Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
2006 Sameerah S.A.R. Lian L.M. With contributions from Lim TO, Goh A, Faridah AMY, Nour Hanah O, Rosminah MD, Radzi H, Menon J, Zainon A, Sharmini, Lim K, Cheng MF, GR Letchumanan, Muruga V, Zanariah H, Oiyammal C, Lim YS, Goh AS, Chong WP, Wan Azman WA, Hooi LS, Zaki M, Zawawi N, Goh BL, Fadilah O, Chang BC, Fong AYY, Sim KH, Haarathi C, Rohna R, Asmah J, Roshidah B, Muralitharan G, Tan AL, Malek R, Lei CM, Masrahayu M, Ngau YY, Lim GC, Wan Ariffin A, M Roslan H, Mary SM, Marzida M, Choy YC, Norliza MA, Siti Nor Aizah A, Salina AA, Ramli MA, Suarn S, Noor Ratna N, Zariah AA, Hanip R, Raymond AA, Azrinorwaty Z, Pang YK, Abdol Malek AZ, Aziah AM, Samsinah HH, Shahirah Z, Saraiza AB, Anura M, Noormah MD, Bethel L, Goh PP, Thiageswari U A publication of the Pharmaceutical Services Division and the Clinical Research Centre Ministry of Health Malaysia May 2009 © Ministry of Health Malaysia Published jointly by: The National Medicines Use Survey Clinical Research Centre, Ministry of Health 3rd Floor, MMA House 124, Jalan Pahang 50286 Kuala Lumpur Malaysia Tel. : (603) 4043 9300 Fax : (603) 4043 9500 e-mail : [email protected] Web site: http://www.crc.gov.my/nmus and The National Medicines Use Survey Pharmaceutical Services Division Ministry of Health Lot 36, Jalan Universiti 124, Jalan Pahang 46350 Petaling Jaya Malaysia Tel. : (603) 7841 3200 Fax : (603) 7968 2222 This report is copyrighted. However it may be freely reproduced without the permission of the National Medicines Use Survey. Acknowledgment would be appreciated. Suggested citation is Sameerah S.A.R, Lian L.M. (Eds). Malaysian Statistics On Medicine 2006. Kuala Lumpur 2009 This report is also published electronically on the website of the National Medicines Use Survey at: http://www.crc.gov.my/nmus Funding: The National Medicines Use Survey is funded by a grant from the Ministry of Health Malaysia (MRG Grant Number: NMUS MRG-CRC-2008-01) ISSN 1823-8300 9 771823 830006 PREFACE Ensuring access to quality and affordable medicines is one important objective of Malaysia’s National Medicines Policy. The National Medicines Use Survey (NMUS) was conducted with the intent to continuously and systematically collect data on medicines in the hope to further improve its use as well as providing a tool for better decision making in the allocation of healthcare resources for the Malaysian population. NMUS is into its fourth year and we are glad to announce the successful publication of its third report, the Malaysian Statistics on Medicines (MSOM) 2006. It is worthwhile to note that the first report MSOM 2004 presented results largely from pilot surveys and using test methods basically to demonstrate that such a project was feasible in a healthcare system such as Malaysia that has many players. In 2005, we scaled up the survey with larger sample size and wider distribution and also refined data processing and statistical methods. For MSOM 2006, data collection was on a similar scale; the data processing was further enhanced to improve quality and the statistical methods reviewed to take into consideration stratification of hospitals which gives more accurate estimates as hospitals of different sizes may have a drug use profile. The data processing and complex statistical methods as explained in the methods section of this publication. Hence results in MSOM 2006, in our opinion are more reliable, more