be consistent with the MRI study by Blazek et al. (8) who reported no impact of mitral valve calcification on the occurrence of embolic lesions. STUDY LIMITATIONS. The number of patients enrolled in this study was low. Most patients (11 of 14; 79%) had functional MR. Degenerative MR might be associated with more valve-related debris. We made no differentiation with respect to the type of MR. No brain imaging or assessment of neurocognitive function before and after the intervention was performed. WHAT IS NEW? The present study of a dual-filter cerebral protection system employed during MitraClip therapy has shown that embolic debris, composed predominantly of acute thrombus and foreign material likely originating from the hydrophilic device coating, was released in all patients. WHAT IS NEXT? Our findings warrant further studies to assess the impact of cerebral protection on the incidence of cerebrovascular events and possibly identify patients in whom cerebral protection should be mandatory during MitraClip implantation. JACC: CARDIOVASCULAR INTERVENTIONS VOL. Frerker et al. -, NO. -, 2016 Cerebral Protection During MitraClip Implantation - 2016:-–- REFERENCES 1. Iung B, Baron G, Butchart EG, et al. A prospective survey of patients with valvular heart disease in Europe: The Euro Heart Survey on Valvular Heart Disease. Eur Heart J 2003;24:1231–43. 2. Feldman T, Foster E, Glower DD, et al. Percutaneous repair or surgery for mitral regurgitation. N Engl J Med 2011;364:1395–406. 3. Nickenig G, Estevez-Loureiro R, Franzen O, et al. Percutaneous mitral valve edge-to-edge repair: inhospital results and 1-year follow-up of 628 patients of the 2011–2012 Pilot European Sentinel Registry. J Am Coll Cardiol 2014;64:875–84. 4. Maisano F, Franzen O, Baldus S, et al. Percutaneous mitral valve interventions in the real world: early and 1-year results from the ACCESSEU, a prospective, multicenter, nonrandomized post-approval study of the MitraClip therapy in Europe. J Am Coll Cardiol 2013;62:1052–61. 5. Nishimura RA, Otto CM, Bonow RO, et al. 2014 AHA/ACC guideline for the management of patients with valvular heart disease: executive summary: a report of the American College of Cardiology/ American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol 2014;63:2438–88. 6. Vahanian A, Alfieri O, Andreotti F, et al. Guidelines on the management of valvular heart disease (version 2012). Eur Heart J 2012;33:2451–96. patients undergoing transcatheter aortic valve implantation. EuroIntervention 2012;8:43–50. 10. Van Mieghem NM, Schipper ME, Ladich E, et al. Histopathology of embolic debris captured during transcatheter aortic valve replacement. Circulation 2013;127:2194–201. 11. Bendszus M, Stoll G. Silent cerebral ischaemia: hidden fingerprints of invasive medical procedures. Lancet Neurol 2006;5:364–72. 12. Stone GW, Adams DH, Abraham WT, et al. Clinical trial design principles and endpoint definitions for transcatheter mitral valve repair and replacement: part 2: endpoint definitions: A consensus document from the Mitral Valve Academic Research Consortium. J Am Coll Cardiol 2015;66:308–21. 13. Zuern CS, Bauer A, Lubos E, et al. Influence of non-cardiac comorbidities on outcome after percutaneous mitral valve repair: results from the German transcatheter mitral valve interventions (TRAMI) registry. Clin Res Cardiol 2015;104: 1044–53. 14. Vermeer SE, Prins ND, den Heijer T, Hofman A, Koudstaal PJ, Breteler MM. Silent brain infarcts and the risk of dementia and cognitive decline. N Engl J Med 2003;348:1215–22. 7. Glower DD, Kar S, Trento A, et al. Percutaneous mitral valve repair for mitral regurgitation in highrisk patients: results of the EVEREST II study. J Am Coll Cardiol 2014;64:172–81. 15. Ghanem A, Müller A, Nähle CP, et al. Risk and fate of cerebral embolism after transfemoral aortic valve implantation: a prospective pilot study with diffusion-weighted magnetic resonance imaging. J Am Coll Cardiol 2010;55:1427–32. 8. Blazek S, Lurz P, Mangner N, et al. Incidence, characteristics and functional implications of cerebral embolic lesions after the MitraClip procedure. EuroIntervention 2015;10:1195–203. 16. Feld GK, Tiongson J, Oshodi G. Particle formation and risk of embolization during transseptal catheterization: comparison of standard trans- 9. Naber CK, Ghanem A, Abizaid AA, et al. First-inman use of a novel embolic protection device for septal needles and a new radiofrequency transseptal needle. J Interv Card Electrophysiol 2011; 30:31–6. 17. Nagaoka S, Akashi R. Low-friction hydrophilic surface for medical devices. Biomaterials 1990;11: 419–24. 18. Mehta RI, Mehta RI, Solis OE, et al. Hydrophilic polymer emboli: an under-recognized iatrogenic cause of ischemia and infarct. Mod Pathol 2010; 23:921–30. 19. Babcock DE, Hergenrother RW, Craig DA, Kolodgie FD, Virmani R. In vivo distribution of particulate matter from coated angioplasty balloon catheters. 3196–205. Biomaterials 2013;34: 20. Schipper ME, Stella PR, de Jonge N, Virmani R, de Weger RA, Vink A. Embolization of hydrophilic coating material to small intracardial arteries after multiple percutaneous transluminal angioplasty procedures. Int J Cardiol 2012;155: e45–6. 21. Allan RW, Alnuaimat H, Edwards WD, Tazelaar HD. Embolization of hydrophilic catheter coating to the lungs: report of a case mimicking granulomatous vasculitis. Am J Clin Pathol 2009; 132:794–7. 22. Maleki K, Mohammadi R, Hart D, Cotiga D, Farhat N, Steinberg JS. Intracardiac ultrasound detection of thrombus on transseptal sheath: incidence, treatment, and prevention. J Cardiovasc Electrophysiol 2005;16:561–5. 23. Van Mieghem NM, El Faquir N, Rahhab Z, et al. Incidence and predictors of debris embolizing to the brain during transcatheter aortic valve implantation. J Am Coll Cardiol Intv 2015;8: 718–24. KEY WORDS cerebral protection, embolization, MitraClip, mitral regurgitation, transcatheter mitral valve repair 9