Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
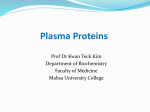
LIVER FAILURE/CIRRHOSIS/PORTAL HYPERTENSION Alterations in the Functional Capacity of Albumin in Patients with Decompensated Cirrhosis Is Associated with Increased Mortality Rajiv Jalan,1 Kerstin Schnurr,2 Rajeshwar P. Mookerjee,1 Sambit Sen,1 Lisa Cheshire,1 Stephen Hodges,1 Vladimir Muravsky,2 Roger Williams,1 Gert Matthes,2,3 and Nathan A. Davies1 Albumin concentration is diminished in patients with liver failure. Albumin infusion improves survival of cirrhotic patients with spontaneous bacterial peritonitis, and it is hypothesized that this may be due in part to its detoxifying capabilities. The aim of this study was to perform detailed quantitative and qualitative assessment of albumin function in patients with cirrhosis. Healthy controls and patients with acute deterioration of cirrhosis requiring hospital admission (n ⴝ 34) were included. Albumin function was assessed using affinity of the fatty acid binding sites using a spin label (16 doxyl-stearate) titration and electron paramagnetic resonance spectroscopy and ischemia-modified albumin (IMA) was measured. Twenty-two patients developed acute-on-chronic liver failure. Twelve were treated with the Molecular Adsorbents Recirculating System (MARS) and 10 with standard medical therapy. For each parameter measured, the patients’ albumin had reduced functional ability, which worsened with disease severity. Fifteen patients died, and IMA, expressed as an albumin ratio (IMAR), was significantly higher in nonsurvivors compared with survivors (P < 0.001; area under the receiver operating curve ⴝ 0.8). No change in the patients’ albumin function was observed following MARS therapy. A significant negative correlation between IMAR and the fatty acid binding coefficients for sites 1 and 2 (P < 0.001 for both) was observed, indicating possible sites of association on the protein. Conclusion: The results of this study suggests marked dysfunction of albumin function in advanced cirrhosis and provide further evidence for damage to the circulating albumin, which is not reversed by MARS therapy. IMAR correlates with disease severity and may have prognostic use in acute-on-chronic liver failure. (HEPATOLOGY 2009;50:555-564.) See Editorial on Page 355 Abbreviations: ACLF, acute-on-chronic liver failure; AUROC, area under the receiver operating curve; EPR, electron paramagnetic resonance; IMA, ischemiamodified albumin; IMAR, IMA/albumin ratio; MARS, Molecular Adsorbents Recirculating System; MELD, model of end-stage liver disease. From the 1Liver Failure Group, Institute of Hepatology, University College London, London, United Kingdom; 2MedInnovation GmbH, Wildau, Germany; and the 3Institute of Transfusion Medicine, University Hospital Leipzig, Leipzig, Germany. Received October 28, 2008; accepted February 9, 2009. Supported by The Seigmund Warburg Benevolent fund and by an unrestricted grant from CSL Behring Grifols; and Talecirs; and BPL (for supplying Human Serum Albumin); coordinated by the Plasma Proteins Therapeutic Association. This work was undertaken at UCLH/UCL, who received a proportion of funding from the Department of Health’s NIHR Biomedical Research Centres funding scheme. The views expressed in this work are those of the authors and not necessarily those of the Department of Health. Address reprint requests to: Nathan Davies, Liver Failure Group, Institute of Hepatology, 69-75 Chenies Mews, University College London, London WC1E 6HX, United Kingdom. E-mail: [email protected]; fax: (44)-2073800405. Copyright © 2009 by the American Association for the Study of Liver Diseases. Published online in Wiley InterScience (www.interscience.wiley.com). DOI 10.1002/hep.22913 Potential conflict of interest: Nothing to report. A lbumin is the major plasma protein and constitutes around 50% of the cell free protein in healthy individuals. It is produced exclusively in the liver, and therefore its concentration is reduced during hepatic dysfunction.1 Following the Cochrane meta-analysis describing potential harmfully effect of albumin infusion in critically ill patients, there has been a reexamination of the use of albumin infusions for volume replacement. However, the results of the recently published SAFE study have provided new data confirming the safety of albumin infusion in critically ill patients.2,3 Liver failure results in multiple organ dysfunction, and mortality rates without liver transplantation remain unacceptably high.4 However, recovery is associated with complete reversal of multiorgan dysfunction. At present, in patients with cirrhosis, albumin is used mainly to replenish the circulating volume. With increasing severity of cirrhosis, there is a progressive increase in cardiac output, which is associated with a progressive reduction in individual organ blood flow. This peculiar circulatory disturbance is thought to occur as a result of splanchnic 555 556 JALAN ET AL. Fig. 1. A diagrammatic representation of the functional albumin domains. BS-1, BS-2, BS-3, and BS-4 represent the functional fatty acid binding sites; N terminus represents the Cu/Zn metal binding domain; and Cys 34 represents the antioxidant property of albumin. vasodilatation that culminates in a reduction of effective arterial blood volume.5 In patients with cirrhosis, albumin infusion prevents the postparacentesis circulatory disturbance in patients undergoing total abdominal paracentesis and reduces