representative and more robust. Eleven new chapters are added, bringing in a total of 25 in MSOM 2006 compared to the 14 chapters in MSOM 2005. We are optimistic that more chapters will be reported in future publications of MSOM. We hope that this MSOM 2006 report will be useful to relevant healthcare professionals serving as a source of reference and baseline for embarking in future research or clinical audits towards improving rational prescribing. We would like to thank all staff who had worked very hard in ensuring the success of the survey, all agencies and institutions that had helped in providing data, all expert panel members for their enthusiasm and contributions in completing the chapter reports and each and everyone who have in one way or another contributed to the success of NMUS and this publication. Pharmaceutical Services Division Clinical Research Centre Ministry of Health Malaysia i ACKNOWLEDGEMENTS The National Medicines Use Survey would like to thank the following for their participation, assistance, support or contributions: • • • • • • • • • • Director General of Health, Ministry of Health Malaysia Deputy Director General of Health (Research and Technical Support), MOH Deputy Director General of Health (Medical Services), MOH Deputy Director General of Health (Public Health), MOH Senior Director of Pharmaceutical Services Division, MOH Senior Director of Oral Health Division, MOH Director, National Pharmaceutical Control Bureau, MOH Director, Clinical Research Centre, MOH Principal Assistant Secretary, Procurement Division, MOH Director, The Office of Electronic Government Application Project (EG-AG), Accountant General’s Department • Director, Government Procurement Division, MOH • Secretary, Information Management Division, MOH • All medical doctors, pharmacists and support personnel who participated in the NMUS surveys • All participating public and private hospitals which provided or allowed access to their medicines procurement • Members of the NMUS Expert Panels who contributed to writing this report • Universiti Malaysia Medical Centre, Hospital Universiti Kebangsaan, Hospital Universiti Sains Malaysia, Lumut Armed Forces Hospital, Terendak Armed Forces Hospital • Association of Private Hospitals Malaysia, Malaysian Organisation of Pharmaceutical Industries (MOPI) and Pharmaceutical Association of Malaysia (PhAMA) • Malaysian Medical Council, Malaysian Medical Association, Malaysian Pharmaceutical Society, The Academy of Family Physicians, Primary Care Doctors Association Malaysia, Malaysian Dental Association, Malaysian Private Dental Practitioners Association • Pharmaniaga Logistik Sdn. Bhd. and Forte Tech Solutions Sdn. Bhd. • All who have in one way or another supported and/or contributed to the success of the NMUS and this report Mr. Mohd. Hatta bin Ahmad Chairman Dr. Lim Teck Onn Co-Chairman National Medicines Use Survey, Ministry of Health Malaysia iii ABOUT THE NATIONAL MEDICINES USE SURVEY The National Medicines Survey (NMUS) is a project initiated and supported by the Ministry of Health (MOH) to collect information on the supply, procurement, prescription, dispensing and use of drugs in Malaysia. The NMUS is designed to support the implementation of our National Medicines Policy (NMP). The objectives of NMP are to ensure only safe, efficacious and good quality medicines are available for use in Malaysia, as well as to promote equitable access