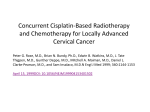
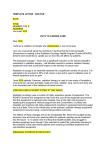
Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
ORIGINAL ARTICLE Retrospective Analysis of Concomitant Cisplatin During Radiation in Patients Aged 55 Years or Older for Treatment of Advanced Cervical Cancer A Gynecologic Oncology Group Study Charles Kunos, MD, PhD,* Chunqiao Tian, PhD,Þ Steven Waggoner, MD,þ Peter G. Rose, MD,§ and Rachelle Lanciano, MD|| Hypothesis: Patients with stages II to IVa cervical cancer aged 55 years or older were compared with patients younger than 55 years who received weekly cisplatin during pelvic radiation for differences in chemoradiation administration, toxicity, and outcome. Methods: Retrospective review included patients enrolled on Gynecologic Oncology Group trial Nos. 120 and 165 (n = 335) who received weekly cisplatin (40 mg/m2) during pelvic irradiation (40.8Y50.1 Gy) followed by intracavitary brachytherapy (30Y40 Gy). Results: For all 335 patients, 53% completed 6 cycles of chemotherapy during radiation with no observed difference in frequency among patients younger than 55 years or 55 years or older (P = 0.616). Excess hematological but not genitourinary toxicity was seen in patients 55 years or older. At 5 years, 56% of patients younger than 55 years were predicted to be alive and disease-free compared with 55% of those aged 55 years or older (P = 0.629). A 5-year survival was 60% in patients younger than 55 years as compared with 56% in patients aged 55 years or older (P = 0.265). Conclusions: Patients aged 55 years or older with locally advanced cervical cancer undergoing concurrent weekly cisplatin with pelvic radiation on cooperative group clinical trials achieve similar progression-free and overall survivals as younger patients. Disparity was not observed in the seriousness or frequency of treatment-related sequelae. Key Words: Cervical cancer, Chemoradiation, Elderly Received April 7, 2009, and in revised form May 19, 2009. Accepted for publication June 16, 2009. (Int J Gynecol Cancer 2009;19: 1258Y1263) *Department of Radiation Oncology, Case Comprehensive Cancer Center and University Hospitals of Cleveland Case Medical Center, Cleveland, Ohio; †Gynecologic Oncology Group Statistical and Data Center, Roswell Park Cancer Institute, Buffalo, NY; ‡Department of Obstetrics and Gynecology, Division of Gynecologic Oncology, Case Comprehensive Cancer Center and University Hospitals of Cleveland Case Medical Center; §Department of Obstetrics and Gynecology, Division of Gynecologic Oncology, Case Comprehensive Cancer Center and The Cleveland Clinic, Cleveland, OH; and ||Department of Radiation Oncology, Delaware County Memorial Hospital, Drexel Hill, PA. Address correspondence and reprint requests to Charles Kunos, MD, PhD, Department of Radiation Oncology, University Hospitals Case Medical Center, 11100 Euclid Ave, LTR 6068, Cleveland, Ohio 44106. E-mail: [email protected]. This study was supported in part by a grant (K12 CA076917) to C.K. from the National Institutes of Health and the Case Comprehensive Cancer Center and also by National Cancer Institute grants to the Gynecologic Oncology Group Administrative Office (CA 27469) and the Gynecologic Oncology Group Statistical Office (CA 37517). The following member institutions participated in this study: University of Alabama at Birmingham, Oregon Health Sciences University, Duke University Medical Center, Abington Memorial Hospital, University of Copyright * 2009 by IGCS and ESGO ISSN: 1048-891X DOI: 10.1111/IGC.0b013e3181b33ace 1258 Rochester Medical Center, Walter Reed Army Medical Center, Wayne State University, University of Minnesota Medical School, Emory University Clinic, University of Southern California at Los Angeles, University of Mississippi Medical Center, Colorado Gynecologic Oncology Group, PC, University of California at Los Angeles, University of Washington, University of Pennsylvania Cancer Center, University