Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Quantium Medical Cardiac Output wikipedia , lookup
History of invasive and interventional cardiology wikipedia , lookup
Saturated fat and cardiovascular disease wikipedia , lookup
Cardiovascular disease wikipedia , lookup
Electrocardiography wikipedia , lookup
Cardiac surgery wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Jatene procedure wikipedia , lookup
Echocardiography wikipedia , lookup
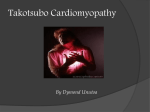
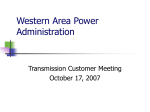
CASE REPORT 258 An uncommon case of T TC in in a young woman with multiple sclerosis Basal Tako-Tsubo cardiomyopathy Mattia Cattaneo a , Alessandra Pia Porretta a , Carlo Cereda b , Marco Moccetti c , Claudio Gobbi b , Elena Pasotti c , Daniel Sürder c , Claudio Städler b , Augusto Gallino a, d a Cardiovascular Medicine Department, Ospedale Regionale di Bellinzona e Valli, Bellinzona, Switzerland; b Department of Neurology, Neurocenter of Southern Switzerland, Ospedale Regionale, Lugano, Switzerland; c Department of Cardiology, Fondazione Cardiocentro Ticino, Lugano, Switzerland; d University of Zürich, Switzerland 1C–D). Although cardiac magnetic resonance imaging Summary (MRI) was not performed, the diagnosis of myocarditis Tako-Tsubo cardiomyopathy (TTC) is an infrequent, mostly stress-related transient cardiomyopathy, which mainly affects postmenopausal women. Inverted or basal TTC (B-TTC) episodes are rarer. Our case illustrates a rare example of B-TTC in a 30-year-old woman with an acute multiple sclerosis relapse as the associated stressor, possibly providing a hypothetical pathological substrate for this TTC episode. This uncommon case suggests that both factors of young age or neurological events may affect TTC pattern during one episode. Moreover, this case raises the question as to whether researchers on TTC should adopt a new perspective, embracing cardiovascular as well as neuroanatomical and -functional features. Key words: Tako-Tsubo cardiomyopathy; apical-sparing; multiple sclerosis; young age was reasonably rejected owing to the absence of systemic inflammation (normal C-reactive protein, leucocyte and procalcitonin values), negative bacterial blood cultures and viral tests. Phaeochromocytoma was excluded because of normal 24-hour urine fractionated catecholamines and metanephrines. Two days later the ECG showed complete spontaneous normalisation (fig. 2). Thus, the diagnosis of basal (inverted) Tako-Tsubo cardiomyopathy (TTC) was retained. Cerebrospinal MRI performed 5 days before the TTC episode showed an acute inflammatory lesion affecting dorsal medulla (fig. 1E). This area is involved in cardio- Case report vascular homeostasis and regulation of autonomic responses to stressful events through sympathetic drive The current report describes a 30-year-old Caucasian [1], thus providing a hypothetical pathological sub- woman who came to our attention because she pre- strate for this TTC episode. This medullary lesion re- sented with a rapidly progressing bilateral proprio- covered at 5-month MRI follow-up. ceptive ataxia, spinothalamic hypoaesthesia and gait impairment. Two years before, the patient had experienced an analogous neurological episode. Medical history, clinical, laboratory and imaging findings sup- Discussion Tako-Tsubo cardiomyopathy (TTC) is an infrequent, ported the diagnosis of an acute multiple sclerosis mostly stress-related transient cardiomyopathy, which relapse according to McDonald criteria. Intravenous, is currently poorly understood and simulates acute and later oral, steroid therapy was implemented with coronary syndrome in the absence of significant ob- suboptimal patient relief. Ten days later the patient structive lesions on coronary angiography [2]. TTC was transferred to the coronary care unit because of mainly affects the midapical segments of the left ven- acute typical chest pain. With the exception of ongoing tricle in postmenopausal women and apical-sparing significant neurological impairment no further clini- TTC episodes are rare [2]. Relying on a few case reports cal findings nor haemodynamic compromise were and a small observational trial, some investigators present. The electrocardiogram (ECG) showed diffuse have raised the question of whether inverted or basal ST-segment depression (fig. 1A), the corrected QT-inter- TTC (B-TTC) may be associated with young (premeno- val was not prolonged (409 msec) and brain natriuretic pausal) age [3–6], neurological events that act as psy- peptide (BNP) levels were not measured. Transthoracic cho-physical stressors, and/or acute and sub-acute echocardiography showed akinetic basal segments (fig. neurological events acting as psychophysical stressors 1B: 4-chamber view, end-systole: arrows) and apical hy- [7]. percontractility with slightly reduced (45–50%) left Our case illustrates a rare example of B-TTC in a ventricle ejection fraction (LVEF%) (see online Video 1: 30-year-old woman with an acute relapse of multiple four-chamber