to, rational and cost-effective use of these medicines, ultimately leading to improved health for all Malaysians. In supporting this, the NMUS provides the functional capacity for the collection, analysis, reporting and dissemination of data on drug utilisation in Malaysia. The NMUS is jointly sponsored by: • Pharmaceutical Services Division, Ministry of Health • Clinical Research Centre, Ministry of Health Purpose of the NMUS The availability of high quality, reliable and timely information on medicines use is crucial for any discussion on improving the use of medicines in Malaysia. The objective of the NMUS is therefore to quantify the present state and time trends of medicines utilisation at various level of our health care system, whether national, regional, local or institutional. Routinely compiled statistics on medicines utilisation have many uses, such as to: 1. Estimate the number of medicines users overall, by age, sex and geography and over time. 2. Estimate on the basis of known disease epidemiology to what extent medicines are under or over-used. 3. Describe pattern of medicines use through assessing which alternative drugs are being used for particular conditions and to what extent. 4. Relate the number of adverse drug reactions reported to our pharmacovigilance system to the number of people exposed to the drug in order to assess the magnitude of the problem, or to estimatethe degree of under-reporting of adverse events. 5. Provide a crude estimate of disease prevalence based on its prescription rate. 6. Estimate expenditure on pharmaceuticals, which constitutes a significant proportion of our healt care expenditure. 7. Monitor and evaluate the effects of interventions to improve the use of medicines. These interventions may be educational effort, promotional campaign, formulary restriction, medicines reimbursement scheme or regulatory measures. iv NMUS STEERING COMMITTEE Chairman Mr. Mohd. Hatta bin Ahmad, Deputy Director (Pharmacy Practice), Pharmaceutical Services Division, Ministry of Health Malaysia Co-Chairman Dr. Lim Teck Onn, Director, Clinical Research Centre, Ministry of Health Malaysia Members Ms. Sameerah Shaikh Abd. Rahman, Senior Principal Assistant Director, Pharmaceutical Services Division, Ministry of Health Malaysia Dr. Faridah Aryani bt. Md. Yusof, Head, Pharmaceutical Research Unit, Clinical Research Centre, Ministry of Health Malaysia Dr. Lian Lu Ming, Pharmacist Grade U52, Clinical Research Centre, Ministry of Health Malaysia Ms. Siti Fauziah bt. Abu, Senior Assistant Director, Pharmaceutical Services Division, Ministry of Health Malaysia Ms. Sarah a/p Nagalingam, Senior Assistant Director, Pharmaceutical Services Division, Ministry of Health Malaysia v NMUS PROJECT TEAM Chairman Mr. Mohd. Hatta bin Ahmad Co-Chairman Dr. Lim Teck Onn NMUS Project Staff NMUS Project Coordinator Ms. Sameerah binti Shaikh Abdul Rahman NMUS Project Manager Dr. Lim Chiao Mei Dr. Lian Lu Ming Pharmacist Liaison Officer Ms. Siti Fauziah bt. Abu Ms. Sarah Nagalingam Technical Support Staff Pharmaco-Epidemiologist Dr. Faridah Aryani bt. Md Yusof Dr. Nour Hanah bt. Othman Ms. Rosminah bt. Md Din NMUS Survey Co-ordinator Ms. Lee Kim Tin Economist Mr. Adrian Goh Statistician Dr. Hoo Ling Ping Ms. Norhafizah bt. Ab. Manan IT Manager Ms. Celine Tsai Pao Chien Database Developer/ Administrator Ms. Tang Roh Yu Ms. Lim Jie Ying Ms. Nor Afirdaus Zainal Abidin Network Administrator Kevin Ng