of Miami School of Medicine, Milton S. Hershey Medical Center, Georgetown University Hospital, University of Cincinnati, University of North Carolina School of Medicine, University of Iowa Hospitals and Clinics, University of Texas Southwestern Medical Center at Dallas, Indiana University School of Medicine, Wake Forest University School of Medicine, Albany Medical College, University of California Medical Center at Irvine, Tufts-New England Medical Center, Rush-Presbyterian-St Luke’s Medical Center, SUNY Downstate Medical Center, University of Kentucky, Eastern Virginia Medical School, The Cleveland Clinic Foundation, Johns Hopkins Oncology Center, State University of New York at Stony Brook, Eastern Pennsylvania GYN/ONC Center, PC, Cooper Hospital/University Medical Center, Columbus Cancer Council, University of Massachusetts Medical School, Fox Chase Cancer Center, Medical University of South Carolina, Women’s Cancer Center, University of Oklahoma, University of Virginia Health Sciences Center, University of Chicago, University of Arizona Health Science Center, Tacoma General Hospital, Mayo Clinic, Case Western Reserve University, Tampa Bay Cancer Consortium, and The New York Hospital/Cornell Medical Center. International Journal of Gynecological Cancer & Volume 19, Number 7, October 2009 Copyright @ 2009 by IGCS and ESGO. Unauthorized reproduction of this article is prohibited. International Journal of Gynecological Cancer & Volume 19, Number 7, October 2009 C ervical carcinoma ranks second among malignancies in women worldwide, accounting for nearly 190,000 deaths annually.1 Age at diagnosis for new cases of cervical carcinoma has been observed to follow a bimodal distribution, with peak ages at 30 to 39 years and 60 to 69 years. Age at diagnosis has been identified as a risk factor for cancer relapse and death after chemoradiation for locally advanced stages II to IVa cervical cancer. A prior Gynecologic Oncology Group (GOG) multivariate study of nonYcisplatincontaining chemoradiation trials showed that older patient age was significantly associated with less frequent cervical cancer relapse or cancer-related death,2 yet contemporary cisplatin-containing chemoradiation trials no longer identify patient age influencing risk of relapse or survival after adjusting for cofactors.3Y8 Nevertheless, population-based studies have shown an increased disparity in cervical cancer incidence and mortality among patients aged 55 years or older.1,9 The US Surveillance, Epidemiology, and End-Results (SEER) cancer registries reported a 35% incidence of cervical cancer but 55% cervical cancerYrelated mortality for patients aged 55 years or older (1998Y2002).10 Explanations for the disparity between cervical cancer incidence and mortality are lacking. Perhaps, patient chemotherapy administration during radiation is not being realized as recommended by cooperative group clinical trials.3Y8 An earlier national Patterns of Care Study evaluating practice patterns between 1996 and 1999 showed that 25% of patients 60 years or older underwent chemoradiation for cervical cancer as compared with 48% among patients aged 40 years or younger (P = 0.02).11 Between 1998 and 2002, SEER-Medicare data show increased chemoradiation administration among women aged 55 years or older; however, only 43% aged 55 years or older received concurrent chemoradiation.9 Whether patients aged 55 years or older derive benefit from chemoradiation treatment of cervical cancer remains relatively unknown. This is, in part, because of limited numbers of patients aged 55 years or older enrolled in clinical chemoradiation studies of advanced cervical cancer. Beliefs that patients aged 55 years or older tolerate chemoradiation more poorly may also lead to a lack of clinical outcome benefit for chemoradiation.12 In the case of concurrent radiosensitizing cisplatin, perceived and actual hematological, genitourinary, and gastrointestinal sequelae often