mortality in patients with spontaneous bacterial peritonitis.6 In a separate study, patients with hepatorenal syndrome treated with Terlipresssin plus albumin showed a significant improvement in outcome compared with patients treated with Terlipressin alone.7 These effects of albumin were interpreted to be due to its ability to produce adequate volume expansion, thereby preserving renal circulation.6,7 Albumin has been shown to undertake a variety of functions including fatty acid transport, metal chelation, drug binding and anti-oxidant activity. These functions are achieved through its antioxidant property provided by the thiol moiety at cys-34 and several important binding sites (Fig. 1).1 It is likely that it is this antioxidant and the detoxification property of albumin that was associated with improved outcome of stroke patients that received albumin infusion compared with standard of care.8 Indeed, a recent study described functional disturbances in the antioxidant function of albumin in patients with liver failure.9 It is this functional property of albumin that has been exploited by the detoxification systems based upon the principles of albumin dialysis. One such device that is commercially available is the Molecular Adsorbents Recirculating System (MARS) (Gambro, Lund, Sweden) and studies using this device show beneficial pathophysiological and clinical effects particularly in reducing the HEPATOLOGY, August 2009 severity of hepatic encephalopathy with small studies also showing possible survival benefit in liver failure patients.10-12 However, at present, detailed functional characteristics of the different binding sites in cirrhosis have not been determined. The overall aim of this study was to perform a detailed qualitative and quantitative assessment of the functional capacity of albumin in patients with liver disease of varying severities and to determine whether these alterations could be used as a marker of disease severity and prognosis. We chose to use two methods of testing albumin functionality. Electron paramagnetic resonance (EPR) spectroscopy was used to perform detailed analyses of the individual binding sites that are associated with the main function of albumin. Ischemia-modified albumin,13 a test that measures the cobalt-binding capacity of albumin, was measured in the same cohort to determine whether this simpler test could be used as a biomarker to determine prognosis in patients with acute-on-chronic liver failure (ACLF). In addition, we wanted to determine whether dialysis against an albumin solution using the MARS system has any ability to affect albumin functional capacity in patients with ACLF. Patients and Methods All patients gave written informed consent, and the study was approved by the local ethics committee. Patients Thirty-four patients with alcoholic cirrhosis defined on clinical, radiological, biochemical, and/or histological grounds were enrolled in the study. Included patients had been admitted with acute decompensation of cirrhosis manifested by increasing jaundice. Prophylactic antibiotics (cefotaxime) were prescribed following initial cultures if there was a suspicion of infection, and stopped if subsequent cultures proved negative. Patients were excluded if they were under 18 years of age or over 75 years of age, had hyponatremia, had a hepatic/extrahepatic malignancy, had fewer than 3 days of post-gastrointestinal bleeding, or if they received any immunomodulatory therapy or albumin infusion prior to entry in the study. The reference population of 80 healthy volunteer blood donors (reference control [n ⫽ 80]) served as controls. All patients received supportive therapy including nutrition and vitamin supplementation according to local guidelines. Local treatment protocols were initiated for development of complications including, sepsis, hepatorenal syndrome, and organ failure (full intensive care support), as indicated. Twelve of the 34 patients were included following correction of any electrolyte disturbances or hypovolemia HEPATOLOGY, Vol. 50, No. 2, 2009 and 48 hours after initiation of specific therapy to treat the precipitating event, and this group served as disease controls. The other 22 patients were included on the day they were admitted to the intensive care unit with a diagnosis of ACLF, which was defined as acute deterioration in liver function over a period of 2 to 4 weeks, associated with a precipitating event, leading to severe deterioration in clinical status, with jaundice and hepatic encephalopathy (grade 2 or more) and/or hepatorenal syndrome, with a sequential organ failure assessment score of 8 or more. Of these 22 patients, 12 were treated with the molecular adsorbents recirculating system and 10 with standard supportive medical therapy. The selection for treatment with MARS or standard of care was decided randomly as a part of other clinical studies (unpublished data). Samples from patients with cirrhosis without organ failure were collected from patients within 48 hours of admission, after initiation of therapy for their precipitating event. Study Design Peripheral venous blood was aseptically collected into pyrogen-free tubes (BD Vacutainer Lithium-Heparin [60 U per tube]; BD, Plymouth, UK) at the time of inclusion into the study and used for routine biochemistry, markers of oxidative stress, and albumin functional capacity. For harvesting plasma, blood was placed immediately on ice. After centrifugation, plasma was aliquoted into