Hong Heng Mr. Adlan Ab. Rahman Desktop Publisher Ms. Azizah Alimat Webmaster Mr. Patrick Lum See Kai vi MEMBERS OF NMUS EXPERT PANELS Expert Panel 1. Antihypertensives, Steroid & Immunosuppressive, Renal Therapeutics Members Dato Dr. Zaki Morad Mohd. Zaher (Chairperson) Dr. Lim Teck Onn Dr. Zawawi bin Nordin Dr. Hooi Lai Seong Dr. Goh Bak Leong Datin Fadilah bt. Othman Ms. Manjulaa Devi a/p Subramaniam Ms. Puteri Juanita bt. Zamri Ms. Nur Salima bt. Shamsudin Ms. Zarina bt. Abdul Ghafir Institution International Medical University Clinical Research Centre, MOH Medical Department, Sultanah Nur Zahirah Hospital, Kuala Terengganu Nephrology Dept., Sultanah Aminah Hospital, Johor Bahru Nephrology Dept., Serdang Hospital Pharmacy, Selayang Hospital Pharmacy, Kuala Lumpur Hospital Pharmacy, Selayang Hospital Pharmacy, Selayang Hospital Pharmacy, Selayang Hospital 2. Antidiabetics, Endocrine and Metabolic Therapeutics Members Dr. G.R. Letchumanan a/l Ramanathan (Chairperson) Dr. Muruga Vadivale Dr. Zanariah Hussein Dr. Sharmini Selvarajah Dr. Ariza Zakaria Ms. Cheng Mei Fen Ms. Oiyammal Chelliah Mr. Lim Kelvin Mr. Mohd. Nazri Md. Dazali Institution Medical Department, Taiping Hospital Sanofi Aventis Medical Department, Putrajaya Hospital Clinical Research Centre, MOH Clinical Research Centre, MOH Xepa-Soul Pattinson (M) Sdn. Bhd. Pharmacy, Sungai Bakap Hospital, Penang Pharmacy, Penang Hospital Pharmacy, Tampin Health Clinic 3. Antilipidaemia and Cardiovascular Therapeutics Members Dr. Chang Boon Cheng (Chairperson) Prof. Dr. Sim Kui Hian Dr. Alan Fong Yean Yip Dr. Chong Wei Peng Ms. Haarathi a/p Chandriah Ms. Nirmala a/p Jagan Ms. Yap Yih Jun Ms. Long Mei Sim Institution Cardiology Dept., Sarawak General Hospital Cardiology Dept., Sarawak General Hospital Cardiology Dept., Sarawak General Hospital University Malaya Medical Centre Pharmacy, TAR Klang Hospital Pharmacy, Kuala Lumpur Hospital Pharmacy, Kuala Lumpur Hospital Pharmacy, Selayang Hospital vii MEMBERS OF NMUS EXPERT PANELS Expert Panel 4. Antineoplastic, Oncology Members Ms. Lim Yeok Siew (Chairperson) Prof. Wan Ariffin Abdullah Dr. Gerard Lim Chin Chye Dr. Mohd. Roslan b. Haron Dr. Goh Ai Sim Ms. Yuzlina bt. Muhamad Yunus Ms. Kamarun Neasa Begam bt. Mohd. Kassim Institution Pharmacy, Kuala Lumpur Hospital Paediatric Oncology Dept., University Malaya Medical Centre Radiotherapy & Oncology Dept., Kuala Lumpur Hospital Oncology Dept., Sultan Ismail Hospital, Johor Bahru Haematology Unit, Medical Department, Pulau Pinang Hospital Pharmacy, Putrajaya Hospital Pharmacy, Kuala Lumpur Hospital 5. Antiinfectives Members Ms. Sameerah bt. S.A. Rahman (Chairperson) Dr. Ngau Yen Yew Ms. Thong Kah Shuen Ms. Masrahayu bt. Moydin Ms. Rahela bt. Ambaras Khan Ms. Jacqueline Lai Institution Pharmaceutical Services Division, MOH Medical Dept., Kuala Lumpur Hospital Pharmacy, Raja Permaisuri Bainun Hospital, Ipoh Pharmacy, Selayang Hospital Pharmaceutical Services Division, MOH Tawau Hospital, Sabah 6. Musculo-skeletal Therapeutics Members Dato’ Dr. Ramanathan a/l Ramaiah (Chairperson) Dr. Ahmad Tajuddin b. Abdullah Dr. Chew Chin Seong Dr. Ling How Tieng Ms. Aizura bt. Abdul Rahman Institution Orthopaedics Dept., Raja Permaisuri Bainun Hospital, Ipoh Orthopaedics Dept., Sultanah Nur Zahirah Hospital, Kuala Terengganu Orthopaedics Dept., Raja Permaisuri Bainun Hospital, Ipoh Orthopaedics Dept., Raja Permaisuri Bainun Hospital, Ipoh Pharmacy, Raja Permaisuri