lead to the practice of withholding chemoradiation for treatment of cervical cancer in older patients.13,14 The purpose of this retrospective study was to evaluate chemoradiation administration, toxicity, and outcome of patients with cervical cancer aged 55 years or older as compared with patients younger than 55 years treated on GOG protocol Nos. 120 and 165. METHODS Detailed methodology for clinical trial GOG Nos. 120 and 165 have been published previously.3,4 Briefly, patients had untreated stage IIB, III, or IVA invasive squamous, adenosquamous, or adenocarcinoma of the cervix. To establish clinical stage, patients must have undergone complete physical examination, pelvic examination, and chest radiograph. Surgical staging was mandatory for GOG No. 120 but optional for GOG No. 165, with 18% of GOG No. 165 study patients undergoing surgical staging.3,4 Patients with disease outside the pelvis, those with surgically or radiographically confirmed para-aortic node metastasis or those not candidates for radiation, were ineligible. Institutional review board approval among participating institutions was obtained for clinical trial GOG protocol Nos. 120 and 165. Written informed consent consistent with institutional, state, and federal regulations was obtained before entry on the study and randomization. Chemoradiation in Women Aged 55 Years or Older Chemotherapy Gynecologic Oncology Group Nos. 120 (n = 176) and 165 (n = 159) included patients randomly assigned to weekly cisplatin chemotherapy (40 mg/m2) for 4 hours before radiation therapy on days 1, 8, 15, 22, 29, and 36. Cisplatin chemotherapy was discontinued for leukopenia (GOG 0120 G 2500 or GOG 0165 G 3000 per cubic millimeter) or thrombocytopenia (GOG 0120 G 50,000 or GOG 0165 G 100,000 per cubic millimeter) and resumed after resolution. For subsequent cycles, cisplatin chemotherapy was discontinued for neurotoxicity grade 3 and higher or a creatinine level of more than 2 mg/dL. Gynecologic Oncology Group Nos. 120 and 165 did not specify growth factor administration. Radiation For GOG No. 120, anterior-posterior and posterior-anterior or 4-field box technique pelvic radiation was delivered in 1.7-Gy fractions using 4-MV photons or higher to doses ranging from 40.8 Gy for patients with stage II to 51.0 Gy for patients with stage III/IVA. In GOG No. 165, 4-field box pelvic radiation was delivered in 1.8-Gy fractions using 4-MV photons or higher to a dose of 45.0 Gy. In general, the 4-field box techniques used an upper margin of the L5 vertebra and a lower margin of the midportion of the obturator foramen or the lowest extent of disease with a 3-cm margin for anterior and posterior radiation fields. Laterally, the anterior and posterior radiation fields extended 1.5 to 2 cm beyond the pelvic brim. For right and left lateral radiation fields, the anterior border was the pubic symphysis, and the posterior border was the space between the S2 and S3 vertebrae. The superior and inferior margins for lateral radiation fields were the same as the anterior and posterior radiation fields. Intracavitary lowYdose rate brachytherapy followed external beam radiation 1 to 3 weeks later. One or 2 applications were allowed. LowYdose rate brachytherapy doses were 40.0 Gy for patients with stage II and 30.0 Gy for patients with stage III/IVA on GOG protocol No. 120 and 40.0 Gy for all stages on GOG No. 165, prescribed to radiation prescription point A. If intracavitary brachytherapy could not be delivered, additional external beam radiation to a dose of 61.2 Gy was done. Interstitial brachytherapy was not allowed on GOG No. 120 or 165, but highYdose rate brachytherapy was allowed on GOG No. 165. For GOG No. 165, highYdose rate brachytherapy consisted of 5 fractions of 6.0 Gy (total dose, 30.0 Gy) started the fourth week of external beam radiation with at least 1 fraction per week. In both studies, total irradiation time was to be less than 10 weeks. Radiotherapy was