cryotubes (Corning Inc., Corning B.V., Netherlands) and stored at ⫺80°C until further analysis. Bilirubin, albumin, liver function tests, coagulation parameters, full blood count, and c-reactive protein were routinely performed. model of end-stage liver disease (MELD)14 and Pugh score15 were calculated. The patients were followed prospectively over a period of 90 days. In the patients that developed ACLF, plasma samples were collected again 7 days after inclusion. Measurement of Albumin Function The functional characteristics of albumin were measured using two techniques. The molecular structure is shown in Fig. 1 which also depicts the binding sites studied. Electron Paramagnetic Resonance. The functional capacity of the albumin binding sites were measured using a spin label and electron paramagnetic resonance spectroscopy as described.16,17 There are six well-known binding sites for fatty acids on the albumin molecule, three with high and three with lower affinity, that were examined in this study. The spin label used for albumin 16doxyl stearic acid (Sigma-Aldrich GmbH, Germany) was added to plasma samples in defined concentrations. Ethanol was used as a polar reagent (99% puriss, USPXXII, JALAN ET AL. 557 Merck KG, Germany), increasing aliquots of which were added to the labeled plasma samples, which were then incubated at 37°C for 10 minutes before the EPR spectra were recorded (MMS, MedInnovation GmbH, Germany). Analysis of the recorded spectra, using MMS software, provided information on albumin conformation and binding properties. Two different situations were considered: (1) in vitro conditions, which included noncompetitive examination of fatty acid adsorption, transport capacity, and fatty acid unloading; and (2) a competitive test that simulated in vivo conditions in which albumin loading, transport and unloading were studied for the functional parameters of albumin quality as transport drug in competitive situations. Using EPR spectroscopy, albumin conformational modifications can be determined from its interaction with other ligands. The EPR spectra-based parameters (KB1, binding coefficient, and N1, capacity of high-affinity sites; KB2, binding coefficient, and N2, capacity of secondary binding sites; RTE, real transport efficiency; DTE, detoxification efficiency) allow conclusions to be made as to the extent of maintained transport of fatty acids, drugs, bilirubin, metabolites, biomarkers, and so forth. In addition, it is possible to assess the detoxification function of measured albumin.16,17 Ischemia-Modified Albumin. Ischemia-modified albumin (IMA) is identified using an assay to determine the ability of the protein to chelate cobalt. There are several sites on the protein that have the ability to bind metals, though most interest to date has focused on the N-terminal region.13,18 IMA was determined according to the cobalt-binding assay method of Bhagavan et al.13 Briefly, plasma was incubated with a cobalt chloride (1 g/L, 10 minutes) and dithiothreitol (1.5 g/L, 2 minutes) before dilution in saline prior to measurement at 470 nm in a spectrophotometer (Agilent 8453 Diode Array, Agilent, UK). IMA was calculated from the difference between samples measured with and without dithiothreitol. Plasma albumin concentration was determined using an automated COBAS Integra biochemical analyzer (Roche Diagnostics, UK). Markers of Oxidative Stress Malondialdehyde. Malondialdehyde (MDA) was determined using a modified thiobarbituric acid reactive substances assay described by Lapenna et al.19 wherein the major interfering/oxidizable component in the plasma is inhibited by addition of sodium sulphate. F2 Isoprostanes. F2 isoprostanes (free 8-isoprostane F2␣) was assayed with a commercial EIA kit (Cayman Chemical, Ann Arbor, MI) according to the manufacturer’s instructions and as described.20 Briefly, 200 L 558 JALAN ET AL. plasma was deproteinized with 600 L ethanol containing 3H-prostaglandin E2 as an internal standard to account for losses. After centrifugation, the supernatant was reduced to near dryness, and 2 mL acetic acid was added and applied to a preconditioned C18 SPE cartridge (Waters, Milford, MA). The column was washed with water, dried with nitrogen, and eluted with high-performance liquid chromatography– grade hexane. The prostanoid fraction was eluted with 5 mL ethylacetate containing 1% methanol, eluant reduced to dryness and reconstituted in 450 L of EIA buffer, 100 L being used to determine recovery of 3H-PGE2 and 50 L added to the EIA plate with isoprostane tracer and antibody. Isoprostane levels were determined by reference to authentic standards and corrected for losses. Statistical Analysis All the data were described as mean and standard error. Differences between groups were calculated using an independent samples t test for the normally distributed data and the Mann-Whitney test for data not normally distributed. Correlations between variables were calculated using linear regression. Survival analysis was performed using the Kaplan-Meier method and the log-rank test was used to test statistical significance. Results Patients The main causes leading up to acute decompensation in the patients were infection (n ⫽ 18), superimposed alcoholic hepatitis (n ⫽ 11), and variceal bleeding (n ⫽ 5). Twenty-two patients proceeded to deterioration in their clinical condition requiring prolonged hospital admission and supportive care in a high-dependency/intensive care unit and were considered to