view). These findings were inconsistent sclerosis acting as an associated stressor. Approxi- with a moderate increase in serum troponin (peak 3.5; mately 90% of reported TTC cases occur in postmeno- reference value <0.09). The patient immediately under- pausal women of advanced age and are mostly related went selective coronary angiography, which disclosed to emotional or physical stress [2, 8]. There is evidence the absence of any coronary stenosis or dissection (fig. that a pathophysiological association between neuro- CARDIOVASCULAR MEDICINE – KARDIOVASKULÄRE MEDIZIN – MÉDECINE CARDIOVASCULAIRE 2015;18(9):258–260 CASE REPORT 259 Figure 1: Acute phase ECG shows diffuse ST-segment depression. (A) Transthoracic echocardiography, 4-chamber view, end-systole (B) shows akinetic basal segments (arrows) and apical hypercontractility (see also online Video 1). Selective left (C) and right (D) coronary artery angiography show absence of any coronary stenosis or dissection. (E) Axial T2-weighted MRI showing an acute dorsal medullary inflammatory lesion affecting the solitary tract and the ventro-lateral medulla (arrow). logical disorders and TTC may exist [7]. Diagnostic cri- tion of whether TTC episodes related to all sorts of teria have been published excluding TTC in the case of acute neurological events should be classified as TTC in acute cerebrovascular events and critically ill patients future diagnostic criteria and whether TTC diagnostic [2, 8, 9]. criteria should be revised. Lastly, it suggests that fu- Previously described cases have suggested that AS-TTC ture research on TTC should be based on a new per- is associated with either young age or neurological spective, embracing cardiovascular as well as neuroan- events. This uncommon case suggests that both condi- atomical and -functional features. tions may affect TTC pattern during the same episode and that it should be considered for the patient’s correct management. It has actually been shown that different TTC patterns may be associated with different complications and short-term mortality [10]. Furthermore, only acute cerebrovascular events are currently considered exclusion criteria. This case raises the ques- CARDIOVASCULAR MEDICINE – KARDIOVASKULÄRE MEDIZIN – MÉDECINE CARDIOVASCULAIRE Video on www.cardiovascmed.ch: Transthoracic echocardiography (4-chamber view) end-systole: it displays left ventricle (LV) wall motion abnormalities with akinetic basal segments, apical hypercontractility and moderately reduced LV ejection fraction. 2015;18(9):258–260 CASE REPORT 260 Figure 2: Post-acute phase ECG demonstrates complete normalisation of repolarisation within two days. Authors’ contribution All authors take responsibility for all aspects of the reliability and freedom from bias of the data presented and their discussed interpretation. Disclosure statement No financial support and no other potential conflict of interest relevant to this article were reported. References Correspondence: Mattia Cattaneo, MD Clinical and Research fellow Cardiovascular Medicine Department – Ospedale Regionale di Bellinzona e Valli, San Giovanni (EOC), Via Soleggio CH-6500 Bellinzona Switzerland mattia.cattaneo[at]eoc.ch 1 Taggart P, Critchley H, Lambiase PD. Heart-brain interactions in cardiac arrhythmia. Heart. 2011;97(9):698–708. 2 Prasad A, Lerman A, Rihal CS. Apical ballooning syndrome (TakoTsubo or stress cardiomyopathy): A mimic of acute myocardial infarction. Am Heart J. 2008;155:408–17. 3 Mansencal N, Abbou N, N’Guetta R, Pilliere R, El Mahmoud R, Dubourg O. Apical-sparing variant of Tako-Tsubo cardiomyopathy: prevalence and characteristics. Arch Cardiovasc Dis. 2010;103(2):75–9. 4 Mansencal N, El Mahmoud R, Pilliere R, Dubourg O. Relationship between pattern of Tako-Tsubo cardiomyopathy and age: from midventricular to apical ballooning syndrome. Int J Cardiol. 2010;138(1):e18–20. CARDIOVASCULAR MEDICINE – KARDIOVASKULÄRE MEDIZIN – MÉDECINE CARDIOVASCULAIRE 5 Reuss CS, Lester SJ, Hurst RT, Askew JW, Nager P, Lusk J, et al. Isolated left ventricular basal ballooning phenotype of transient cardiomyopathy in young women. Am J Cardiol. 2007;99(10):1451–3. 6 Berton E, Vitali-Serdoz L, Vallon P, Maschio M, Gortani G, Benettoni A. Young girl with apical ballooning heart syndrome. Int J Cardiol. 2012;161(1):e4–6. 7 Santoro F, Carapelle E, Cieza Ortiz SI, Musaico F, Ferraretti A, d’Orsi G, et al. Potential links between neurological disease and TakoTsubo cardiomyopathy: a literature review. Int J Cardiol. 2013;168(2):688–91. 8 Akashi YJ, Goldstein DS, Barbaro G, Ueyama T. Takotsubo cardiomyopathy: a new form of acute, reversible heart failure. Circulation 2008;118:2754–62. 9 Scantlebury DC, Prasad A. Diagnosis of Takotsubo cardiomyopathy. Circ J. 2014;78(9):2129–39. 10 Nishida J, Kouzu H, Hashimoto A, Fujito T, Kawamukai M, Mochizuki A et al. “Ballooning” patterns in takotsubo cardiomyopathy reflect different clinical backgrounds and outcomes: a BOREAS-TCM study. Heart Vessels. 2014 Jul 25. [Epub ahead of print] 2015;18(9):258–260