withheld for grade 3 or 4 leukopenia and up to 1 week for gastrointestinal or genitourinary radiation-related toxicity. Statistical Analysis Age groups were dichotomized at 55 years owing to the disparity of cervical cancer incidence and mortality apparent in SEER cancer registries10 and then at 70 years owing to an apparent decrease in odds of chemotherapy use during radiation among patients with cervical cancer in the US SEER-Medicare cancer registry between 1998 and 2003.9 Age was dichotomized to facilitate comparison to 1998Y2003 US SEER-Medicare data that reflect cancer health service delivery to a highly skewed population of women aged 55 years or older.9 Several parameters of chemotherapy were evaluated in relation to age groups. Relative dose (RD) was the ratio of actual to expected dose of cisplatin in standard chemotherapy (40 mg/m2 6 cycles). Relative time (RT) was defined as the ratio of actual to expected duration of chemotherapy (6 weeks). Relative dose intensity (RDI) was defined as the ratio of RD to RT. A ratio lesser than 1.0 indicated patients received less intensity of chemotherapy than planned. Treatment completion was defined as completing 6 cycles of chemotherapy because this was the proposed number of cycles in the 2 GOG studies. Treatment * 2009 IGCS and ESGO Copyright @ 2009 by IGCS and ESGO. Unauthorized reproduction of this article is prohibited. 1259 International Journal of Gynecological Cancer Kunos et al TABLE 1. Patient characteristics by age group Characteristic Race White Black Other GOG performance status 0 1 or 2 Stage II III/IV Tumor grade 1 2 3 or not graded Histologic diagnosis Squamous Others Tumor size, cm G5 Q5 Parametrial involvement Unilateral Bilateral Pelvic node Positive Negative/not done Protocol treatment GOG 120 GOG 165 TABLE 2. Treatment parameters by age group G55 yr (n = 232), % Q55 yr (n = 103), % 56.5 25.4 18.1 66.0 19.4 14.6 0.083 71.6 28.5 65.1 35.0 0.233 62.9 37.1 60.2 39.8 0.634 9.1 59.1 31.9 5.8 60.2 34.0 0.597 87.9 12.1 85.4 14.6 0.529 48.7 51.3 66.0 34.0 0.003 56.9 43.1 61.2 38.8 0.465 16.4 83.6 6.8 93.2 0.018 53.5 46.6 50.5 49.5 P Pearson W2 method used to compare the difference in proportion between 2 groups. toxicities were graded as defined in previous clinical reports.3,4 Progression-free survival (PFS) was calculated from date of patient enrollment to the date of progression or recurrence of disease, death, or most recent follow-up visit. Overall survival (OS) was calculated from the date of patient enrollment to the date of death or last contact. The mean RD, RT, and RDI between patients younger than 55 years and patients aged 55 years or older were compared using Student t test. The number of treatment cycles, cause of treatment incompletion, and toxicity were compared by Pearson W2 test. The factors associated with treatment incompletion were identified using a logistic regression model. The cumulative probability of PFS or OS was estimated by Kaplan-Meier procedure, and the logrank test was used to compare the difference of the distribution between the 2 groups. All statistical analyses were 2 tailed (> = 0.05) and were performed using Statistical Analysis System software (SAS version 9.1; SAS Inc, Cary, NC). RESULTS Of 335 patients included for this analysis, median age was 49 years (range, 20Y80 years). Two hundred thirty-two patients were 1260 & Volume 19, Number 7, October 2009 Treatment Parameter RD* Mean (SD) Median (25thY75th Pct) RT‡ Mean (SD) Median (25thY75th Pct) RDI§ Mean (SD) Median (25thY75th Pct) No. treatment cycles, % 0 1 2 3 4 5 6 G55 yr (n = 232) Q55 yr (n = 103) P 0.85 (0.17) 0.84 (0.20) 0.830† 0.87 (0.79Y0.99) 0.88 (0.81Y0.97) 1.00 (0.27) 1.09 (0.79) 0.251† 1.00 (0.83Y1.14) 1.00 (0.83Y1.24) 0.87 (0.15) 0.86 (0.18) 0.547† 0.92 (0.79Y0.99) 0.94 (0.75Y0.98) 0.0 0.9 0.0 6.5 8.6 30.6 53.5 1.0 1.9 1.9 1.9 11.7 31.1 50.5 0.616|| *Ratio of actual to expected dose of chemotherapy. †Student t test use to compare the difference