Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
191
REVIEW ARTICLE
Use of Dapsone in the Prevention and Treatment of Pneumocystis carinii
Pneumonia: A Review
Walter T. Hughes
From the Department of Infectious Diseases, St. Jude Children’s
Research Hospital, Memphis, Tennessee
Since 1984, when dapsone was first found to have activity
against Pneumocystis carinii [1], ú200 publications have addressed the use of this drug in the prevention and treatment of
P. carinii pneumonia (PCP). Reports have been limited almost
exclusively to clinical studies of patients with HIV infection
and to experimental studies of the corticosteroid-treated rat
model. These investigations have been adequate to give a reasonable perspective on the use of dapsone in the management
of PCP, especially for prophylaxis. The purpose of this article
is to review all publications, as well as studies presented at
national and international meetings, and to provide pertinent
information on the use of this drug for PCP in the immunocompromised host.
Antimicrobial Activities of Dapsone
Dapsone-USP, 4-4*-diaminodiphenylsulfone, is a synthetic sulfone with bactericidal and bacteriostatic activity against Mycobacterium leprae and is effective in the treatment of patients with
leprosy. It is also active in high concentrations (§10 mg/mL)
against Mycobacterium tuberculosis and several other species
Received 31 October 1997; revised 20 February 1998.
Financial support: National Cancer Institute (P01 CA-20180 and P30 CA21765), National Institutes of Allergy and Infectious Diseases (Pediatric ACTG,
U01 AI32908), and the American Lebanese Syrian Associated Charities.
Reprints or correspondence: Dr. Walter T. Hughes, 332 North Lauderdale,
Memphis, Tennessee 38105.
Clinical Infectious Diseases 1998;27:191–204
q 1998 by the Infectious Diseases Society of America. All rights reserved.
1058–4838/98/2701–0035$03.00
/ 9c51$$jy36
06-16-98 00:27:17
of mycobacteria, including Mycobacterium avium complex. In
combination with pyrimethamine, dapsone has been used successfully as chemoprophylaxis for malaria due to chloroquineresistant Plasmodium falciparum and Plasmodium vivax.
With or without trimethoprim (TMP) or pyrimethamine, dapsone has been shown in animal and human studies to effectively
prevent and treat PCP. Some evidence suggests it has activity
against Toxoplasma gondii.
Mechanisms of Action
Dapsone was first synthesized from para-chloronitrobenzene
in 1945 [2] and first marketed in the United States in 1957.
The drug is an analog of para-Aminobenzoic acid and acts
through the inhibition of folic acid synthesis in susceptible
organisms. It is an inhibitor of the dihydropteroate synthetase
of P. carinii. Voeller et al. [3] found that a 1.5-mM concentration of dapsone inhibited 50% of P. carinii dihydropteroate
synthetase activity. In another study, 0.4 mM of dapsone was
effective when tested in an in vitro culture [4].
Dapsone may conceivably affect P. carinii infection by
mechanisms other than intervention with folic acid synthesis.
In vitro studies have shown that dapsone stimulates neutrophil
motility. In a clinical study of healthy individuals [5], dapsone
mediated stimulation of polymorphonuclear leukocyte migration. This was related to inhibition of the peroxidase-H2O2halide system in vitro. Other studies indicate that dapsone may
inhibit the alternate pathway of complement activation and
interfere with the myeloperoxidase-H2O2-halide-mediated cytotoxic system within neutrophils. A recent study of AIDS
cida
UC: CID
Downloaded from http://cid.oxfordjournals.org/ by guest on September 9, 2014
Dapsone, with or without trimethoprim or pyrimethamine, has strong anti-Pneumocystis carinii
activity, as demonstrated by in vitro methods, animal studies, and clinical trials. The drug blocks
folic acid synthesis of P. carinii by inhibition of dihydropteroate synthetase activity. Dapsone is
efficiently absorbed (70% – 80%) from the gastrointestinal tract, reaches peak serum concentration
in 2 – 6 hours, and is adequately distributed to the fluid of the alveolar spaces. Synergistic effects
against P. carinii are noted when trimethoprim is combined with dapsone. This combination is
recommended for therapeutic use for P. carinii pneumonia (PCP) as an alternative for patients who
cannot take trimethoprim-sulfamethoxazole (TMP-SMZ). Evidence from more than 40 studies of
dapsone as prophylaxis for PCP in AIDS patients shows that dapsone, either alone or in combination
with pyrimethamine, is as effective as aerosolized pentamidine or atovaquone but slightly less
effective than TMP-SMZ. Adverse effects include rash, anemia, methemoglobinemia, agranulocytosis, and hepatic dysfunction. Desensitization can be accomplished with many cases. Dapsone is the
most cost-effective prophylaxis currently available for PCP.
192
Hughes
Metabolism and Pharmacokinetics
At least two major metabolites come from biotransformation
of dapsone: monoacetyl dapsone (MADDS) and dapsone hydroxylamine. Neither contributes to the therapeutic affect of
the drug. Dapsone is acetylated to MADDS by N-acetyltransferase in the liver. MADDS may also be acetylated to dapsone,
and an equilibrium may be reached within a few hours after
administration. There are no significant differences between
slow and fast acetylators in the frequency and type of side
effects, plasma concentrations, and therapeutic efficacy in nonPCP conditions. The second major metabolite is N-hydroxylated to dapsone hydroxylamine in the liver by the mixed oxidase system in the presence of oxygen and NADPH. This
metabolite has been associated with hematologic toxicity.
/ 9c51$$jy36
06-16-98 00:27:17
Dapsone is available in 25-mg and 100-mg tablets. No intravenous formulation has been developed for commercial use.
In healthy adults dapsone is slowly but efficiently absorbed
from the gastrointestinal tract, with 70% – 80% bioavailability
in an acidic environment. Peak serum concentrations of 1.7
mg/mL to 1.9 mg/mL are achieved in 2 – 6 hours after a dose
of 100 mg. The drug is well distributed throughout total-body
water and all tissues. The plasma half-life may vary from 10
to 50 hours, with a mean time of 30 hours, for both dapsone
and MADDS. About 70% – 85% of the drug is excreted in the
urine. Enterohepatic circulation following biliary excretion of
free drug also occurs, accounting for prolonged persistence in
the plasma after drug administration is stopped [10].
In children with HIV infection, pharmacokinetic studies
show that clearance (CL) and Vss (apparent volume of distribution of steady state) of dapsone are approximately twofold
greater than in adults, while the t12 is comparable [11]. The
dose of 2.0 mg/kg (not to exceed a total dose of 100 mg/d)
administered at the same frequency used in adults may be used
for prophylaxis for and treatment of PCP.
Dapsone is readily soluble at normal acidic gastric pH and
remains insoluble at neutral pH. Because some drugs given
concomitantly with dapsone are absorbed best at alkaline pH,
such as didanosine, concern has been expressed about the effect
of alkalinization on the efficacy of dapsone [12]. In a prospective study in which volunteers were given 100 mg of dapsone
plus Maalox C (Novartis Consumer Health, Summit, NJ), the
antacid was found to facilitate rather than impair absorption of
dapsone [13]. At present there are no sound data to suggest
that clinicians need to modify the gastric acidity of patients
during the use of dapsone.
HIV-infected patients rarely receive dapsone without concomitant medications. The pharmacokinetic interactions of zidovudine, TMP, and dapsone in HIV-infected patients have
been studied [14]. Zidovudine did not influence the pharmacokinetic profile of dapsone, and dapsone had no effect on the
pharmacokinetic disposition of zidovudine. However, TMP decreased the renal clearance of zidovudine by 58%. There was
also a concurrent 54% decrease in urinary recovery of zidovudine. The mean area under the concentration curve from zero
to 6 hours of the zidovudine-glucuronide/zidovudine ratio was
unchanged. The data indicate that zidovudine, TMP, and dapsone can be given concomitantly to AIDS patients without
clinically significant interactions. However, with impaired liver
function and impaired glucuronidation, the doses of zidovudine
may need to be decreased.
In Malaysian leprosy patients, rifampin was found to decrease the plasma t12 of dapsone by 22% – 83%, probably by
enhancing hepatic clearance by induction of microsomal enzymes [15]. Because plasma concentrations of dapsone are
0.1 – 7.0 mg/mL with a dose of 200 mg and the MIC (in cell
culture) is 0.1 – 10 mg/mL, the concomitant use of rifampin and
dapsone could compromise the efficacy of the latter drug [16].
Population pharmacokinetics of dapsone were examined in
cida
UC: CID
Downloaded from http://cid.oxfordjournals.org/ by guest on September 9, 2014
patients with and without PCP [6] compared the ability of their
neutrophils to activate the respiratory burst. When stimulated
with P. carinii, neutrophils from the patients with a history of
PCP had a significantly lower response than those from the
other groups studied.
The in vitro experiments of Bozeman et al. [7] suggest that
dapsone could prevent myeloperoxidase- and eosinophil peroxidase – mediated tissue injury at sites where the peroxidase enzymes are secreted and diluted into the neutral pH environment
of the tissue interstitial space. However, dapsone did not inhibit
peroxidase-mediated antimicrobial activity, occurring at high
enzyme concentrations in the acid environment of the phagolysosomes. Whether or not dapsone affects neutrophil motility
and function to the extent that a discernible therapeutic impact
occurs is not known.
Some in vitro studies suggest dapsone might have some effect
on HIV replication [8]. In phytohemagglutinin P–activated HIV1-infected peripheral blood mononuclear cells, dapsone (2–10
ng/mL) decreased cell proliferation and HIV-1 replication. However, dapsone increased HIV-1 replication in peripheral blood
lymphocytes and monocyte-derived macrophages. Dapsone metabolites are potent oxidants that induce glutathione consumption
to counteract oxidative processes. It can be speculated that peripheral blood lymphocytes and monocyte-derived macrophages may
be able to generate N-hydroxyl-dapsone metabolically upon exposure to dapsone. This may, in turn, induce a glutathione deficit
in these cells and an oxidative exhaustion that leads to IL-2dependent proliferation of lymphocytes or enhancement of HIV
replication, or both. Duval et al. [8] found these activating effects
at concentrations from 1 ng/mL to 10 ng/mL. Dapsone serum
concentrations in HIV-infected patients given the drug range from
1.5 ng/mL to 4.2 ng/mL [9].
As with many drugs, the activity of dapsone may not be
limited to its effect on a single target in cell replication. Its
effect on the dihyhdropteroate synthetase of P. carinii is established. It seems reasonable to expect the anti-inflammatory
activity demonstrated in cases of leprosy, dermatitis herpetiformis, and other conditions would also occur in cases of PCP.