Bainun Hospital, Ipoh 7. Analgesic and Anaesthetics Members Dr. Mary S. Cardosa (Chairperson) Prof. Dr. Marzida bt. Mansor Institution Anaesthesiology Dept., Selayang Hospital University of Malaya Medical Centre viii MEMBERS OF NMUS EXPERT PANELS Expert Panel 7. Analgesic and Anaesthetics Members Clinical Assoc. Prof. Dr. Choy Yin Choy Ms. Faizah bt. Abdul Rahman Ms. Norliza bt. Mat Ariffin Institution Universiti Kebangsaan Malaysia Medical Centre Pharmacy, Selayang Hospital Pharmacy, Selayang Hospital 8. Psychiatric Therapeutics Members Dr. Siti Nor Aizah bt. Ahmad (Chairperson) Dato’ Dr. Suarn Singh a/l Jasmit Singh Dr. Ramli b. Ali Dr. Salina bt. Abdul Aziz Dr. Nor Hayati bt. Ali Ms. Mariam Bintarty bt. Rushdi Mr. Syed Fadzli b. Syed Sailuddin Ms. Noor Ratna bt. Naharuddin Ms. Shamini a/p Rama Institution Psychiatry Dept., Kuala Lumpur Hospital Bahagia Hospital, Tanjung Rambutan Psychiatry Dept., Selayang Hospital Psychiatry Dept., Kuala Lumpur Hospital Psychiatry Dept., Kajang Hospital Pharmacy, Kuala Lumpur Hospital Pharmaceutical Services Division, MOH Pharmacy, Permai Hospital, Johor Bahru Pharmacy, Bahagia Hospital, Tanjung Rambutan 9. Respiratory Therapeutics Members Datin Dr. Aziah bt. Ahmad Mahayiddin (Chairperson) Assoc. Prof. Dr. Samsinah bt. Haji Hussain Assoc. Prof. Dr. Pang Yong Kek Dr. Norhaya Mohd. Razali Dr. Mat Zuki b. Mat Jaeb Mr. Abdol Malek b. Abd. Aziz Ms. Joanne Liew Ms. Shahirah bt. Zainudi Institution Institute of Respiratory Medicine, Kuala Lumpur Hospital Dept. of Pharmacy, University Malaya University of Malaya Medical Centre Medical Dept., Sultanah Nur Zahirah Hospital, Kuala Terengganu Medical Dept., Raja Perempuan Zainab II Hospital, Kota Bharu Pharmacy, Malacca Hospital Pharmacy, Kuala Lumpur Hospital Pharmacy, Selayang Hospital 10. Gastrointestinal Therapeutics Members Dr. Jayaram Menon (Chairperson) Dato’ Dr. Muhammad Radzi b. Abu Hassan Ms. Zainon bt. Abudin Ms. Azuana bt. Ramli Institution Medical Dept., Queen Elizabeth Hospital, Sabah Sultanah Bahiyah Hospital, Alor Star Pharmacy, Selayang Hospital Pharmacy, Serdang Hospital ix MEMBERS OF NMUS EXPERT PANELS Expert Panel 11. Neurology Members Dr. Zariah bt. Abdul Aziz (Chairperson) Institution Neurology Dept., Sultanah Nur Zahirah Hospital, Kuala Terengganu Neurology Dept., Kuala Lumpur Hospital Medical Faculty, UKM Medical Centre Pharmacy, Sultanah Nur Zahirah Hospital, Kuala Terengganu Pharmacy, Kuala Lumpur Hospital Dato’ Dr. Mohd. Hanip b. Rafia Prof. Dr. Raymond Azman Ali Ms. Norhasyimah bt. Abdul Rahman Ms. Azinorwaty bt. Zakaria 12. Obstetrics & Gynaecology Members Dr. Muralitharan Ganesalingam (Chairperson) Institution Obstetrics & Gynaecology Dept., Kuala Lumpur Hospital Pharmacy, Kuala Lumpur Hospital Primary Care Doctors Organisation Malaysia Ms. Tan Ai Leen Dr. Molly Cheah 13. Otorhinolaryngology Audiology Members Dr. Saraiza bt. Abu Bakar (Chairperson) Dr. Anura Michelle Manual Institution Otorhinolaryngology Dept., Serdang Hospital Otorhinolaryngology Dept., University of Malaya Medical Centre Medical Development Division, MOH Ms. Normah bt. Mohd. Darus 14. Dermatology Members Dr. Rohna bt. Ridzwan (Chairperson) Dr. Asmah bt. Johar Dr. Roshidah bt. Baba Institution Dermatology Dept., Selayang Hospital Dermatology Dept., Kuala Lumpur Hospital Dermatology Dept., Malacca Hospital 15. Nephrology Urology Members Dr. Rohan Malek Johan Thambu (Chairperson) Dr. Clarence Lei Chang Moh Normah