have ACLF. Of these, 12 were treated with MARS and the rest with standard of care. No clinical or biochemical differences were observed between the patients treated with MARS compared with the group treated with standard medical care. In the MARS-treated patients, there was a reduction in bilirubin (P ⬍ 0.01) and creatinine (P ⬍ 0.05) concentrations at day 7, which resulted in a reduction in MELD score. However, although this would suggest an improvement in outcome, survival remained unaffected, with eight of the 12 patients dying in the MARS group and 7 of the 10 patients dying in the group treated with standard of care (Table 1). The cause of death was multiorgan failure in both groups. Albumin Function Electron Paramagnetic Resonance. Albumin functionality is characterized by four groups of EPR spectrum HEPATOLOGY, August 2009 Table 1. Patient Characteristics Age Sex MELD score Child-Pugh score SOFA score Albumin (g/L) Bilirubin (mol/L) INR Creatinine (mol/L) MDA (mol/L) F2-Isoprostanes (pg/mL) In-hospital mortality Cirrhosis, No Organ Dysfunction (n ⴝ 12) ACLF Treated with MARS (n ⴝ 12) ACLF Treated with SMT (n ⴝ 10) 47 ⫾ 3.4 10 M, 2 F 9.3 ⫾ 2* 7.9 ⫾ 1.3† 5.5 ⫾ 1.2† 37 ⫾ 4† 83 ⫾ 9‡ 1.2 ⫾ 0.2‡ 73 ⫾ 8‡ 3.3 ⫾ 2.1† 267 ⫾ 32† None 47 ⫾ 4.4 9 M, 3 F 19.7 ⫾ 3 11.4 ⫾ 1.5 9.3 ⫾ 2.5 26 ⫾ 1.7 428 ⫾ 57 1.8 ⫾ 0.2 146 ⫾ 41 7.4 ⫾ 1.9 423 ⫾ 39 8 patients 48 (2.9) 8 M, 2 F 20 ⫾ 3 12.2 ⫾ 1.4 9.4 ⫾ 1.7 25 ⫾ 1.3 323 ⫾ 47 1.8 ⫾ 0.1 179 ⫾ 67 7.7 ⫾ 2.3 489 ⫾ 28 7 patients Data are expressed as the mean ⫾ standard error. Abbreviations: F, female; INR, international normalized ratio; M, male; SMT, standard medical therapy; SOFA, sequential organ failure assessment. *P ⬍ 0.05, †P ⬍ 0.01, ‡P ⬍ 0.001 for the cirrhosis, no organ dysfunction group versus the ACLF groups. parameters: Albumin functionality is characterized by three groups of EPR spectrum parameters: (1) capacity of binding sites and strength of fatty acid holding; (2) global parameters of albumin transport (transport, loading, and unloading of fatty acids); and (3) functional parameters of albumin quality in regard to its ability to uptake and hold toxic substances produced via metabolism. The EPR data of the healthy subjects were used as reference values. All healthy volunteers showed normal albumin conformation and transport functionality. Examination of the data obtained from the 80 control subjects showed no significant differences in any measured value for either age or sex (Fig. 2). For each parameter measured, patients with both stable cirrhosis and those with ACLF were significantly worse compared with the healthy volunteers. Transport Efficiency. Albumin transport function parameters were evaluated following the model of a threestep transport process for fatty acids. This incorporates substrate sorption and binding parameters in which albumin from healthy subjects demonstrate high binding constants for substrate uptake. The second phase is transfer of the bound substrates into the circulatory system. Finally, the albumin should be able to demonstrate the ability to release the substrate to target objects. Substrate delivery from albumin requires albumin receptor or albumin surface interaction with the cell membrane; in this process, the albumin substrate binding constant is controlled by hydrophobic interactions at the target binding site. In the EPR studies, the local albumin membrane delivery operations were simulated using ethanol for modification of these hydrophobic interactions. Overall, the albumin transport efficiency in ACLF patients was found to be only about 10% of the normal functional ability of albu- HEPATOLOGY, Vol. 50, No. 2, 2009 JALAN ET AL. 559 Within these measures, cirrhotic patients were found to have significantly lower (P ⬍ 0.001, KB1 and P ⬍ 0.001, KB2) fatty acid binding capability compared with healthy controls. This ability was then further reduced in patients with acute decompensation. Albumin detoxification efficiency for uptake of toxins was evaluated to show the fixation of toxins and a minimal dissociation rate of albumin as the ratio of albumin sorption capability compared with its delivery efficiency. In this measure it was found that healthy controls had a significantly better calculated detoxification capacity compared with stable cirrhotic subjects (P ⬍ 0.001), which was in turn significantly higher than that of ACLF patients (P ⬍ 0.05). The detoxification efficiency was significantly lower in nonsurvivors compared with survivors (P ⬍ 0.007) (Table 2). The detoxification efficiency correlated closely with transport efficiency (r ⫽ 0.93; P ⬍ 0.0001). Effective Albumin Concentration. From these results, it was possible to derive an effective albumin concentration that revealed that cirrhotic subjects had significantly lower functionality than healthy controls (P ⬍ 0.001). This functionality was again found to be reduced further in the ACLF group compared with the cirrhotic, no organ dysfunction group (P ⬍ 0.05) (Table 3). Ischemia Modified Albumin. It was not possible to differentiate between groups using the IMA results due to the wide variance in the values obtained. However, when the IMA values were considered relative to the patients’ Fig. 2. Functional alterations in albumin obtained from the reference population of healthy volunteers. (A) Relationship between age and real transport efficiency (RTE). (B) Relationship between age and detoxification efficiency (DTE). In each case the lines indicate the line of best fit (linear