CID 1998;27 (July)
CID 1998;27 (July)
Dapsone and P. carinii Pneumonia
/ 9c51$$jy36
06-16-98 00:27:17
for once-a-week dosing of dapsone for PCP prophylaxis. Unfortunately, no studies of dapsone combined with TMP in
weekly doses have been performed.
Experimental Studies in Animals
Because of the remarkably high incidence of naturally acquired P. carinii infection in rats, the administration of corticosteroid immunosuppression for 4 – 6 weeks or longer results in
the provocation of extensive P. carinii pneumonitis from the
latent infection in 70% – 100% of animals. This experimental
animal model has been used to screen and identify drugs for
anti – P. carinii activity [21, 22]. Almost without exception,
drugs found effective in rat studies have been effective in
humans with PCP.
In 1984, Hughes and Smith [1] screened several drugs and
found that a 25-mg/(kgrd) dosage of dapsone was totally effective in preventing P. carinii infection. Dapsone was then evaluated at dosages of 5, 25, and 125 mg/(kgrd) and compared
with TMP-SMZ given at 50/250 mg/(kgrd) orally. The two
highest dosages of dapsone and TMP-SMZ prevented the infection in 100% of animals, and the lowest dosage of dapsone
(5.0 mg/[kgrd]) prevented it in 40% of all rats. All of the
untreated control animals developed PCP. Therapeutic efficacy
was determined by allowing animals to develop extensive PCP
and then initiating drug therapy. Based on the extent of residual
pneumonitis at the completion of treatment, the frequency of
PCP was reduced to 50% by TMP-SMZ and to 25% by dapsone, while all of the untreated controls had extensive PCP.
In later studies [23] the efficacies of TMP-SMZ, TMP/dapsone, dapsone, and pentamidine were compared for the prevention of PCP in the corticosteroid-treated rat model. While 11
(73%) of 15 untreated control animals had PCP after 10 weeks
of immunosuppression, none of the animals given 125 mg of
dapsone per kg daily, weekly, biweekly, or monthly had evidence of infection. Of the 10 rats given a single dose of dapsone
23 and 50 days after immunosuppression was started, five
(50%) developed P. carinii pneumonia. When three drugs were
given separately to groups of 10 rats in single doses every
other week, PCP occurred in 40% of those treated with TMPSMZ, in none of those treated with TMP/dapsone, and in all
of those given pentamidine.
The experiments showed that dapsone is highly effective in
chemoprophylaxis for PCP when given at monthly intervals or
more frequently and that dapsone and TMP/dapsone are more
effective than TMP-SMZ when given at biweekly intervals. It
seems reasonable to expect that at least weekly or even biweekly doses of dapsone or TMP/dapsone would provide an
effective and reasonably safe chemoprophylaxis regimen for
patients at high risk for PCP.
Separate studies of dapsone in the rat model [24, 25] and in
a mouse model of severe combined immunodeficiency [26]
have also shown dapsone to have potent anti – P. carinii activity. Walzer et al. [27] found dapsone alone to be effective in
cida
UC: CID
Downloaded from http://cid.oxfordjournals.org/ by guest on September 9, 2014
HIV-infected patients receiving 100 mg of dapsone twice
weekly. Rifampin was found to increase the values of clearance/bioavailability (CL/F) and volume of clearance/bioavailability (V/F) by Ç70% (CL/F and V/F were 1.83 L/h and
69.6 L, respectively, in those not taking rifampin) [17].
In AIDS patients successfully treated for PCP, the mean
peak dapsone level of 2.1 mg/mL was achieved 6 hours after
administration of TMP/dapsone [18]. Dapsone and TMP
plasma concentrations were both higher when the drugs were
given concomitantly than when given separately. Plasma concentrations of dapsone were 40% higher in patients treated
with TMP/dapsone than in those treated with the same dose of
dapsone alone (2.1 mg/mL vs. 1.5 mg/mL). The concentration
of TMP was 45% higher in patients treated with TMP/dapsone
than in those treated with TMP-sulfamethoxazole (SMZ) (18.8
mg/mL vs. 12.4 mg/mL).
In a subsequent study the same authors were not able to
demonstrate increased concentrations when these drugs were
given concomitantly [14]. However, the former study evaluated
a larger group of patients receiving treatment for PCP, while
the latter study involved only six asymptomatic patients. Until
more definitive data are available, the extent of drug interaction
is unclear. One can conclude at least that no antagonistic effects
are at play.
Because infection with P. carinii and the disease it causes
are located almost exclusively in the lung, it is critical that
drug activity and concentration be maximal in the lung parenchyma and alveolar space. Cruciani et al. [19] studied the penetration of dapsone into epithelial lining fluid of HIV-infected
patients receiving prophylaxis with dapsone (100 mg twice
weekly). The bronchoalveolar lavage (BAL) fluid and plasma
samples were studied for dapsone concentrations. The mean
concentrations in BAL fluid at 2, 4, 12, 24, and 48 hours after
the dose of 100 mg were 0.9, 0.7, 1.55, 0.23, and 0.45 mg/L,
respectively. These concentrations were 76%, 79%, 115%,
65%, and 291% respectively, of those observed in plasma at
the same times. This study suggests that dapsone is well distributed into the epithelial lining fluid and that administration of
100 mg of dapsone twice a week provides sustained concentrations in the tissue compartment.
The pharmacokinetics and safety of weekly dapsone and
dapsone plus pyrimethamine in adults with AIDS were studied
[20]. Of three doses — 100 mg, 200 mg, and 300 mg of dapsone
weekly — 200 mg weekly was established as the maximum
tolerated dose. This dose was then found to be well tolerated
in combination with pyrimethamine (25 mg).
In another study [9], median plasma concentrations of dapsone and pyrimethamine during day 1 after ingestion of
200 mg of dapsone and 75 mg of pyrimethamine were 1.04
mg of dapsone and 0.36 mg of pyrimethamine per mL. By day
6 – 7 the dapsone concentration decreased to õ20 ng/mL, but
the pyrimethamine level remained elevated at 0.13 mg/mL.
Concurrent administration of didanosine did not decrease the
drug concentrations. These data tend to support the potential
193
194
Hughes
murine PCP and that Ro 11-8958, an analog of TMP, enhanced
the efficacy of dapsone. In an animal model with dual infections
of PCP and toxoplasmosis, Brun-Pascaud et al. [28] found the
drug combination of pyrimethamine (3 mg/kg) plus dapsone
(25 mg/kg or 50 mg/kg) administered daily totally prevented
both infections. In another study, a diformyl derivative of dapsone, 4-4*-sulfonylbisformanilide, was found to have efficacy
equal to that of dapsone [29]. This compound has not been
evaluated in clinical trials for PCP.
Clinical Trials: Treatment
/ 9c51$$jy36
06-16-98 00:27:17
Although the numbers of patients studied were small, the
100% successful response rate with dapsone/TMP suggested
the combination was more efficacious than dapsone alone (61%
successful response rate). Furthermore, it is noteworthy that
major toxicity was noted in none of the patients treated with
dapsone alone, in 13% of those treated with dapsone/TMP, and
in 51% of recipients in the comparable study with TMP-SMZ.
Whether or not TMP plays a role in the toxicity profile is not
known. Such a role might come from a direct adverse effect
of TMP or might be due to an associated increase in the plasma
concentration of dapsone, as shown in one of the studies by
Lee et al. [14] and discussed herein in the section on metabolism and pharmacokinetics.
In a small randomized (2:1) double-blind study [32], 18
HIV-infected patients with moderate or severe PCP (D[A-a]
O2 of 35 – 55 mm Hg) received either trimetrexate, leucovorin,
and dapsone or TMP-SMZ. Ten (77%) of the 13 patients given
trimetrexate/leucovorin/dapsone and 3 (60%) of the 5 treated
with TMP-SMZ had responded favorably by day 21 of treatment. Adverse reactions occurred in 85% and 80% of the patients, respectively.
In 1991 Safrin et al. [33] concluded that a high-dose, singleagent regimen of dapsone was not suitable for further study or
as therapy for PCP and that this therapy should not be clinically
employed. Their study was a prospective one of seven patients
with mild PCP. Patients were treated with 200 mg of dapsone
daily. None of the seven patients successfully completed a full
course of treatment with dapsone; two patients died, and four
experienced major side effects. There was no explanation for
these poor responses in comparison with those in other studies.
In 1996 a randomized, double-blind study (ACTG [AIDS
Clinical Trials Group] 108) was reported by Safrin et al. [34]
that involved 181 AIDS patients with cytologically documented
PCP, who were randomized to receive treatment with one of
three drug regimens: dapsone plus TMP, TMP-SMZ, or clindamycin plus primaquine. Dapsone was used at a dosage of 100
mg/d. Treatment was given over a period of 21 days.
The results showed no significant differences among the
groups with respect to therapeutic failure (P ú .2), survival
during therapy or for 2 months thereafter (P ú .2), and treatmentlimiting toxicity (P Å .2) (figures 1 and 2). However, elevation
of serum aminotransferase levels to more than five times the
baseline levels was more frequent in the TMP-SMZ group
(P Å .003), and one or more serious hematologic toxic effects
(neutropenia, anemia, thrombocytopenia, or methemoglobinemia) occurred more frequently in the clindamycin/primaquine
group (P Å .01). Of the 8 deaths (4.4%) during the 81-day period
of observation, 4 were in the TMP-SMZ group, 2 in the dapsone/
TMP group, and 2 in the clindamycin/primaquine group. While
this is the largest trial evaluating the therapeutic efficacy of dapsone, the limited sample size prevented unequivocal demonstration of the equality of these three regimens.
Several single case reports describe the successful treatment
of PCP with dapsone, with and without TMP [35 – 38]. At
cida
UC: CID
Downloaded from http://cid.oxfordjournals.org/ by guest on September 9, 2014
The first clinical trials to evaluate dapsone in humans with
PCP were done in 1984 and 1985. The plan was to first evaluate
dapsone plus TMP in an open-label study for efficacy in the
treatment of PCP. If this was successful a second study would
be undertaken with dapsone alone. This approach stemmed
from the animal studies showing the combination of dapsone/
TMP to be more effective than dapsone alone [21].
The initial study by Leoung et al. [30] included adult patients
with AIDS and first-episode PCP at the San Francisco General
Hospital between November 1984 and April 1985. Dapsone
(100 mg/d) and TMP (20 mg/[kgrd]) were given orally. Fifteen
patients were studied. The pretreatment arterial oxygen tension
ranged from 48 to 82 torr (median, 68.1 torr) in 14 of the
patients, and one patient’s value was 104 torr. The conditions
of all 15 patients improved clinically and radiographically
within 3 – 10 days after the start of dapsone/TMP therapy. Continued improvement was noted at the end of 3 weeks of treatment.