between 2 groups. ‡Ratio of actual to expected duration of chemotherapy. §Relative dose/RT. ||Pearson W2 used to compare the proportion of completion (53.5% vs 50.5%). younger than 55 years, and 103 patients were 55 years or older. There were 13 elderly patients (Q70 years) included in this analysis. There were no significant differences between the 2 age groups in the distributions of race, GOG performance status, clinical stage, tumor grade, tumor histologic diagnosis, or parametrial involvement. However, larger tumors (P = 0.003) or pelvic lymph nodes TABLE 3. Treatment-related adverse effects by age group Adverse Effect Grade 3 or 4 (selected) Leukopenia Thrombocytopenia Other hematological Gastrointestinal Genitourinary Neurological Cutaneous Any grade 3 or 4 G55 Yr (n = 232), % Q55 Yr (n = 103), % 22.0 2.2 12.1 18.1 6.5 1.7 2.6 47.8 32.0 1.0 21.4 19.4 1.9 1.0 50.5 2.90.656 P* 0.050 0.671 0.028 0.775 0.082 1.000 1.000 *Pearson W2 or Fisher exact method used to compare the difference in proportion between 2 groups. * 2009 IGCS and ESGO Copyright @ 2009 by IGCS and ESGO. Unauthorized reproduction of this article is prohibited. International Journal of Gynecological Cancer & Volume 19, Number 7, October 2009 with metastasis (P = 0.018) were observed more commonly among patients younger than 55 years (Table 1). Overall, 53% of patients completed 6 cycles of chemotherapy during radiation. The mean RD, RT, and RDI were 0.85, 1.03, and 0.87, respectively (Table 2). Patients younger than 55 years or 55 years or older were equally likely to finish 6 cycles of chemotherapy during radiation (54% vs 51%; P = 0.616), without differences in RD, RT, and RDI (Table 2). For the 13 elderly patients (Q70 years), 7 (54%) completed 6 cycles of chemotherapy during radiation. In this study population, 49% of patients reported at least 1 grade 3 or 4 adverse effect without difference between age groups younger than 55 years and 55 years or older. Although thrombocytopenia, genitourinary, and neurological and cutaneous toxicities were rare, a higher proportion of patients aged 55 years or older experienced leukopenia (32% vs 22%; P = 0.050) and other hematological (21% vs 12%; P = 0.028) toxicities during chemoradiation (Table 3). Nine (69%) of 13 patients aged 70 years or older experienced at least 1 grade 3 or 4 adverse effect. After controlling for other clinical factors and treatment protocol (Table 4), patients aged 55 years or older were no more TABLE 4. Factors associated with treatment incompletion Characteristic Incompletion, % OR (95% CI) 46.6 49.5 Referent 1.16 (0.71Y1.89) 43.3 60.8 45.2 Referent 2.13 (1.22Y3.74) 1.09 (0.61Y1.96) 45.9 51.0 Referent 1.27 (0.76Y2.11) 50.5 42.5 Referent 0.70 (0.43Y1.13) Age group, yr G55 Q55 Race White African American Other Performance status 0 1 or 2 Stage II III/IV Histologic diagnosis Squamous Others Tumor grade 1 2 3 Tumor size, cm e5 95 Parametrial involvement Unilateral Bilateral Pelvic node Positive Negative/not done P* 0.552 0.029 0.361 0.146 Referent 0.70 (0.36Y1.39) 44.4 45.7 51.4 Referent 1.13 (0.49Y2.61) 1.53 (0.64Y3.68) 49.2 45.5 Referent 0.85 (0.53Y1.34) FIGURE 1. Kaplan-Meier estimate of PFS for patients younger than 50 years and patients aged 50 years or older. likely to stop cisplatin chemotherapy during radiation as compared with patients younger than 55 years (odds ratio [OR], 1.16; 95% confidence interval [CI], 0.71Y1.89; P = 0.552). The only factor potentially affecting treatment completion was race, as AfricanAmerican patients had a greater frequency of not completing prescribed protocol therapy than white patients (OR, 2.13; 95% CI, 1.22Y3.74; P = 0.029). Reasons describing why a patient did not complete prescribed protocol therapy were not encoded for these clinical trials. At the time of this report, 169 patients showed disease progression, including 157 deaths. Median follow-up duration for patients still alive was 94 months, with a maximum follow-up