Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
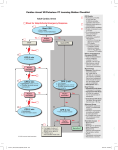
ACLS Cardiac Arrest 1 If unwitnessed Start HPCPR 2 min - Give oxygen - Attach monitor/defibrillator Yes If witnessed begin compressions - Attach monitor/defibrillator No Rhythm shockable? 2 9 VF/VT 3 4 Doses/Details CPR Quality: (per current HPCPR guidelines) - Push hard (> 2 inches [5 cm]) and fast (110/min) allow complete chest recoil - Minimize interruptions in compressions - Avoid excessive ventilation - Rotate compressor every 2 minutes - Ratio: 10 compressions to 1 ventilation simultaneously - Quantitative waveform capnography If PETCO2 <10 mm Hg, attempt to improve CPR quality Asystole/PEA Shock Return of Spontaneous Circulation (ROSC): - Pulse and blood pressure HPCPR 2 min - IV/IO access Rhythm shockable? Shock Energy: - Biphasic: Manufacturer recommendation (120-200J) if unknown, use maximum available Second and subsequent doses should be equivalent, and higher doses may be considered - Monophasic: 360 J No Yes 5 6 Shock 10 HPCPR 2 min HPCPR 2 min - Epinephine every 3-5 min - Consider advanced airway & capnography - IV/IO access - Epinephine every 3-5 min - Consider advanced airway & capnography No Yes Rhythm shockable? Rhythm shockable? Yes 7 11 Shock Advanced Airway: - Supraglottic advance airway or ETT - Waveform capnography to confirm and monitor ET tube placement - With ETT or Supraglottic Airway placed ratio remains 10 compressions to 1 ventilation simultaneously No HPCPR 2 min 8 - Treat reversible causes HPCPR 2 min - Amiodarone - Treat reversible causes No Rhythm shockable? Yes Dr. Larry Smith Approved: 12/12/14 12 - If no signs of return of spontaneous circulation (ROSC), go to 10 or 11 - If ROSC, go to Post-Cardiac Arrest Care protocol Reviewed: 12/10/14 Revised: 12/12/14 Drug Therapy: - Epinephrine IV/IO dose: 1 mg every 3-5 min - Amiodarone IV/IO dose: First dose: 300 mg bolus Second dose: 150 mg Go to 5 or 7 Document: · Detailed Assessment · Treatment · Response to Treatment · SpO2, Cardiac Rhythm, Vital Signs · Verify ETT Placement · Communication with Medical Control Reversible Causes: - Hypovolemia - Hypoxia - Hydrogen ion (acidosis) - Hypo-/hyperkalemia - Hypothermia - Tension pneumothorax - Tamponade, cardiac - Toxins - Thrombosis, pulmonary - Thrombosis, coronary ACLS Cardiac Arrest