Fourteen of the patients had adverse reactions (nausea and
vomiting in 6, maculopapular rash in 8, decrease in hematocrit
(ú5%) in 7, neutropenia in 1, and thrombocytopenia in 1).
Two patients had to be withdrawn from the therapy because
of rash. Six patients had an increase in hepatic transaminase
levels. The observed 100% initial response rate (95% CI, 78% –
100%) and 87% overall efficacy (95% CI, 58% – 98%) were
equal to or better than the values noted in a comparable study
with TMP-SMZ and pentamidine.
Because of the success of the initial study with use of both
dapsone and TMP, the second planned study was undertaken
to evaluate dapsone alone [31]. As shown in animal studies,
the single-drug therapy was effective but not as effective as
the combination. The 18 patients with AIDS and PCP admitted
to San Francisco General Hospital between April 1985 and
July 1985 were given dapsone (100 mg/d) orally for 21 days.
The conditions of 7 (39%) of the 18 patients worsened during
dapsone therapy, and these cases were considered treatment
failures; the conditions of the remaining 11 (61%) improved
within 3 – 10 days after administration of dapsone was started.
Adverse reactions were noted in 6 of the 11 patients whose
dapsone therapy was maintained (rash in 6 patients and abnormal liver enzyme levels in 2). However, no toxic effect necessitating termination of treatment occurred.
CID 1998;27 (July)
CID 1998;27 (July)
Dapsone and P. carinii Pneumonia
present one may conclude that dapsone, with or without TMP,
is effective in the treatment of PCP, but the drug combination
is most effective. TMP/dapsone is probably similar in efficacy
to TMP-SMZ for mild and moderately severe PCP. Dapsone
alone is not indicated for treatment. Some but not all patients
who have experienced adverse reactions to TMP-SMZ will be
able to tolerate TMP/dapsone.
once a day orally; (2) dapsone, 50 mg daily, plus pyrimethamine, 50 mg once a week, and leucovorin, 25 mg once a week
orally; or (3) dapsone, 200 mg, plus pyrimethamine, 75 mg,
and leucovorin, 25 mg once a week orally. The dapsone
dose recommended as PCP prophylaxis for children is 2.0
mg/(kgrd), not to exceed 100 mg daily.
In the early years of the AIDS epidemic, before PCP prophylaxis became established as standard practice, PCP occurred in
80% of persons with AIDS and was the AIDS-defining illness
in ú60% of patients [83]. Effective chemoprophylaxis and
more effective primary treatment for HIV infection have
brought about an impressive reduction in PCP among patients
with HIV infection.
Unfortunately, despite these effective prophylactic regimens,
PCP continues to be a significant opportunistic infection in
AIDS. A longitudinal cohort study in the Multicenter AIDS
Cohort Project, reported in 1995 [84], identified factors associated with failure of PCP prophylaxis in patients prescribed
TMP-SMZ, dapsone, or aerosolized pentamidine. The main
predictor of failure of prophylaxis was profound lymphopenia
affecting CD4/ lymphocyte counts. Of the 476 patients receiving prophylaxis, 92 (19%) had breakthrough PCP. PCP occurred more rapidly among patients receiving aerosolized pentamidine (14.5% of patients per year) and dapsone (13.5% per
year) than among those given TMP-SMZ (9.8% per year) as
the initial regimen.
Although more than 40 studies involved the use of dapsone
as prophylaxis for PCP, these investigations have varied greatly
Clinical Trials: Prophylaxis
The greatest use of dapsone in the management of PCP has
been as prophylaxis for patients at high risk for this infection.
The efficacy demonstrated in animal studies has also been demonstrated in at least 41 clinical trials involving HIV-infected individuals (table 1). Two major advantages of dapsone are its long halflife, allowing infrequent dosing, and low cost. Some evidence
suggests dapsone in combination with pyrimethamine may prevent mycobacterial infections [81] and toxoplasmosis [62].
Efficacy with regard to the successful prevention of PCP has
been demonstrated in clinical trials of four drugs: TMP-SMZ,
dapsone, aerosolized pentamidine, and atovaquone. TMP-SMZ
is considered the first choice for those who can tolerate the
drug. Dapsone was recommended in the ‘‘1997 USPHS/IDSA
Guidelines for the Prevention of Opportunistic Infections in
Persons Infected with Human Immunodeficiency Virus’’ [82]
for those who are unable to take TMP-SMZ. The dosage
schemes suggested are: (1) dapsone, 50 mg b.i.d. or 100 mg
/ 9c51$$jy36
06-16-98 00:27:17
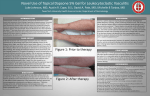
Figure 2. Time until dose-limiting toxicity, according to treatment
regimen for Pneumocystis carinii pneumonia. Logrank test, P ú .2.
TS Å trimethoprim-sulfamethoxazole; DT Å dapsone/trimethoprim;
CP Å clindamycin/primaquine. Figure reprinted from [34] with permission.
cida
UC: CID
Downloaded from http://cid.oxfordjournals.org/ by guest on September 9, 2014
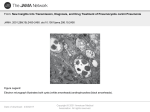
Figure 1. Time until therapeutic failure, according to treatment
regimen for Pneumocystis carinii pneumonia. Logrank test,
P ú .2. TS Å trimethoprim-sulfamethoxazole; DT Å dapsone/trimethoprim; CP Å clindamycin/primaquine. Figure reprinted from
[34] with permission.
195
196
Hughes
CID 1998;27 (July)
Table 1. Data from dapsone prophylaxis studies described in the literature.
Percentage of patients with
Prophylaxis
Reference, year,
type of study
[39], 1984, PO
[40], 1989, CR
[41], 1989, PO
[42], 1990, PO
[43], 1990, RO
[45], 1991, RO
[46], 1991, O
[47], 1991, RO
[48], 1991, PO
[49], 1991, O
[50], 1991, PO
[51], 1991, RO
[52], 1992, RO
[53], 1992, CR
[54], 1992, RO
[55], 1992, PO
[56], 1992, RO
[57], 1992, PO
[58], 1993, RO
[59], 1993, CR
[60], 1993, RO
[61], 1993, RO
[62], 1993, RO
Dapsone
TMP-SMZ
None
Dapsone
None
Dapsone
Dapsone
Dapsone
Dapsone
Dapsone
Dapsone
Dapsone /
Pyrimethamine
Dapsone
Expected
Dapsone
Pentamidine (a)
Dapsone
Dapsone
Dapsone /
Pyrimethamine
Dapsone
Dapsone /
Pyrimethamine
Dapsone
None
Dapsone
Fansidar
Dapsone
Pentamidine (a)
Dapsone
TMP-SMZ
Pentamidine (a)
Dapsone
Prior TMP-SMZ:
With AEs
Without AEs
Dapsone /
Pyrimethamine
TMP-SMZ
Dapsone
TMP-SMZ
Dapsone /
Pyrimethamine
Pentamidine
Dapsone /
Pyrimethamine
TMP-SMZ
Dapsone
Dapsone /
Pyrimethamine
Pentamidine (a)
TMP/SMZ
Dapsone
Pentamidine (a)
Dapsone /
Pyrimethamine
Pentamidine
/ 9c51$$jy36
Dosage*
No. of
patients
100 mg/d
Daily
...
100 mg/w
...
50 – 100 mg/d
50 mg/d
100 mg/d
100 mg/w
200 mg/w
300 mg/w
200 mg/w
25 mg/w
100 – 300 mg/w
(Calculated)
100 mg 2 1 w
400 mg/m
100 mg 2 1 w
200 mg/w
200 mg/w
25 mg/w
100 mg 2 1 w
100 mg 2 1 w
25 mg 2 1 w
50 mg 2 1 w
...
50 mg/d
500 mg 1 1 w
100 mg 2 1 w
400 mg/mo
50 mg/d
31w
300 mg/mo
100 mg 3 1 w
100 mg 3 1 w
25 mg 3 1 w
312
100 mg/d
Daily
100 mg/w
25 mg/w
300 mg/mo
100 mg/w
25 mg/w
31w
100 mg 3 1 w
100 mg/w
25 mg/w
300 mg/mo
31w
100 mg 2 1 w
100 mg q2w
50 mg/d
50 mg/w
300 mg/mo
06-16-98 00:27:17
cida
Time observed
Break-through
PCP
AEs
173
48
23
16
46
24
20
10
5
7
9
5
9.4 mo
8.2 mo
9.6 mo
ND
190 d
108 d
19 w
19 w
ND
ND
ND
ND
1
0
100
6.3
34.8
4
ND
ND
4
0
0
0
10
38
...
ND
...
20
7
ND
ND
23
ND
ND
61
...
50
46
22
23
22
9 mo
...
11.3 mo
Same
34 w
40 w
37 w
2
23
16
15.2
4.5
4.3
4.5
13
...
16
4
18
13
18
2.3
1.8
3.1
2.7
10
80
0
2
18
17
6.5
0
3.6
0
0
...