of 169 months (25%Y75% quartile, 78Y123 months). At 5 years, 56% of patients younger than 55 years were predicted to be alive and disease-free compared with 55% of those aged 55 years or older (Fig. 1). The distribution of PFS was essentially the same (log-rank test: P = 0.629). There was also no significant difference in OS between the 2 groups (log-rank test: P = 0.265), with a 5-year survival of 60% in patients younger than 55 years compared with 56% in patients aged 55 years or older (Fig. 2). DISCUSSION 0.310 48.6 39.5 Chemoradiation in Women Aged 55 Years or Older This report confirmed that in the cooperative group, clinical trial setting, chemoradiation administration, toxicity, and outcome of patients with cervical cancer aged 55 years or older are similar to 0.406 0.481 0.580 49.2 45.0 Referent 0.87 (0.54Y1.42) 48.3 42.2 Referent 0.81 (0.41Y1.57) 0.524 *Odds ratio estimated by Logistic regression model, adjusted for covariates and protocol. FIGURE 2. Kaplan-Meier estimate of OS for patients younger than 50 years and patients aged 50 years or older. * 2009 IGCS and ESGO Copyright @ 2009 by IGCS and ESGO. Unauthorized reproduction of this article is prohibited. 1261 Kunos et al International Journal of Gynecological Cancer patients of younger age. Given that chemoradiation use for locally advanced cervical cancer has risen steadily because of publication of 5 chemoradiation clinical trials, patients aged 55 years or older were expected to have similar risks of cancer-related relapse or death as compared with patients younger than 55 years.4Y8 For given tumor and demographic factors for patients enrolled in GOG Nos. 120 and 165, patients aged 55 years or older were just as likely to complete all recommended chemotherapy treatments during radiation as patients of younger age. Retrospective analyses of population-based cancer registries have not encoded detailed chemotherapy administration records. Unlike population-based cancer registry studies, this retrospective analysis of 2 cooperative group clinical trials offered reliable abstraction of the exact regimen of chemotherapy administration, patient-specific chemotherapy dosage, and adverse effects of treatment. In this study, ratios of actual delivered chemotherapy dose to expected dose, actual to expected time of chemotherapy delivery, and RD to RT were determined for GOG protocols Nos. 120 and 165. The observed RD, RT, and RDI were similar among treated patients regardless of age (Table 2), even among the limited number of patients aged 70 years or older. Certainly, this finding is open to interpretive criticism. Not only patients participating in clinical trials are often highly motivated to complete protocol prescription therapy, but also physicians are highly motivated to have their patients complete all protocol prescription therapy. For instance, in the 1998Y2002 SEER-Medicare population cervical cancer registry, only 47% of patients aged 55 years or older treated for locally advanced cervical cancer with radiation received at least 5 cycles of concomitant chemotherapy.9 A significant decreased odds of radiation and chemotherapy administration in patients aged 71 years or older was also observed.9 By comparison, 84% of patients younger than 55 years and 82% of patients aged 55 years or older completed at least 5 cycles of chemotherapy in GOG protocol Nos. 120 and 165. Perhaps, patient and physician motivations and possibly overall ancillary treatment support provided by controlled cooperative group clinical trials accounts for the disparity in chemotherapy use during radiation administration among SEERMedicare and GOG patient populations. In previous retrospective analyses, it has been noted that physician bias, attributed to elderly patient moderate-to-severe medical comorbidity, adversely impacts allocation of primary and adjuvant therapies for patients with cancer.12,15Y17 In this report, there was not an overall excess incidence of