regression) for the data, and the line was not found to be significantly different from zero. (C) The measurements of albumin functionality were sex-independent (black bars, males; white bars, females). min from healthy volunteers (Table 2). These values were found to be significantly lower in cirrhotic patients compared with healthy controls (P ⬍ 0.001 in each case) and were further reduced in ACLF subjects. Transport efficiency was significantly lower in nonsurvivors compared with survivors (P ⬍ 0.05). Detoxification Efficiency. Albumin screening parameters were evaluated using concentration parameters of free fatty acid and 16-DS bound to albumin. The measured binding capacity was significantly reduced in subjects with liver disease compared with healthy controls (P ⬍ 0.05). This finding demonstrates that the threedimensional protein structure of the albumin is affected in patients with liver disease. Table 2. Functional Albumin Parameters in Different Patient Groups Measure EPR spectroscopy Binding coefficient (highaffinity KB1) Number of labels (highaffinity site, N1) Binding coefficient (lowaffinity KB2) Number of labels (lowaffinity site, N2) Calculated real transport efficiency Calculated detoxification efficiency Effective albumin IMA IMAR Healthy Cirrhosis, No Organ Dysfunction (n ⴝ 12) ACLF (n ⴝ 22) 97.4 (15.6) 27.5 (5.6)* 17.9 (3.5)* 3.1 (0.1) 2.4 (0.1) 2.5 (0.9) 58.3 (11) 20.1 (3.1)* 14.1 (1.8)*,† 2.9 (0.2) 3.1 (0.1) 2.6 (0.1)*,† 75 (6.9) 27.5 (5.1)* 14.3 (1.9)*,† 120 (33) 50.26 (3.02) 0.69 (0.034) 0.010 (0.001) 28.2 (5.3)* 25.6 (3.1)* 0.64 (0.022) 0.021 (0.001) 11.6 (2.6)*,‡ 20.98 (2.2)* 0.64 (0.017) 0.03 (0.002)*,‡ Data are expressed as the mean (standard error). See text for explanations regarding the description of the various binding sites. *P ⬍ 0.001 compared with healthy volunteers; †P ⬍ 0.05, ‡P ⬍ 0.01 compared with cirrhosis, no organ dysfunction group. 560 JALAN ET AL. HEPATOLOGY, August 2009 Table 3. Characteristics of Survivors versus NonSurvivors Factor MELD score Child-Pugh score SOFA score Real transport efficiency Detoxification efficiency IMAR Survivors (n ⴝ 19) Nonsurvivors (n ⴝ 15) P Value AUROC 13.1 (1.5) 9.4 (0.9) 7.1 (2.3) 19.5 (2.2) 11 (0.4) 9.5 (1.2) ⬍0.05 0.3 ⬍0.01 0.76 0.66 0.74 26.2 (4) 22.5 (4.4) 0.020 (0.001) 14.9 (2.7) 12.2 (2.9) 0.033 (0.003) ⬍0.05 ⬍0.01 ⬍0.01 0.65 0.72 0.80 Data are expressed as mean (standard error). Abbreviation: SOFA, sequential organ failure assessment. plasma albumin levels, significant differences were observed. The IMA/albumin ratio (IMAR) was significantly higher in ACLF patients (P ⬍ 0.05, Table 2). Regression analyses comparing the binding constants determined using the spin label studies and the measured IMAR scores found a significant relationship at both binding sites 1 and 2. Similar significance levels were found between the IMAR and the log10 derivative values from BS1 and BS2 (IMAR versus logKB1, r ⫽ 0.6; IMAR versus logKB2, r ⫽ 0.62; P ⬍ 0.001 for both) (Fig. 3), indicating a relationship between the inability of cobalt to bind to the protein and the function of these sites. Higher IMAR correlated closely with the MELD score (r ⫽ 0.81; P ⬍ 0.007) (Fig. 4) but not Child-Pugh score. IMAR levels were significantly higher in nonsurvivors compared with survivors (area under the receiver operating curve [AUROC]: 0.8) (Fig. 5). With a cutoff ratio value of 0.02, the sensitivity and specificity were 83% and 67% respectively. Kaplan-Meier analysis confirmed increased mortality in the group with an IMAR ⬎0.02; log-rank: P ⫽ 0.03) (Fig. 6). during the study period, this difference was not statistically significant. Discussion This study provides the first detailed description of the qualitative and quantitative reduction in albumin function in patients with liver disease. The data indicate that the ability of albumin to transport protein-bound substances and drugs and act as detoxification agent is severely compromised in patients with cirrhosis, and is further reduced in patients with ACLF. Additionally, our data suggest that the severity of the functional abnormalities of albumin function measured by IMAR may be a useful biomarker to determine survival of patients with acute decompensation of cirrhosis, though this will be dependent on an appropriately powered validation study. From the pathophysiologic perspective, the increase in IMAR levels with disease severity provides evidence of protein modification, which in keeping with the published literature has been shown to be associated with severity of oxidative stress.21,22 The use of EPR spectra provides data regarding changes in fatty acid binding of serum albumin under modulation of medium hydrophilicity and allows conclusions for transport and detoxification capacity of this integral plasma protein.16,17,21 The efficiency of the Markers of Oxidative Stress MDA and F2 isoprostanes were significantly higher in the ACLF group compared with the group that did not develop organ failure (P ⬍ 0.05 and P ⬍ 0.01, respectively) (Table 1). MDA was insignificantly higher in nonsurvivors, but F2 isoprostanes were significantly greater in nonsurvivors compared with survivors (P ⬍ 0.05). IMAR correlated significantly with MDA (r ⫽ 0.67; P ⬍ 0.01) and F2 isoprostanes (r ⫽ 0.6; P ⬍ 0.05), but the relationship with the detoxification efficiency and transport efficiency were statistically insignificant. Effect of MARS Therapy on Albumin Function No significant differences in albumin function were found between