10
10.8
12
17
55
55
2
33
128
109
12 – 18 mo
16 mo
10
10
65
51
50
46
77
133
125
79
12 mo
6 mo
6 mo
6 mo
18 mo
18 mo
5.7 mo
7.4 mo
9.3 mo
23 w
54
25
142
16
ND
12
ND
84
47
39
58
ND
862 pm
776 pm
21 mo
2
2
2
12
ND
70
64
ND
29
85
10 mo
380 d
2
15.3
ND
42
81
23
116
380 d
126 pm
304 d
3.7
14
6.9
67
39
7.8
108
107
126
152
173
299
339
42
43
539
4.6
2.8
18
14
5.8
1.09
9.0
10.7
2.0
24.3
176
Same
5.7
1.7
UC: CID
d
d
w
w
d
Downloaded from http://cid.oxfordjournals.org/ by guest on September 9, 2014
[44], 1990, PO
Drug
CID 1998;27 (July)
Dapsone and P. carinii Pneumonia
197
Table 1. (Continued )
Percentage of patients
with
Prophylaxis
Reference, year,
type of study
[63], 1993, CR (children)
[64], 1993, PR
[65], 1993, CR
[66], 1994, RO
[69], 1995, RO
[70], 1995, RO
[71], 1995, RO
[72], 1995, RO
[73], 1995, CR
[74], 1995, RO
[75], 1995, RO
[76], 1996, CR
[77], 1996, CR
[78], 1996, RO
[79], 1997, RO
[80], 1997, O
Dosage*
Dapsone
Dapsone /
Pyrimethamine
Fansidar
Dapsone /
Pyrimethamine
Pentamidine
Dapsone /
Pyrimethamine
TMP-SMZ
Pentamidine (a)/
Pyrimethamine
Sulphamethopyrazine/
Pyrimethamine
Dapsone
Dapsone
TMP-SMZ
Pentamidine (a)
Pentamidine iv
Dapsone
Pentamidine (a)
Dapsone /
Pyrimethamine
TMP-SMZ
Pentamidine (a)
Dapsone /
Pyrimethamine
TMP-SMZ
Dapsone /
Pyrimethamine
Pentamidine (a)
Dapsone
TMP-SMZ
Pentamidine
Dapsone
TMP-SMZ
Pentamidine
Dapsone /
Pyrimethamine
TMP-SMZ
Dapsone
TMP-SMZ
Clindamycin / primaquine
Dapsone
TMP-SMZ
Pentamidine
Dapsone /
Pyrimethamine
TMP-SMZ
Dapsone
Atovaquone
Dapsone
1 mg/(kgrd)
100 mg 2 1 w
25 mg 2 1 w
ND
100 mg/w
12.5 mg q4d
300 mg/mo
100 mg/w
25 mg/w
31w
300 mg/mo
25 mg daily
500 mg 2 1 w
25 mg 2 1 w
100 – 350 mg/w
1 mg/(kgrd)
31w
300 mg/mo
4 mg/(kgrmo)
50 mg/d
300 mg/mo
100 mg/w
25 mg q.o. w
q.o.d.
300 mg/mo
100 mg 2 1 w
50 mg 2 1 w
31w
200 mg/w
75 mg/w
300 mg/mo
...
ND
...
100 mg/d
Daily
300 mg/mo
100 mg 2 1 w
50 mg 2 1 w
31w
ND
ND
ND
50 mg/d
Daily
300 mg/mo
100 mg 2 1 w
25 mg 2 1 w
31w
100 mg/d
1500 mg/d
50 mg/(m2rw)
No. of
patients
Time observed
20
21
7.3 mo
12 mo
29
56
Break-through
PCP
AEs
12.5
9.8
15
9.5
14 mo
3.6
12.5
20
8.7
13
14
16 mo
11 mo
15.4
7
5.3
20
15
15
10 mo
11 mo
0
0
0
14
14
12 mo
0
21
52
71
225
76
48
93
103
63
25 w
ND
6
21
6
20
25
5.7
11.7
14.3
4
ND
ND
ND
ND
20
11.7
11.1
1.5
5.8
6.3
10.6
4.4
9
ND
0
4.1
10
30
242
45
178
253
288
276
278
105
505 d
(per py)
Same
Same
36 mo (accumulated risk)
Same
Same
24 mo
5.4
13
9.8
14.5
17.5
18
21
9.4
4
ND
ND
ND
75
79
12
3
115
62
147
24
45
129
20
137
Same
63.4 py
176.2 py
22.8 py
418 pm
1110 pm
164 pm
20 mo
6.9
11.0
3.4
30.7
13
0.9
14
5.8
8
16
44
38
ND
ND
ND
8.5
157
521
536
32
20 mo
(per 100 py)
Same
1y
2.6
18.3
15.5
0
7
27.5
26.8
0
ND
ND
ND
ND
12.4 mo
13.4 mo
160 d
66
68
96
275
211 d
430 d
104
291
449 d
NOTE. AEs Å adverse events; C Å clinical; ND Å not determined or not reported; O Å open label; P Å prospective not randomized; PCP Å Pneumocystis
carinii pneumonia; pm Å patient-months; py Å patient-years; R Å randomized.
* TMP-SMZ dose: 160 – 320 mg of TMP and 800 – 1,600 mg of SMZ.
/ 9c51$$jy36
06-16-98 00:27:17
cida
UC: CID
Downloaded from http://cid.oxfordjournals.org/ by guest on September 9, 2014
[67], 1994, CR
[68], 1994, CR
Drug
198
Hughes
/ 9c51$$jy36
06-16-98 00:27:17
occurred in 55% of patients given 50 mg of dapsone daily,
whereas in another study [39] only 10% of patients had adverse
reactions when given double this dose (100 mg). However,
general comparison of adverse reactions to dapsone and to
other drugs can be made within each study. From review of
all the studies (table 1), one can generally conclude that adverse
reactions occur more frequently with dapsone than with aerosolized pentamidine and that no striking differences are seen
between dapsone and TMP-SMZ.
Some perspective on the relative efficacy of dapsone with
respect to TMP-SMZ and aerosolized pentamidine can be
gleaned from the studies reported. Among the 16 studies in
which dapsone, with and without pyrimethamine, was compared with TMP-SMZ, the rate of break-through PCP was
greater with dapsone in 11 of the studies [53, 55, 58, 60, 66,
68, 70, 71, 76 – 78], and in 5 [39, 56, 73 – 75] the break-through
rates were similar.
In 15 studies dapsone was compared with aerosolized pentamidine [45, 52, 53, 57, 60 – 62, 65, 68 – 70, 72 – 74, 77], and
no statistically significant difference in rates of break-through
PCP were discernible, although in one study [70] PCP occurred
in 14.3% of those receiving dapsone and pyrimethamine and
5.8% of those receiving pentamidine. Salmon-Ce´ron et al. [69]
found lower survival among AIDS patients taking dapsone than
among those receiving aerosolized pentamidine for prophylaxis. This European study randomized 196 AIDS patients to
receive either aerosolized pentamidine (300 mg monthly) or
dapsone (50 mg daily).
After a follow-up (mean { SD) of 13 { 6.4 months, the
study was prematurely terminated because of excessive mortality in the dapsone group; 21% of the 103 patients in the
pentamidine group vs. 42% of the 93 receiving dapsone had
died. The mean CD4 cell count during the study was lower
in the dapsone group. The dapsone preparation used in this
study contained 200 mg of iron protoxalate per tablet. Weinberg [85] suggests the increased iron burden from this formulation might have contributed to the lower survival rate. He
has shown that iron chelators inhibit the growth of P. carinii
in cell culture and are effective in the treatment of PCP in
animals [86, 87].
Bucker et al. [88] utilized a meta-analysis to examine the
efficacy of dapsone (and dapsone plus pyrimethamine), TMPSMZ, and aerosolized pentamidine in patients with HIV infection. The analysis included 4,832 patients in 22 trials. For the
1,548 patients given dapsone, with or without pyrimethamine,
and the 1,800 patients receiving aerosolized pentamidine, the
risk ratio for PCP was 0.90 (95% CI, 0.71 – 1.15). For the 1,484
patients given TMP-SMZ vs. the dapsone group, the risk ratio
of PCP was 0.49 (95% CI, 0.26 – 0.92). For TMP-SMZ vs.
aerosolized pentamidine, the risk ratio of PCP was 0.59 (95%
CI, 0.45 – 0.76).
The report by El Sadr et al. [79] shows atovaquone to be as
effective as dapsone in PCP prophylaxis. Future studies will
place this drug in perspective for PCP prophylaxis.
cida
UC: CID
Downloaded from http://cid.oxfordjournals.org/ by guest on September 9, 2014
in experimental design, dapsone dosages, and intervals of administration. Dosages ranged from 50 to 300 mg/d, with and
without pyrimethamine, and at intervals from daily to weekly.
Dapsone prophylaxis has been compared to that with TMPSMZ, aerosolized pentamidine, fansidar, clindamycin/primaquine, and atovaquone in retrospective and prospective studies
and in randomized and nonrandomized studies. Unfortunately,
no study has been blinded, and most of the studies have not
had a sufficient number of subjects or time of observation to
allow statistically sound conclusions to be drawn. In addition,
studies of TMP plus dapsone, shown to be synergistic in animals [21], have not been done in humans. Instead, pyrimethamine has been used in combination with dapsone, intended
in most studies to extend the spectrum of coverage to T. gondii.
However, there are no studies and little rationale to suggest
that TMP would be less effective than pyrimethamine in combination with dapsone against T. gondii.
Only three studies have compared dapsone prophylaxis with
no prophylaxis. None of these were randomized studies. However,
these comparisons are convincing evidence of the anti–P. carinii
activity of dapsone. Metroka et al. [39] found that 100% of 23
high-risk AIDS patients not given prophylaxis developed PCP
over a period of 9.6 months, whereas only 2 (1.0%) of 173 patients
given 100 mg of dapsone daily had PCP over the same period
of time. Lucas et al. [40] noted PCP in 16 (35%) of 46 patients
not receiving prophylaxis and in 1 (6.3%) of 16 patients taking
100 mg of dapsone once a week. Penco [50] reported the occurrence of PCP in 8 (80%) of 10 patients not receiving prophylaxis
during a 6-month period, while only 1 (10%) of 10 AIDS patients
given 50 mg of dapsone twice weekly had PCP during a 12month period of observation (table 1).
There are no conclusive data to support or to discount the
use of pyrimethamine with dapsone as prophylaxis for PCP
because adequate comparative studies have not been done. In
the small randomized study of 55 patients by Lavelle et al.
[47], dapsone (200 mg/w) was compared with the same dose
plus 25 mg of pyrimethamine per week. Break-through PCP
occurred in 4.3% and 4.5% of the groups, respectively. Adverse
reactions occurred in 13% and 18% of the respective groups.
When the confounding variables in the clinical trials are
considered, no specific dose or schedule of administration
can be selected as more effective than others (see table 1).
In studies with 100-mg daily doses of dapsone alone, rates
of break-through PCP of 1% [39], 0 [42], 2% [56], 12%
[63], 17% [74], 18% [79], and 21% [68] were encountered.
When 100 mg of dapsone was given once a week, breakthrough rates were 2% [44], 4% [43], and 6% [67]. When
dapsone was used alone at a dosage of 50 mg/d, breakthrough PCP occurred in 0 [51], 5% [42], 5.7% [69], 6.5%
[53], and 13% of patients [77].
Accurate comparison of adverse reaction rates among the
clinical trials reported is not possible because of the variations
in the definitions for adverse events, periods of observation, and
other factors. For example, in one study [53] adverse reactions
CID 1998;27 (July)
CID 1998;27 (July)
Dapsone and P. carinii Pneumonia
It seems reasonable to conclude that dapsone is not superior
to any drug as prophylaxis for PCP, is somewhat less effective
than TMP-SMZ, and is equal to aerosolized pentamidine in efficacy. Several factors must be considered in choosing between
dapsone and aerosolized pentamidine for patients who cannot
take TMP-SMZ. For example, infants, children, and some adults
may not be able to take aerosolized pentamidine, and aerosol
administration may be hazardous when the patient has a contagious respiratory tract infection. Cost is also a major factor.