treatment-related toxicity in patients aged 55 years as compared with younger patients (Table 3). For patients aged 55 years or older, the proportion of those alive and free of disease was similar to younger patients, at a cost of an increased incidence of manageable grade 3 and higher hematological toxicity. Growth factors were not used in either GOG protocol Nos. 120 or 165 and, perhaps, with further study in the 55-year or older patient population, could lessen hematological toxicity. Genitourinary toxicity was not higher in patients aged 55 years or older despite the more probable increased incidence of impaired renal function in these patients. While treatment-related toxicity was not a barrier to finishing chemotherapy, there was a disparity in the proportion of AfricanAmerican patients not completing prescribed chemotherapy during radiation. Among African-American patients, there was not an identifiable treatment-related factor or toxicity associated with not completing prescribed therapy. For GOG Nos. 120 and 165, compelling evidence explaining the observed disparity of treatment completion was not identified in multivariate analyses.14 Radiation dose and brachytherapy technique were different in GOG Nos. 120 and 165, but too few patients (21 enrolled on GOG 165 [6%] of the 335 total studied here) underwent highYdose rate brachytherapy to comment.3 Perhaps, one explanation could be found among 1262 & Volume 19, Number 7, October 2009 differences in poverty and education levels, as these factors have been associated with lower likelihoods of completing prescribed therapy, which translates into poorer survival.18Y20 In population studies using SEER cancer incidence data, disparity between 5-year survival rates were 7% between low and high poverty and 7% between low and high education census tracts.18 Among patients studied for this analysis, reliable proxy indicators of socioeconomic and educational statuses were not readily coded for analysis and, thus, cannot be commented upon as contributing factors to incomplete protocol treatment administration. With a median follow-up of 94 months among survivors, patients aged 55 years or older were not more likely to relapse or die of cervical cancer as compared with patients younger than 55 years when radiosensitizing doses of cisplatin chemotherapy were administered. Within the cohorts aged 55 years or older and younger than 55 years of GOG Nos. 120 and 165, subpopulations do fare better, as a nonlinear association between age and survival has been observed with patients aged 51 to 60 years having a better prognosis than those patients aged 40 years or younger.14 As such, substantial gains in PFS and OS observed for patients in these cohorts perhaps may only be applicable when cisplatin chemotherapy is used. Concurrent weekly cisplatin with pelvic radiation significantly improves long-term PFS and OS as compared with radiation alone for patients with cervical cancer.4Y6 Whether other radiosensitizing chemotherapeutic agents achieve these gains remains unanswered. For patients aged 55 years or older who do not receive cisplatin chemotherapy owing to medical comorbidity or lack of administrative ability, other agents that can be safely and reliably given during radiation should be studied. The GOG and other large cooperative groups continue to refine the optimal regimen for chemoradiation in the treatment of patients with locally advanced cervical cancer. REFERENCES 1. Waggoner SE. Cervical cancer. Lancet. 2003;361:2217Y2225. 2. Stehman FB, Bundy BN, DiSaia PJ, et al. Carcinoma of the cervix treated with radiation therapy: a multivariate analysis of prognostic variables in the Gynecologic Oncology Group. Cancer. 1991;67: 2776Y2785. 3. Lanciano R, Calkins A, Bundy BN, et al. Randomized comparison of weekly cisplatin or protracted venous infusion of fluorouracil in combination with pelvic radiation in advanced cervix cancer: a Gynecologic Oncology Group Study. J Clin Oncol. 