days 0 and 7 for the ACLF patients in either the SMT or MARS groups (Fig. 7). Although it appears that in the SMT group the effective albumin concentration and detoxification efficiency measures improve Fig. 3. There was good correlation between the binding coefficients (KB1 and KB2) at binding sites 1 and 2 with IMAR. HEPATOLOGY, Vol. 50, No. 2, 2009 Fig. 4. Relationship between IMAR and MELD score. Regression analysis yielded r2 ⫽ 0.65 and P ⬍ 0.007. albumin transport system depends on two factors. In the case of decreased transport function and detoxification efficiency, it signifies modification of the albumin molecule. This may be due to the binding/accumulation of low molecular hydrophobic compounds (toxins, drugs, and so forth) or permanent modifications to the albumin that have occurred, rendering the protein incapable of normal function. This loss of function is highlighted by the reduction in the measured binding constant (KB) for the spin label observed in cirrhotic patients. This finding indicates a reduced ability of the albumin to bind and hold the materials to be transported within the body. Coupled with a decreased binding capacity (number of labels per albumin molecule), this indicates that these materials are Fig. 5. Receiver operator curve analysis of IMAR scores to examine its predictive use for assessing mortality (AUROC ⫽ 0.8). JALAN ET AL. 561 Fig. 6. Kaplan-Meier analysis of outcome based on a cutoff value of 0.02, as determined from the AUROC analysis shown in Fig. 4. A significant difference in survival was observed (P ⬍ 0.03). more likely to exist as a free component within the vasculature with the ability to react arbitrarily rather than being delivered to a specific site. This is most pertinent with regard to albumin-bound drugs and toxin removal. The reduction in detoxification efficiency is especially noteworthy, indicating that the albumin in patients with cirrhosis is incapable of binding and removing waste products for metabolism or excretion effectively. There is Fig. 7. Difference in functional binding capacity determined by spin label binding studies at days 0 and 7 in groups treated either with MARS or standard medical therapy (SMT). (A) Calculated detoxification efficiency. (B) Real transport efficiency. (C) Measured binding capacity at BS1. (D) Calculated effective albumin concentration. No significant difference was found between treatment groups or between day 0 and 7 in either cohort. 562 JALAN ET AL. already evidence to suggest that the plasma antioxidant status of cirrhotic patients is reduced compared with healthy controls.9,23 Because albumin is the dominant plasma protein and is known to exhibit antioxidant properties, this lack of functional ability to both remove toxins and prevent oxidant stress damage suggests that further decompensation may occur more readily. It is interesting to note that the initial results from the IMA studies failed to show any differences between groups. However, once the IMA values were normalized to the plasma albumin concentration, a clear distinction between the patients with ACLF compared with those who did not have organ failure became apparent. In the currently licensed use of this assay, as a rule-out test for cardiac ischemia, most patients would be expected to have normal albumin levels. This is not true for patients with liver disease in whom a progressive decrease in albumin concentration is associated with reduced hepatic function, which may be reduced further with bleeding or sepsis.24 A reduced albumin level will immediately result in a lower capacity to bind cobalt, yielding an artificially high false positive IMA score; however, this provides no information to the degree of albumin damage or oxidative stress load. Hence, a normalbuminemic subject with significant albumin damage would have a similarly high IMA score compared with a hypoalbuminemic individual, even if the albumin present was functioning normally (e.g., following venesection). It is only by expressing the IMA per unit albumin that an understanding of the amount of albumin dysfunction can be determined. By normalizing the measured IMA score to the plasma albumin concentration in this way, a relative indicator of albumin damage, and hence the environment of oxidative stress, can be obtained. We would therefore suggest that IMA should be expressed relative to the albumin concentration (IMAR) to minimize the interference from reduced albumin level. Using this rationale, our studies revealed that IMAR levels predicted mortality of patients with acute decompensation of cirrhosis accurately with an AUROC of 0.8. Though it is likely that a patient with liver disease is likely to have reduced albumin levels, our study indicates that when this is coupled with ongoing albumin damage and expressed as a ratio, the prognostic indication is less favorable. This observation must be taken in light of the fact that it is a relatively small study and would require confirmation in larger studies. These observations do, however, indicate alternative mechanisms to explain the proven value of albumin infusion in patients with cirrhosis with spontaneous bacterial peritonitis6 and also where albumin formed part of a combination ther- HEPATOLOGY, August 2009 apy for hepatorenal syndrome.7 According to the classical hypothesis, the benefit of albumin in these situations is thought to be due to expansion of the circulating plasma volume, thereby ensuring adequate renal perfusion. The