Cost of Prophylaxis
Adverse Effects
Adverse effects of dapsone include a dose-related hemolysis
seen in most patients receiving high dosages of §200 mg/d.
Methemoglobinemia may occur at symptomatic and asymptomatic levels. Peripheral motor weakness may also occur with
high doses. Adverse reactions unrelated to dosage include
agranulocytosis, aplastic anemia, a variety of cutaneous reactions, and a ‘‘sulfone syndrome’’ (fever, exfoliative dermatitis,
jaundice, lymphadenopathy, anemia, and methemoglobinemia)
believed to be a hypersensitivity reaction occurring after 6 – 8
weeks of treatment.
Although adverse reactions are fairly common with dapsone,
fatalities are rare. Useful information on toxicity has come
from studies of a patient without AIDS who consumed a single
2,500-mg dose of dapsone, 25 times the usual daily dose [91].
The next day he was noted to have blue skin. Twenty hours
post-dose the methemoglobin concentration was 2.5 g/dL (25%
of total hemoglobin). The plasma dapsone level was 18.8
mg/L. The patient had an uneventful recovery without specific
therapy.
/ 9c51$$jy36
06-16-98 00:27:17
Balestrini et al. [92] studied the adverse events in 261 HIVinfected patients taking dapsone as prophylaxis for PCP. Seventy-one patients (27%) stopped taking the drug; 23 had rash;
10 had hematologic toxicity; 10 had malaise or nausea; and 10
died of causes not related to dapsone. Because of the doubleblind, randomized design of the study by Medina et al. [93],
a valid comparison of adverse effects from dapsone/TMP and
TMP-SMZ can be made. Patients with known allergy to any
of the drugs were excluded from the study. The drugs were
given for the treatment of PCP. Dosages used were 20 mg of
TMP plus 100 mg of SMZ/(kgrd) and 20 mg of TMP/(kgrd)
plus 100 mg (total dose) of dapsone daily.
Major toxic effects that required a change to another drug
occurred in 9 (30%) of 30 patients receiving dapsone/TMP and
in 17 (57%) of 30 patients receiving TMP-SMZ (P õ .025).
Abnormally high liver transaminase levels occurred in 1 and
6, neutropenia (õ750 neutrophils/mm3) in 1 and 5, thrombocytopenia in 1 and 1, severe rash in 3 and 3, nausea and vomiting
in 2 and 2, a decline in hematocrit by §25% in 0 and 0, and
methemoglobinemia (ú20%) in 1 and 0 of the patients receiving dapsone/TMP and TMP-SMZ, respectively. Therapeutic
efficacy was similar in the two groups.
Beumont et al. [94] assessed the safety of dapsone prophylaxis
in patients who had previously been found intolerant of TMPSMZ. Of 75 patients subsequently given dapsone, the overall
incidence of adverse events was 39%. Rash (16%) and anemia
(23%) were the most common events. However, when each case
was evaluated critically, only three cases of anemia (4%) and two
cases of rash (3%) were considered ‘‘likely related’’ to dapsone.
Only five (6.7%) of the 75 patients had the same adverse event
as previously experienced with TMP-SMZ.
A retrospective review of 89 patients receiving dapsone because of prior adverse reactions to TMP-SMZ showed 56%
experienced single or multiple adverse reactions (maculopapular rash in 27 patients, CNS symptoms in 15, gastrointestinal
symptoms in 8, and anemia in 12) [95].
Few HIV-infected patients who receive PCP prophylaxis
take only the drug or drugs prescribed for this purpose. The
concomitant use of several drugs adds to the complexity in
sorting out the adverse effects of one specifically. Moore et al.
[96] attempted to quantify the incidence of these effects in
clinical practice. They calculated the overall adverse event rates
from the use of dapsone, TMP-SMZ, zidovudine, didanosine,
and zalcitabine in an observational cohort of 1,450 HIV-infected patients with CD4/ lymphocyte counts of £500/mm3.
The rates are given in table 2. The adverse events from dapsone
were not related to CD4/ lymphocyte count, race, gender, age,
or injection drug use.
A desensitization scheme has been evaluated by Metroka
et al. [97] for patients with hypersensitivity-like reactions to
dapsone. Fourteen patients who had fever (ú397C) and diffuse
erythematous maculopapular rash that appeared 8 – 14 days
after initiation of dapsone therapy were desensitized over a
period of 42 days. Daily doses of dapsone escalated from
cida
UC: CID
Downloaded from http://cid.oxfordjournals.org/ by guest on September 9, 2014
A dapsone regimen is the most economical currently available for prophylaxis for both individual and population use.
The annual cost (in $U.S.) of PCP prophylaxis for an adult is
$8,190 for atovaquone, $1,200 for aerosolized pentamidine,
and $30 for TMP-SMZ (3 days a week), in comparison with
$70 for daily dapsone and $10 for weekly dapsone [89]. However, efficacy and safety must be factored into the cost equation.
Using a decision-analytic model, Freedberg et al. [90] assessed
the effectiveness and costs of dapsone, TMP-SMZ, and aerosolized pentamidine as initial prophylaxis for PCP in HIV-infected
individuals with CD4/ lymphocyte counts of õ200/mm3. Each
strategy increased life expectancy by about 18%, compared
with that with no prophylaxis. Annual per-person costs were
$400 for dapsone, $700 for TMP-SMZ, and $1,680 for aerosolized pentamidine. They estimated that for 100,000 people receiving prophylaxis with TMP-SMZ or dapsone (and switching
to aerosolized pentamidine if oral therapy is not tolerated), the
savings in medical costs is between $8 million and $124 million
per year.
199
200
Hughes
Table 2. Adverse effects associated with drugs used in the treatment
of 1,450 HIV-infected men with CD4/ cell counts of £500/mm3.
Adverse event rate
(per 100 person-years)
Drug
Dapsone
Didanosine
Zidovudine
Trimethoprim-sulfamethoxazole
Zalcitabine
16.2%
24.1%
26.3%
26.3%
37.0%
NOTE. Data are from [96].
/ 9c51$$jy36
06-16-98 00:27:17
Single cases of symptomatic methemoglobinemia have been
reported [103 – 105]. Specific and effective therapy is the infusion of methylene blue (1.0 mg/kg).
Theoretically, inhibition of N-acetyl-transferase (NAT) – dependent acetylation of dapsone could increase the plasma concentration of dapsone, shifting the biotransformation pathway
to the P450-mediated formation of hydroxylamine, a toxic metabolite of dapsone. In in vitro studies of human liver cytosol
and clinically relevant concentrations of drugs used in the management of AIDS patients, pyrimethamine modestly (by 30%)
inhibited MADDS formation [106]. No inhibition was observed
with atovaquone, sulfadiazine, clarithromycin, TMP, ketoconazole, and fluconazole. This experiment suggests that NAT-2 is
the predominant liver NAT isoform acetylating dapsone in vivo
and that coadministration with other anti – opportunistic infection drugs should not inhibit this acetylation pathway.
Studies to elucidate the mechanism of increases in serum
creatinine level, sometimes associated with the administration
of pyrimethamine plus dapsone, show this abnormality is due
to the renal tubular secretion of creatinine by pyrimethamine.
The inhibition is reversible and does not affect the glomerular
filtration rate [107].
Wu and DuBois [108] demonstrated that dapsone inhibits
oxidation of pyruvate in rat and mouse tissues by interfering
with the pyruvate oxidase system. Because thymine pyrophosphate is needed for normal function of pyruvic oxidase and
because thymine deficiency is associated with symptoms of
dapsone poisoning, an animal study was done to supplement
dapsone administration with thymine hydrochloride. The results showed that the LD50 for control rats given dapsone alone
was 233 mg/kg, whereas if dapsone were given with thymine
hydrochloride the LD50 was 425 mg/kg. No clinical studies
have evaluated the use of thymine in dapsone toxicity.
One case of dapsone toxicity with megaloblastic pancytopenia associated with vitamin B12 deficiency has been reported
[109], suggesting that supplemental folic acid might be indicated when this is likely to occur.
Conclusion
Dapsone is effective in the prevention of PCP and in combination with TMP is effective in the treatment of this pneumonitis. It is not the drug of first choice for either prophylaxis or
treatment for patients who can take TMP-SMZ. The data currently available are adequate to consider it as a drug of second
choice for patients who have experienced adverse effects from
TMP-SMZ. Most but not all patients with such effects will be
able to take dapsone safely. The most serious adverse effects
from dapsone are dose-related hemolytic anemia, peripheral
motor weakness, and methemoglobinemia as well as dose-unrelated granulocytopenia, aplastic anemia, and cutaneous reactions such as the sulfone syndrome.
Although the number of studies to clearly define the optimal
dose and schedule for administration is limited, the following
cida
UC: CID
Downloaded from http://cid.oxfordjournals.org/ by guest on September 9, 2014
0.01 mg initially to 90 mg by day 37. Thirteen of the 14 patients
were successfully desensitized and once again were given dapsone prophylaxis for up to 7 months at the full dosage of 100
mg/d. The 14th patient developed a recurrent diffuse rash on
day 42.
Holtzer et al. [98] studied 60 HIV-infected patients who had
hypersensitivity reactions (anaphylaxis, rash, hives, pruritis, or
drug fever) to TMP-SMZ and were subsequently given dapsone
as prophylaxis for PCP. Thirteen (22%) of the 60 patients also
had hypersensitivity reactions to dapsone. Four (30.8%) of the
13 patients were able to continue receiving dapsone despite
the adverse reaction. Thus, up to 85% of patients with adverse
reactions to TMP-SMZ might be expected to tolerate prophylaxis with dapsone.
The classic sulfone syndrome (fever, hemolytic anemia, and
fulminant hepatitis) was reported in the first fatal case of dapsone toxicity [99]. Mole-Boetani et al. [100] reported the first
case of the sulfone syndrome involving a patient with AIDS
and reviewed the 22 cases of sulfone syndrome in non-AIDS
patients reported in the literature. The AIDS patient’s syndrome
resolved, and he was discharged after 10 days in the hospital.
Methemoglobinemia in HIV-infected patients receiving dapsone has been reported infrequently, although this is wellknown as a toxic effect from its early use in non-AIDS patients.
Sin et al. [101] described five AIDS patients who had symptomatic methemoglobinemia while taking either primaquine or dapsone alone or in combination. Two cases resulted from intentional overdoses of dapsone, and three cases developed within
a few days of starting primaquine while the patients were receiving dapsone. Four cases required iv methylene blue, supplemental oxygen, and RBC transfusion.