2005;23: 8289Y8295. 4. Rose P, Ali S, Watkins E, et al. Long-term follow-up of a randomized trial comparing concurrent single agent cisplatin, cisplatin-based combination chemotherapy, or hydroxyurea during pelvic irradiation for locally advanced cervical cancer: a Gynecologic Oncology Group Study. J Clin Oncol. 2007;25:2804Y2810. 5. Eifel PJ, Winter K, Morris M, et al. Pelvic irradiation with concurrent chemotherapy versus pelvic and para-aortic irradiation for high-risk cervical cancer: an update of radiation therapy oncology group trial (RTOG) 90-01. J Clin Oncol. 2004;22:872Y880. 6. Stehman FB, Ali S, Keys HM, et al. Radiation therapy with or without weekly cisplatin for bulky stage 1B cervical carcinoma: follow-up of a Gynecologic Oncology Group trial. Am J Obstet Gynecol. 2007;197:503.e1Y6. 7. Whitney CW, Sause W, Bundy BN, et al. Randomized comparison of fluorouracil plus cisplatin versus hydroxyurea as an adjunct to radiation therapy in stage IIB-IVA carcinoma of the cervix with negative para-aortic lymph nodes: a Gynecologic Oncology Group Study. J Clin Oncol. 1999;17:1339Y1348. 8. Peters WI, Liu P, Barrett R, et al. Concurrent chemotherapy and pelvic radiation therapy compared with pelvic radiation therapy alone as adjuvant therapy after radical surgery in high-risk early-stage cancer of the cervix. J Clin Oncol. 2000;18:1606Y1613. * 2009 IGCS and ESGO Copyright @ 2009 by IGCS and ESGO. Unauthorized reproduction of this article is prohibited. International Journal of Gynecological Cancer & Volume 19, Number 7, October 2009 9. Kunos C, Gibbons H, Simpkins F, et al. during pelvic radiation for cervical cancer patients aged Q55 years in the SEER-Medicare population. J Oncol. 2008: 931532. Epub August 27, 2008. 10. National Cancer Institute Cancer Statistics Branch. SEER Cancer Statistics Review 1975Y2002 Tables 1Y10 and 1Y12, 2005 (vol 2007). http://seer.cancer.gov/csr/1975_2002. Accessed April 1, 2009. 11. Eifel PJ, Moughan J, Erickson B, et al. Patterns of radiotherapy practice for patients with carcinoma of the uterine cervix: a patterns of care study. Int J Rad Oncol Biol Phys. 2004;60:1144Y1153. 12. Wright J, Gibb R, Geevarghese S, et al. Cervical carcinoma in the elderly: an analysis of patterns of care and outcome. Cancer. 2005;103: 85Y91. 13. Mitchell P, Waggoner S, Rotmensch J, et al. Cervical cancer in the elderly treated with radiation. Gynecol Oncol. 1998;71:291Y298. 14. Monk BJ, Tian C, Rose PG, et al. Which clinical/pathologic factors matter in the era of chemoradiation as treatment for locally advanced cervical carcinoma? Analysis of two Gynecologic Oncology Group (GOG) trials. Gynecol Oncol. 2007;105:427Y433. Chemoradiation in Women Aged 55 Years or Older 15. Neugut AI, Fleischauer AT, Sundarajan V, et al. Use of adjuvant chemotherapy and radiation therapy for rectal cancer among the elderly: a population-based study. J Clin Oncol. 2002;20:2643Y2650. 16. Yancik R, Wesley MN, Ries LA, et al. Effect of age and comorbidity in postmenopausal breast cancer patients aged 55 years and older. JAMA. 2001;285:885Y892. 17. Samet J, Hunt WC, Key C, et al. Choice of cancer therapy varies with age of patient. JAMA. 1986;255:3385Y3390. 18. Singh GK, Miller BA, Hankey BF, et al. Persistent area socioeconomic disparities in U.S. incidence of cervical cancer, mortality, stage and survival, 1975Y2000. Cancer. 2004;101:1051Y1057. 19. Coker AL, Du XL, Fang S, et al. Socioeconomic status and cervical cancer survival among older women: findings from the SEER-Medicare linked data cohorts. Gynecol Oncol. 2006;102:278Y284. 20. Patel DA, Barnholtz-Sloan JS, Patel MK, et al. A population-based study of racial and ethnic differences in survival among women with invasive cervical cancer: analysis of surveillance, epidemiology, and end results data. Gynecol Oncol. 2005;97:550Y558. * 2009 IGCS and ESGO Copyright @ 2009 by IGCS and ESGO. Unauthorized reproduction of this article is prohibited. 1263