results of this study indicate that it is likely that additional benefit may have been conferred by the enhancement of the transport and detoxification function of albumin contributing to the improved outcome in these patients.1 Though the exact mechanism/stress mediator leading to the formation of IMA could be varied, in the laboratory the effect can be consistently repeated via exposure of albumin to hydroxyl radicals.18 The significance of this assay in determining periods of ischemia is evident in that it has recently been licensed by the U.S. Food and Drug Administration as a rule-out test for cardiac ischemia.25 Though the presence of IMA is not diagnostic of a cardiac infarct, as any regional ischemia has the potential to generate IMA, its absence indicates that it is most unlikely and patients with a low IMA score can be discharged. The loss of metal chelation function, as evidenced by increasing IMA, would contribute to an environment of continued oxidative stress. As proteins become damaged and release metal ions into the system, where they become redox active, they contribute to radical formation by Fenton chemistry processes.26,27 Albumin ordinarily provides a firstline defense against these reactions by binding and removing metal ions from the plasma, an ability that appears to be deficient in this patient cohort. Of further interest is the observed relationship between the calculated binding constant (KB) of binding sites 1 and 2 and the IMAR score. Previous research into the areas of albumin affected to result in increased IMA have focused on the metal binding region at the N terminus of the protein. However, a recent study28 has suggested that although cobalt may bind at this site transiently, its electronic configuration is better suited to binding at the fatty acid binding sites. We observed a significant relationship between the IMAR and the functionality of these sites, supporting the hypothesis that this is the binding location (Fig. 3). This finding suggests that IMAR may be a more useful indicator of albumin function than previously thought, providing insight into the normal functional capacity of this important, ubiquitous protein. MARS is an extracorporeal albumin dialysis device that has been shown to be of value as a detoxification tool with evidence that it can effectively remove protein-bound substances from the circulation and has been shown to be useful for the treatment of hepatic encephalopathy and in patients with severe cholestasis HEPATOLOGY, Vol. 50, No. 2, 2009 to possibly improve survival.4,10-12 Current hypotheses suggest that the removal of excess protein-bound toxins in the extracorporeal circuit is likely to regenerate the native albumin, thereby enhancing its functional capacity so that it may be able to transport and detoxify more toxins. Contrary to this existing hypothesis, albumin dialysis using MARS did not improve the measured functional capacity of the patient’s circulating albumin. This indicates that although MARS therapy is capable of removing albumin-bound materials (e.g., bilirubin) it remains unable to regenerate the functional characteristics of the native albumin. Similarly, no significant changes in IMAR levels were observed following MARS therapy (data not shown), indicating that the amount of functionally damaged albumin remained elevated after treatment. Furthermore, the observed improvement in the biochemistry values and the prognostic scores merely reflect removal of bilirubin and creatinine, and possibly other metabolic toxins, indicating that albumin dialysis in its current form can be used to treat the symptoms of the condition, but does not address the underlying functional impairment of the patients’ albumin. An explanation for the lack of improvement in the functional capacity of albumin may be that the disease process irreversibly damages the plasma albumin. The nature of such damage has yet to be defined, though interruption of the disulphide bridges within albumin would lead to a breakdown of the globular structure and may prevent binding site access. It should also be considered that the transport properties of the albumin used as dialysate in the MARS system may be significantly lower than in healthy subjects in vivo. In a separate study, it was found that the detoxification efficacy of commercial albumins is only 20% to 40% of the native protein.17 In conclusion, the results of this study clearly indicate that the functional ability of albumin in cirrhosis is severely compromised, which further worsens in liver failure. In addition to these functional disturbances, the albumin concentration was markedly reduced, which most likely further compounds the overall functional capacity of albumin. This loss of albumin function and an increase in IMAR levels, indicating protein modification, was associated with poor survival. Whether this loss of albumin function is merely a consequence of liver failure or is indeed of pathogenic significance needs to be answered in future studies. Though albumin dialysis has been shown to remove albumin-bound toxins, it does not restore the functional ability of the patient albumin. These findings should be considered in the development of new types of albumin dialysis systems and for the use of albumin JALAN ET AL. 563 for dialysis with improved transport and detoxification capacity. Furthermore, these findings argue for further studies of albumin biology in cirrhosis, giving consideration to the use of albumin infusion not for fluid replacement, but as an agent to increase detoxification capacity. References 1. Quinlan GJ, Martin GS, Evans TW. Albumin: biochemical properties and therapeutic potential. HEPATOLOGY 2005;41:1211-1219. 