It is well-known that the risk of methemoglobinemia is increased greatly if two or more drugs, such as primaquine and
dapsone, known to cause this condition, are combined [102].
Blood gas studies and pulse oximetry may not be affected by
methemoglobinemia in the usual concentrations encountered
with dapsone toxicity. However, with a normal cardiorespiratory system and 100% methemoglobinemia, an oxygen saturation of 85% may be expected with use of conventional pulse
oximetry [96]. Co-oximetry, which measures all major hemoglobin species, is accurate in this setting.
CID 1998;27 (July)
CID 1998;27 (July)
Dapsone and P. carinii Pneumonia
References
1. Hughes WT, Smith BL. Efficacy of diaminodiphenylsulfone and other
drugs in murine Pneumocystis carinii pneumonitis. Antimicrob Agents
Chemother 1984; 26:436 – 40.
2. Windholz M, ed. The Merck index. 9th ed. Rahway, NJ: Merck and Co,
1976:370.
3. Voeller D, Kovacs J, Andrawis V, et al. Interaction of Pneumocystis
carinii dihydropteroate synthase with sulfonamides and diaminodiphenylsulfone (dapsone). J Infect Dis 1994; 169:456 – 9.
4. Cushion MT. In vitro studies of Pneumocystis carinii. J Protozool 1989;
36:45 – 52.
5. Anderson R, Gatner MS, van Rensburg CE, et al. In vitro and in vivo
effects of dapsone on neutrophil and lymphocyte function in normal
individuals and patients with lepromatous leprosy. Antimicrob Agents
Chemother 1981; 19:495 – 503.
6. Lawrsen AL, Rungby J, Anderson PL. Decreased activation of the respiratory burst in neutrophils from AIDS patients with previous Pneumocystis carinii pneumonia. J Infect Dis 1995; 172:497 – 505.
7. Bozeman PM, Learn DB, Thomas EL. Inhibition of the human leukocyte
enzymes myeloperoxidase and eosinophil peroxidase by dapsone. Biochem Pharmacol 1992; 44:553 – 63.
8. Duval X, Clayette P, Dereddre-Bosquet N, et al. Dapsone and HIV-1
replication in primary cultures of lymphocytes and monocyte-derived
macrophages. AIDS 1997; 11:943 – 4.
9. Opravil M, Joos B, Luthy R. Levels of dapsone and pyrimethamine in
serum during once-weekly dosing for prophylaxis of Pneumocystis
carinii pneumonia and toxoplasmic encephalitis. Antimicrob Agents
Chemother 1994; 38:1197 – 9.
10. USP dispensing information — volume I: drug information for health care
professionals. 15th ed. Rockville, MD: The United States Pharmacopeial Convention, 1995:1041 – 4.
/ 9c51$$jy36
06-16-98 00:27:17
11. Gatti G, Casazza R, Miletich F, Cruciani M, Bassetti D. Pharmacokinetics
of dapsone in human immunodeficiency virus – infected children. Antimicrob Agents Chemother 1995; 39:1101 – 6.
12. Metroka CE, McMechan MF, Andrada R, Laubenstein LJ, Jacobus DP.
Failure of prophylaxis with dapsone in patients taking dideoxyinosine
[letter]. N Engl J Med 1991; 325:737.
13. Mirochnick M, Cooper E, McIntosh K. Pharmacokinetics of daily and
weekly dapsone in HIV-infected children. In: Program and abstracts
of the 3rd Conference on Retroviruses and Opportunistic Infections.
Alexandria, Virginia: Infectious Diseases Society of America, 1996:
159.
14. Lee BL, Safrin S, Makrides V, Gambertoglio JG. Zidovudine, trimethoprim, and dapsone pharmacokinetic interactions in patients with human
immunodeficiency virus infection. Antimicrob Agents Chemother
1996; 40:1231 – 6.
15. Peters JH, Murray JF, Gordon GR, et al. Effect of rifampicin on the
disposition of dapsone in Malaysian leprosy patients [abstract]. Fed
Proc 1997; 36:996.
16. Horowitz HW, Jorde UP, Wormser GP. Drug interactions in use of dapsone for Pneumocystis carinii prophylaxis. Lancet 1992; 339:747.
17. Gatti G, Merighi M, Hossein J, et al. Population pharmacokinetics of
dapsone administered biweekly to human immunodeficiency virus –
infected patients. Antimicrob Agents Chemother 1996; 40:2748 – 58.
18. Lee BL, Medina I, Benowitz NL, Jacob P, Wofsy CB, Mills J. Dapsone,
trimethoprim, and sulfamethoxazole plasma levels during treatment of
pneumocystis pneumonia in patients with the acquired immunodeficiency syndrome (AIDS): evidence of drug interactions. Ann Intern
Med 1989; 110:606 – 11.
19. Cruciani M, Gatti G, Mengoli C, et al. Penetration of dapsone into pulmonary lining fluid of human immunodeficiency virus type-1 infected
patients. Antimicrob Agents Chemother 1997; 41:1077 – 81.
20. Falloon J, Lavelle J, Ogata-Arakaki D, et al. Pharmacokinetics and safety
of weekly dapsone and dapsone plus pyrimethamine for prevention
of pneumocystis pneumonia. Antimicrob Agents Chemother 1994; 38:
1580 – 7.
21. Hughes WT, Smith BL. Efficacy of diaminodiphenylsulfone and other
drugs in murine Pneumocystis carinii pneumonitis. Antimicrob Agents
Chemother 1984; 26:436 – 40.
22. Hughes WT, Gray VL, Gutheridge WE, et al. Efficacy of a hydroxynaphthoquinone, 566C80, in experimental Pneumocystis carinii pneumonitis. Antimicrob Agents Chemother 1990; 34:225 – 8.
23. Hughes WT. Comparison of dosages, intervals, and drugs in the prevention of Pneumocystis carinii pneumonia [erratum appears in Antimicrob Agents Chemother 1988; 32(8):1294]. Antimicrob Agents Chemother 1988; 32:623 – 5.
24. Walzer PD, Kim CK, Foy JM, Linke MJ, Cushion MT. Inhibitors of
folic acid synthesis in the treatment of experimental Pneumocystis
carinii pneumonia. Antimicrob Agents Chemother 1988; 32:96 – 103.
25. Gonzalez-Ruiz A, Haworth SJ, O’Neil AB, Warhurst DC. Dapsone in
low doses prevents Pneumocystis carinii pneumonia in the rat model.
J Infect 1991; 22:143 – 52.
26. Comley JC, Sterling AM. Effect of atovaquone and atovaquone drug
combinations on prophylaxis of Pneumocystis carinii pneumonia in
SCID mice. Antimicrob Agents Chemother 1995; 39:806 – 11.
27. Walzer PD, Foy J, Steele P, White M. Synergistic combinations of Ro
11-8958 and other dihydrofolate reductase inhibitors with sulfamethoxazole and dapsone for therapy or experimental pneumocystosis. Antimicrob Agents Chemother 1993; 37:1436 – 43.
28. Brun-Pascaud M, Girard PM, Chau F, et al. Experimental evaluation of
PS-15 (a biguanide folate antagonist) alone or combined with dapsone
in dual pneumocystosis and toxoplasmosis infection in a rat model.
In: Program and abstracts of the 2nd National Conference on Human
Retroviruses and Related Infections. 1995:110.
29. Hughes WT, Smith BL, Jacobus DP. Successful treatment and prevention
of murine Pneumocystis carinii pneumonitis with 4,4*-sulfonylbisformanilide. Antimicrob Agents Chemother 1986; 20:509 – 10.
cida
UC: CID
Downloaded from http://cid.oxfordjournals.org/ by guest on September 9, 2014
recommendations are probably adequate: for prophylaxis, (1)
100 mg of dapsone daily or dapsone (50 mg daily) plus pyrimethamine (50 mg once weekly) plus leucovorin (25 mg once
weekly) or (2) dapsone (200 mg) plus pyrimethamine (75 mg)
plus leucovorin (25 mg) once weekly, orally, for adults. The
dose recommended for children is 2.0 mg/(kgrd), not to exceed
100 mg daily. For treatment of PCP, TMP (20 mg/[kgrd]) plus
dapsone (200-mg [total dose] daily) is adequate.
As with any drug, attention should be given to the use of
concomitant medication. Information is limited with regard to
drug interactions with dapsone. Especially for patients with
impaired hepatic and renal function, the use of drugs such as
the antiretroviral nucleosides, antacids, and rifampin should be
carefully monitored.
The combination of TMP with dapsone for prophylaxis has
been essentially unexplored in human studies, although prophylaxis studies in animals and treatment studies in humans suggest
a synergistic effect on efficacy. In circumstances where economy is an issue, dapsone is the least expensive effective prophylaxis available.
Forty years after dapsone was first marketed in the United
States for the treatment of leprosy, indications for its use have
changed dramatically to include PCP, an obscure and insignificant disease in 1957. It is within reason to expect that this old
drug will remain with us for a long time and perhaps find new
indications in the future.
201
202
Hughes
/ 9c51$$jy36
06-16-98 00:27:17
46.
47.
48.
49.
50.
51.
52.
53.
54.
55.
56.
57.
58.
59.
60.
of the 7th International Conference on AIDS (Florence). Florence:
Institute Superiore di Sanita`, 1991:239.
Cruciani M, Danzi MC, Perri G, et al. Dapsone in secondary prophylaxis
of P.C.P. [abstract no W.B.2208]. In: Program and abstracts of the
7th International Conference on AIDS (Florence). Florence: Istituto
Superiore di Sanita`, 1991:234.
Lavelle J, Falloon J, Morgan A, et al. Weekly dapsone and dapsone/
pyrimethamine for PCP prophylaxis [abstract no W.B.2207]. In: Program and abstracts of the 7th International Conference on AIDS (Florence). Florence: Istituto Superiore di Sanita`, 1991:233.
Miller S. Efficacy and safety of twice weekly dapsone as prophylaxis for
Pneumocystis carinii pneumonia [abstract no W.B.2197]. In: Program
and abstracts of the 7th International Conference on AIDS (Florence).
Florence: Istituto Superiore di Sanita`, 1991:231.
Clotet B, Sirera G, Romeu J, et al. Twice-weekly dapsone-pyrimethamine
for preventing PCP and cerebral toxoplasmosis [letter]. AIDS 1991;
5:601 – 2.
Penco G, Crisalli MP, Guida B, et al. Dapsone in the prophylaxis of
Pneumocystis carinii pneumonia [abstract no W.B.2181]. In: Program
and abstracts of the 7th International Conference on AIDS (Florence).
Florence: Istituto Superiore di Sanita`, 1991:227.
Payen MC, Franchioly P, Gerard M, et al. Daily dapsone versus pyrimethamine-sulfadoxine (fansidar) as primary prophylaxis against Pneumocystis carinii pneumonia (PCP) [abstract no TH.B.43]. In: Program
and abstracts of the 7th International Conference on AIDS (Florence).
Florence: Istituto Superiore di Sanita`, 1991:66.
Slavin MA, Hoy JF, Stewart K, Pettinger MB, Lucas CR, Kent SJ.
Oral dapsone versus nebulized pentamidine for Pneumocystis carinii
pneumonia prophylaxis: an open randomized prospective trial to assess
efficacy and haematological toxicity. AIDS 1991; 6:1169 – 74.
Martin MA, Cox PH, Beck K, et al. A comparison of the effectiveness
of three regimens in the prevention of Pneumocystis carinii pneumonia
in human immunodeficiency virus – infected patients. Arch Intern Med
1992; 152:523 – 8.
Hill HE, Wallace M, Kennedy C, et al. Prophylaxis of Pneumocystis
carinii pneumonia (PCP) with dapsone: evaluation of toxicity and
cross-reactivity with trimethoprim-sulfamethoxazole [abstract no
PoB3301]. In: Program and abstracts of the 7th International Conference on AIDS (Amsterdam). Amsterdam: CONGREX Holland BV,
1992:137.
Coker RJ, Nieman R, McBride M, et al. Co-trimoxazole versus dapsonepyrimethamine for prevention of Pneumocystis carinii pneumonia [letter, comment]. Lancet 1992; 340:1099.
Blum RN, Miller LA, Gaggini LC, Cohn DL. Comparative trial of dapsone versus trimethoprim-sulfamethoxazole for primary prophylaxis
of Pneumocystis carinii pneumonia. J Acquir Immunodefic Syndr
1992; 5:341 – 7.
Pont M, Clotet B, Sirara G, et al. Dapsone / pyrimethamine twice weekly
(group A) versus once weekly associated with aerosolized pentamidine
once monthly (group B) to prevent P. carinii pneumonia events in
AIDS [abstract no PuB 7449]. In: Program and abstracts of the 8th
International Conference on AIDS (Amsterdam). Amsterdam: CONGREX Holland BV, 1992:123.
Podzamczer D, Santin M, Jimenez J, et al. Thrice-weekly cotrimoxazole
is better than weekly dapsone-pyrimethamine for the primary prevention of Pneumocystis carinii pneumonia in HIV-infected patients.
AIDS 1993; 7:501 – 6.
Jorde UP, Horowitz HW, Wormser G, et al. Utility of dapsone for prophylaxis of Pneumocystis carinii pneumonia in trimethoprim-sulfamethoxazole-intolerant, HIV-infected individuals. AIDS 1993; 7:355 – 9.
Mallolas J, Zamora L, Gatell JM, et al. Primary prophylaxis for Pneumocystis carinii pneumonia: a randomized trial comparing cotrimoxazole,
aerosolized pentamidine and dapsone plus pyrimethamine. AIDS 1993;
7:59 – 64.
cida
UC: CID
Downloaded from http://cid.oxfordjournals.org/ by guest on September 9, 2014
30. Leoung GS, Mills J, Hopewell PC, Hughes W, Wofsy C. Dapsonetrimethoprim for Pneumocystis carinii pneumonia in the acquired immunodeficiency syndrome. Ann Intern Med 1986; 105:45 – 8.
31. Mills J, Leoung G, Medina I, Hopewell PC, Hughes WT, Wofsy C.
Dapsone treatment of Pneumocystis carinii pneumonia in the acquired
immunodeficiency syndrome. Antimicrob Agents Chemother 1988; 32:
1057 – 60.
32. Stansell JD, Sattler FR, Dube M, et al. Randomized trial of trimetrexate
(TMTX), leucovorin (LV) and dapsone (DAP) vs. trimethoprim/sulfamethoxazole (T/S) for Pneumocystis carinii pneumonia (PCP): clinical
and pharmacokinetic results. (abstract no 863). In: Program and abstracts of the annual meeting of the American Society for Clinical
Oncology 1996:15.
33. Safrin S, Sattler FR, Lee BL, et al. Dapsone as a single agent is suboptimal
therapy for Pneumocystis carinii pneumonia. J Acquir Immune Defic
Syndr 1991; 4:244 – 9.
34. Safrin S, Finkelstein DM, Feinberg J, et al. Comparison of three regimens
for treatment of mild to moderate Pneumocystis carinii pneumonia in
patients with AIDS: a double-blind, randomized trial of oral trimethoprim-sulfamethoxazole, dapsone-trimethoprim, and clindamycin-primaquine. ACTG 108 Study Group [see comments]. Ann Intern Med
1996; 124:792 – 802.
35. Wharton JM, Coleman DL, Wofsy CB, et al. Trimethoprim-sulfamethoxazole or pentamidine for Pneumocystis carinii pneumonia in the acquired immunodeficiency syndrome: a prospective randomized trial.
Ann Intern Med 1986; 105:37 – 44.
36. Rouquet RM, Rose P, Carre P, et al. Pneumocystis carinii pneumonia
presenting with multiple bilateral excavations: complete regression
with the association of dapsone-trimethoprim (abstract no PuB 7485)
In: Program and abstracts of the 8th International Conference on AIDS.
Amsterdam: CONGREX Holland BV, 1992:129.
37. Edelson PJ, Metroka CE, Friedman-Kien A. Dapsone, trimethoprim-sulfamethoxazole, and the acquired immunodeficiency syndrome [letter].
Ann Intern Med 1985; 103:963.
38. Jorde UP, Horowitz HW, Wormser GP. Significance of drug interactions
with rifampin in Pneumocystis carinii pneumonia prophylaxis [letter,
comment]. Arch Intern Med 1992; 152:2348.
39. Metroka CE, Jacobus D, Lewis N. Successful chemoprophylaxis for
pneumocystis with dapsone or bactrim [abstract no T.B.O.4 5:196].
In: Program and abstracts of the 5th International Conference on AIDS
(Montreal). Ottawa: International Development Research Centre, 1989:
196.
40. Lucas CR, Sandland AM, Mijch A, Simpson JM. Primary dapsone chemoprophylaxis for Pneumocystis carinii pneumonia in immunocompromised patients infected with the human immunodeficiency virus.
Med J Aust 1989; 151:30 – 3.
41. Lang OS, Kessinger JM, Tucker RM, Greene SI, Deresinski SC, Stevens
DA. Low-dose dapsone prophylaxis of Pneumocystis carinii [abstract
no T.B.O.5]. In: Program and abstracts of the 5th International Conference on AIDS (Montreal). Ottawa: International Development Research Centre, 1989:196.
42. Kemper CA, Tucker RM, Lang OS, et al. Low-dose dapsone prophylaxis
of Pneumocystis carinii pneumonia in AIDS and AIDS-related complex. AIDS 1990; 4:1145 – 8.
43. Ogata-Arakai D, Falloon J, Lavelle J, et al. The safety of weekly dapsone
and weekly dapsone / pyrimethamine as pneumocystis prophylaxis
[abstract no. Th.B.411]. In: Programs and abstracts of the 6th International Conference on AIDS (San Francisco). 1990:224.
44. Hughes WT, Kennedy W, Dugdale M, et al. Prevention of Pneumocystis
carinii pneumonitis in AIDS patients with weekly dapsone [letter] [see
comments]. Lancet 1990; 336:1066.
45. Kent SJ, Slavin M, Hoy JF, et al. Followup of an open, randomised,
prospective comparison of oral dapsone and nebulised pentamidine for
PCP prophylaxis [abstract no W.B.2228]. In: Program and abstracts
CID 1998;27 (July)
CID 1998;27 (July)
Dapsone and P. carinii Pneumonia
/ 9c51$$jy36
06-16-98 00:27:17
76. Barber BA, Pegram PS, High KP. Clindamycin/primaquine as prophylaxis for Pneumocystis carinii pneumonia. Clin Infect Dis 1996; 23:
718 – 22.
77. Warnoc AC, Rimland D. Comparison of trimethoprim-sulfamethoxazole,
dapsone and pentamidine in the prophylaxis of Pneumocystis carinii
pneumonia. Pharmacotherapy 1996; 16:1030 – 8.
78. Zamora L, Mallolas J, Gatell JM. Prophylaxis of pneumocystis pneumonia and toxoplasmosis [letter, comment]. Ann Intern Med 1996; 124:
1096.
79. El-Sadr W, Murphy R, Luskin-Hawk R, et al. Atovaquone versus dapsone
in the prevention of P. carinii pneumonia in patients intolerant to
trimethoprim and/or sulfamethoxazole [abstract 769]. In Program and
abstracts of the 35th meeting of the Infectious Diseases Society of
America (San Francisco). Washington, DC: Infectious Diseases Society of America, 1997.
80. Maltezou HC, Petropoulos D, Choroszy M, et al. Dapsone for Pneumocystis carinii prophylaxis in children undergoing bone marrow transplantation. Bone Marrow Transplant 1997; 20:879 – 81.
81. Opravil M, Pechere M, Lazzarin A, et al. Dapsone/pyrimethamine may
prevent mycobacterial disease in immunosuppressed patients infected
with the human immunodeficiency virus. Clin Infect Dis 1995; 20:
244 – 9.
82. Centers for Disease Control and Prevention. 1997 USPHS/IDSA guidelines for the prevention of opportunistic infections in persons infected
with human immunodeficiency virus. MMWR 1997; 46(RR-12):1 – 46.
83. Centers for Disease Control. Update: acquired immunodeficiency syndrome — United States. MMWR 1986; 35:17 – 21.
84. Saah AJ, Hoover D, Peng Y, et al. Predictors for failure of Pneumocystis
carinii pneumonia prophylaxis. JAMA 1995; 273:1197 – 202.
85. Weinberg GA. Iron overload as a mechanism for the lowered survival
in AIDS patients receiving dapsone-iron protoxalate for secondary
prophylaxis for Pneumocystis carinii pneumonia. JID 1996; 174:241.
86. Weinberg GA. Iron chelators as therapeutic agents against Pneumocystis
carinii. Antimicrob Agents Chemother 1994; 38:997 – 1003.
87. Weinberg GA, Boehart JR, Shanzer A. Further studies on the activities
of iron chelators against Pneumocystis carinii (abstract B73). In: Program and abstracts of the 35th Interscience Conference on Antimicrobial Agents and Chemotherapy (San Francisco). Washington, DC:
American Society for Microbiology, 1995.