2. Human albumin administration in critically ill patients: systematic review of randomised controlled trials. Cochrane Injuries Group Albumin Reviewers. BMJ 1998;317:235-240. 3. Finfer S, Bellomo R, Boyce N, French J, Myburgh J, Norton R. A comparison of albumin and saline for fluid resuscitation in the intensive care unit. N Engl J Med 2004;350:2247-2256. 4. Stadlbauer V, Davies NA, Sen S, Jalan R. Artificial liver support systems in the management of complications of cirrhosis. Semin Liver Dis 2008;28: 96-109. 5. Schrier RW, Arroyo V, Bernardi M, Epstein M, Henriksen JH, Rodés J. Peripheral arterial vasodilation hypothesis: a proposal for the initiation of renal sodium and water retention in cirrhosis. HEPATOLOGY 1988;8:11511157. 6. Sort P, Navasa M, Arroyo V, Aldeguer X, Planas R, Ruiz-del-Arbol L, et al. Effect of intravenous albumin on renal impairment and mortality in patients with cirrhosis and spontaneous bacterial peritonitis. N Engl J Med 1999;341:403-409. 7. Ortega R, Ginès P, Uriz J, Cárdenas A, Calahorra B, De Las Heras D, et al. Terlipressin therapy with and without albumin for patients with hepatorenal syndrome: results of a prospective, nonrandomized study. HEPATOLOGY 2002;36:941-948. 8. Ginsberg MD, Hill MD, Palesch YY, Ryckborst KJ, Tamariz D. The ALIAS Pilot Trial: a dose-escalation and safety study of albumin therapy for acute ischemic stroke—I: physiological responses and safety results. Stroke 2006;37:2100-2106. 9. Oettl K, Stadlbauer V, Petter F, Greilberger J, Putz-Bankuti C, Hallstrom S, et al. Oxidative damage of albumin in advanced liver disease. Biochim Biophys Acta 2008;1782:469-473. 10. Heemann U, Treichel U, Loock J, Philipp T, Gerken G, Malago M, et al. Albumin dialysis in cirrhosis with superimposed acute liver injury: a prospective, controlled study. HEPATOLOGY 2002;36:949-958. 11. Sen S, Davies NA, Mookerjee RP, Cheshire LM, Hodges SJ, Williams R, et al. Pathophysiological effects of albumin dialysis in acute-on-chronic liver failure: a randomized controlled study. Liver Transpl 2004;10:11091119. 12. Hassanein TI, Tofteng F, Brown RS Jr, McGuire B, Lynch P, Mehta R, et al. Randomized controlled study of extracorporeal albumin dialysis for hepatic encephalopathy in advanced cirrhosis. HEPATOLOGY 2007;46: 1853-1862. 13. Bhagavan NV, Lai EM, Rios PA, Yang J, Ortega-Lopez AM, Shinoda H, et al. Evaluation of human serum albumin cobalt binding assay for the assessment of myocardial ischemia and myocardial infarction. Clin Chem 2003; 49:581-585. 14. Kamath PS, Wiesner RH, Malinchoc M, Kremers W, Therneau TM, Kosberg CL, et al. A model to predict survival in patients with end-stage liver disease. HEPATOLOGY 2001;33:464-470. 15. Pugh RN, Murray-Lyon IM, Dawson JL, Pietroni MC, Williams R. Transection of the oesophagus for bleeding oesophageal varices. Br J Surg 1973; 60:646-649. 16. Kazmierczak SC, Gurachevsky A, Matthes G, Muravsky V. Electron spin resonance spectroscopy of serum albumin: a novel new test for cancer diagnosis and monitoring. Clin Chem 2006;52:2129-2134. 17. Matthes G, Seibt G, Muravsky V, Hersmann G, Dornheim G. Albumin transport analysis of different collected and processed plasma products by 564 18. 19. 20. 21. 22. JALAN ET AL. electron spin resonance spectroscopy. Transfus Apher Sci 2002;27:129135. Roy D, Quiles J, Gaze DC, Collinson P, Kaski JC, Baxter GF. Role of reactive oxygen species on the formation of the novel diagnostic marker ischaemia modified albumin. Heart 2006;92:113-114. Lapenna D, Ciofani G, Pierdomenico SD, Giamberardino MA, Cuccurullo F. Reaction conditions affecting the relationship between thiobarbituric acid reactivity and lipid peroxides in human plasma. Free Radic Biol Med 2001;31:331-335. Sen S, Rose C, Ytrebø LM, Davies NA, Nedredal GI, Drevland SS, et al. Effect of albumin dialysis on intracranial pressure increase in pigs with acute liver failure: a randomized study. Crit Care Med 2006;34:158-164. Gianazza E, Crawford J, Miller I. Detecting oxidative post-translational modifications in proteins. Amino Acids 2007;33:51-56. Mantena SK, King AL, Andringa KK, Landar A, Darley-Usmar V, Bailey SM. Novel interactions of mitochondria and reactive oxygen/nitrogen species in alcohol mediated liver disease. World J Gastroenterol 2007;13:4967-4973. HEPATOLOGY, August 2009 23. Moore K. Isoprostanes and the liver. Chem Phys Lipids 2004;128:125133. 24. Margarson MP, Soni NC. Changes in serum albumin concentration and volume expanding effects following a bolus of albumin 20% in septic patients. Br J Anaesth 2004;92:821-826. 25. Apple FS, Wu AH, Mair J, Ravkilde J, Panteghini M, Tate J, et al. Future biomarkers for detection of ischemia and risk stratification in acute coronary syndrome. Clin Chem 2005;51:810-824. 26. Stadtman ER. Oxidation of free amino acids and amino acid residues in proteins by radiolysis and by metal-catalyzed reactions. Annu Rev Biochem 1993;62:797-821. 27. Stadtman ER, Oliver CN, Starke-Reed PE, Rhee SG. Age-related oxidation reaction in proteins. Toxicol Ind Health 1993;9:187-196. 28. Mothes E, Faller P. Evidence that the principal CoII-binding site in human serum albumin is not at the N-terminus: implication on the albumin cobalt binding test for detecting myocardial ischemia. Biochemistry 2007;46: 2267-2274.