88. Bucher HC, Griffith L, Guyatt GH, Opravil M. Meta-analysis of prophylactic treatments against Pneumocystis carinii pneumonia and toxoplasmic encephalitis in HIV-infected patients. In: Program and abstracts of the 11th International Conference on AIDS (Vancouver).
1996:315.
89. Feder HM, Milch LR. Letter to the editor. N Engl J Med 1997; 336:949 –
60.
90. Freedberg KA, Cohen CJ, Cotton DJ, Tosteson AN. Prophylaxis for
Pneumocystis carinii pneumonia (PCP): a cost-effectiveness analysis
[abstract no T.B.P.68]. In: Program and abstracts of the 5th International Conference on AIDS (Montreal). Ottawa: International Development Research Centre, 1989:298.
91. Woodhouse KW, Henderson DB, Charlton B, et al. Acute dapsone poisoning: clinical features and pharmacokinetic studies. Human Toxicol
1983; 3:507 – 10.
92. Balestrini AA, Erskine D, Lant AF, Hawkins D, et al. A study of the
toxicity of dapsone as a PCP prophylactic agent (abstract no. PuB
7168). In: Program and abstracts of the 8th International Conference
on AIDS (Amsterdam). Amsterdam: CONGREX Holland BV, 1992:
77.
93. Medina I, Mills J, Leoung G, Hopewell PC, et al. Oral therapy for
Pneumocystis carinii pneumonia in the acquired immunodeficiency
syndrome: a controlled trial of trimethoprim-sulfamethoxazole versus
trimethoprim-dapsone. N Engl J Med 1990; 323:776 – 82.
94. Beumont MG, Graziani A, MacGregor RR. Safety of dapsone as PCP
prophylaxis in HIV-infected patients with TMP/SMX intolerance. In:
cida
UC: CID
Downloaded from http://cid.oxfordjournals.org/ by guest on September 9, 2014
61. Torres RA, Barr M, Thorn M, et al. Randomized trial of dapsone and
aerosolized pentamidine for the prophylaxis of Pneumocystis carinii
pneumonia and toxoplasmic encephalitis. Am J Med 1993; 95:573 –
83.
62. Girard PM, Landman R, Gaudebout C, et al. Dapsone-pyrimethamine
compared with aerosolized pentamidine as primary prophylaxis against
Pneumocystis carinii pneumonia and toxoplasmosis in HIV infection.
The PRIO Study Group. N Engl J Med 1993; 328:1514 – 20.
63. Stavola JJ, Noel GJ. Efficacy and safety of dapsone prophylaxis against
Pneumocystis carinii pneumonia in human immunodeficiency virus –
infected children. Pediatr Infect Dis J 1993; 12:644 – 7.
64. Grunewald T, Bergmann F, Eljaschewitsch J, et al. Anitprotozoal prophylaxis in AIDS patients — results of a prospective randomized study
comparing dapsone/pyrimethamine and sulfadiazine/pyrimethamine
[abstract no WS-B13-3]. In: Program and abstracts of the 9th International Conference on AIDS (Berlin). Berlin: Institute for Clinical and
Experimental Virology of the Free University of Berlin, 1993:56.
65. Dorrell L, McCallum AK, Snow MH, et al. Dapsone-pyrimethamine (D/
P) versus aerosolized pentamidine (AP) as prophylaxis against Pneumocystis carinii pneumonia (PCP) in HIV infection [abstract no POB10-1420]. In: Program and abstracts of the 9th International Conference on AIDS (Berlin). Berlin: Institute for Clinical and Experimental
Virology of the Free University of Berlin, 1993:372.
66. Tocchetti A, Tambini R, Allegro A, et al. Four different regimens for
prevention of Pneumocystis carinii pneumonia and toxoplasma encephalitis in HIV-infected patients. AIDS 1994; 8:272 – 3.
67. Spencer M, Andrews L, Ross J, et al. Dapsone prophylaxis in HIV
positive inner city population [abstract no. PB0608]. In: Program and
abstracts of the 10th International Conference on AIDS (Yokahama).
1994:149.
68. Nachman SA, Mueller BU, Mirochnick M, et al. High failure rate of
dapsone and pentamidine as Pneumocystis carinii pneumonia prophylaxis in human immunodeficiency virus – infected children. Pediatr Infect Dis J 1994; 13:1004 – 6.
69. Salmon-Ceron D, Fontbonne A, Saba J, et al. Lower survival in AIDS
patients receiving dapsone compared with aerosolized pentamidine
for secondary prophylaxis of Pneumocystis carinii pneumonia. Study
group [erratum appears in J Infect Dis 1996; 173(1):277]. J Infect Dis
1995; 172:656 – 64.
70. Antinori A, Murri R, Ammassari A, et al. Aerosolized pentamidine,
cotrimoxazole and dapsone-pyrimethamine for primary prophylaxis of
Pneumocystis carinii pneumonia and toxoplasmic encephalitis. AIDS
1995; 9:1343 – 50.
71. Podzamczer D, Salazar A, Jiminez J, et al. Intermittent trimethoprimsulfamethoxazole compared with dapsone-pyrimethamine for the simultaneous primary prophylaxis of pneumocystis pneumonia and toxoplasmosis in patients infected with HIV. Ann Intern Med 1995; 122:
755 – 61.
72. Opravil M, Hirschel B, Lazzarin A, et al. Once-weekly administration
of dapsone/pyrimethamine vs. aerosolized pneumonia and toxoplasmic
encephalitis in human immunodeficiency virus – infected patients. Clin
Infect Dis 1995; 20:531 – 41.
73. Saah AJ, Hoover DR, Peng Y, et al. Predictors for failure of Pneumocystis
carinii pneumonia prophylaxis. Multicenter AIDS Cohort Study.
JAMA 1995; 273:1197 – 202.
74. Bozzette SA, Finkelstein DM, Spector SA, et al. A randomized trial
of three antipneumocystis agents in patients with advanced human
immunodeficiency virus infection. NIAID AIDS Clinical Trial. N Engl
J Med 1995; 332:693 – 9.
75. Sirera G, Clotet B, Romeu J, et al. A randomized study of primary
prophylaxis of Pneumocystis carinii pneumonia (PCP) and cerebral
toxoplasmosis (CT) with twice weekly dapsone-pyrimethamine versus
thrice weekly co-trimoxazole. In: Program and abstracts of 2nd National Conference on Human Retroviruses and Related Infections.
1995:109.
203
204
95.
96.
97.
98.
100.
Program and abstracts of the 34th Interscience Conference on Antimicrobial Agents and Chemotherapy (Orlando). Washington, DC: American Society for Microbiology, 1994:168.
Schranz J, Walmsley S, Phillips A, Salit I. Dapsone adverse reactions
during prophylaxis of Pneumocystis carinii pneumonia [abstract
no PO-BIO-1510]. In: Program and abstracts of the 9th International Conference on AIDS (Berlin). Berlin: Institute for Clinical
and Experimental Virology of the Free University of Berlin, 1993:
387.
Moore RD, Fortgang I, Keruly J, Chaisson RE. Adverse events from
drug therapy for human immunodeficiency virus disease. Am J Med
1996; 101:34 – 40.
Metroka CE, Lewis NJ, Jacobus DP. Desensitization to dapsone in HIVpositive patients [letter]. JAMA 1992; 267:512.
Holtzer C, Coleman R, Flaherty J. Cross-reactivity and patient outcomes
in HIV-infected patients switched from TMP/SMZ to dapsone due to
hypersensitivity reactions during PCP prophylaxis [abstract no 292].
In: Program and abstracts of the 4th Conference on Retroviruses and
Opportunistic Infections. Washington, DC: American Society for Microbiology, 1997:118.
Chalasani P, Baffoe-Bonnie H, Jurado RL. Dapsone therapy causing
sulfone syndrome and lethal hepatic failure in an HIV-infected patient.
South Med J 1994; 11:1145 – 6.
Mohle-Boetani J, Akula S, Holodny M, Katzenstein D, Garcia C. The
sulfone syndrome dapsone treatment for Pneumocystis carinii pneumonia (PCP) prophylaxis. [abstract no M.B.2219]. In: Program and abstracts of the 7th International Conference on AIDS (Florence). Florence: Istituto Superiore di Sanita`, 1991:236.
/ 9c51$$jy36
06-16-98 00:27:17
CID 1998;27 (July)
101. Sin DD, Shafran SD. Dapsone- and primaquine-induced methemoglobinemia in HIV-infected individuals. J Acquir Immune Defic Syndr Hum
Retrovirol 1996; 12(5):477 – 81.
102. Webster LR Jr. Drugs used in the chemotherapy of protozoal infections:
malaria. In: Goodman and Gilman’s the pharmacological basis of therapeutics. 8th ed. New York: Bergeman Press, 1990:978 – 98.
103. Ruttimann S, Laifer G. Successful treatment of HIV-associated Pneumocystis carinii pneumonia with dapsone plus trimethoprim. Wien Klin
Wochenschr 1992; 104:570 – 3.
104. Gallant JE, Hoehn-Saric E, Smith MD. Respiratory insufficiency from
dapsone-induced methemoglobinemia [letter]. AIDS 1991; 5:1392 – 3.
105. Rydzewski B, Davis R. A case of atypical cyanosis. J Tenn Med Assoc
1995; 88:354 – 5.
106. Palamanda JR, Hickman D, Ward A, et al. Dapsone acetylation by human
liver N-acetyltransferases (NAT) and interaction with anti-opportunistic infection drugs. In: Program and abstracts of the 2nd National
Conference on Human Retroviruses and Related Infections. Washington, DC: American Society for Microbiology, 1995:147.
107. Opravil M, Keusch G, Luthy R. Pyrimethamine inhibits renal secretion
of creatinine. Antimicrob Agents Chemother 1993; 37:1056 – 60.
108. Wu AW, Gray S, Brockmeyer R, Safrin S. Quality of life in a doubleblind randomized trial of 3 oral regimens for mild-to-moderate Pneumocystis carinii pneumonia in AIDS (ACTG 108) [abstract no
Tu.B.112]. In: Program and abstracts of the 11th International Conference on AIDS (Vancouver). 1996:229.
109. McKinsey DS, Durfee D, Kurtin PJ. Megaloblastic pancytopenia associated with dapsone and trimethoprim treatment of Pneumocystis carinii
in the acquired immunodeficiency syndrome. Arch Intern Med 1989;
149:965.
cida
UC: CID
Downloaded from http://cid.oxfordjournals.org/ by guest on September 9, 2014
99.
Hughes