Dr. Suresh Sabaratnam Ms. Siti Syarihan bt. Abdullah Institution Urology Dept., Selayang Hospital Hospital, Kuching Urology Dept., Selayang Hospital Pharmacy, Selayang Hospital x MEMBERS OF NMUS EXPERT PANELS Expert Panel 16. Ophthalmology Optometry Members Dr. Bethel Livingstone (Chairperson) Dr. Goh Pik Pin Dr. C.U. Thiageswari Dr. Thayaniti a/p Sandragesu Dr. Vivian Gong Hee Ming Datin Fadilah bt. Othman Ms. Choong Chiau Ling Institution Ophthalmology Dept., Tuanku Jaafar Hospital, Seremban Ophthalmology Dept., Selayang Hospital Ophthalmology Dept., Kuala Lumpur Hospital Opthalmology Dept., Tengku Ampuan Rahimah Hospital, Klang Ophthalmology Dept., Raja Permaisuri Bainun Hospital, Ipoh Pharmacy, Selayang Hospital Pharmacy, Selayang Hospital 17. Haematology Members Ms. Lim Yeok Siew (Chairperson) Dr. Goh Ai Sim Institution Pharmacy, Kuala Lumpur Hospital Medical Dept., Pulau Pinang Hospital 18. Pharmacoeconomics Members Dr. Nour Hanah bt. Othman (Chairperson) Dr. Faridah Aryani bt. Md. Yusof Ms. Rosminah bt. Mohd. Din Ms. Fatimah bt. Abdul Rahim Ms. Nadia Fareeda bt. Muhammad Gowdh Mr. Adrian Goh Institution Pharmaceutical Services Division, MOH Clinical Research Centre, MOH Pharmaceutical Services Division, MOH Pharmaceutical Services Division, MOH Clinical Research Centre, MOH Clinical Research Centre, MOH xi CONTENTS PREFACE………………………………………………………………………………………... ACKNOWLEDGEMENTS……………………………………………………………….……. ABOUT THE NATIONAL MEDICINES USE SURVEY………………………………....…. NMUS STEERING COMMITTEE………………………………………………………...…. NMUS PROJECT TEAM………………………………………………………………...…..... MEMBERS OF NMUS EXPERT PANELS………………………………………………...… CONTENTS……………………………………………………………………………………... METHODS………………………………………………………………………………………. ABBREVIATIONS……………………………………………………………………….…….. i iii iv v vi vii xii xiii xxiii Chapter 1: Use of Medicines in Malaysia ................................................................................…............... Chapter 2: Expenditure on Medicines in Malaysia ................................................................…................. Chapter 3: Use of Medicines for Acid Related Disorders ......................................................................... Chapter 4: Use of Antiobesity Medicines …………................................................................…............... Chapter 5: Use of Antidiabetics ..............................................................................................…………… Chapter 6: Use of Antianaemic Medicines…………................................................................................... Chapter 7: Use of Antihaemorrhagic Medicines…………........................................................................... Chapter 8: Use of Medicines for Cardiovascular Disorders ..................................................................... Chapter 9: Use of Antihypertensives ......................................................................................………….… Chapter 10: Use of Lipid Lowering Medicines ........................................................................……..……. Chapter 11: Use of Dermatologicals ………….......................................................................…………… Chapter 12: Use of Gynaecologicals, Sex Hormones and Hormonal Contraceptives ...........……………. Chapter 13: Use of Urologicals ..............................................................................………………………. Chapter 14: Use of Medicines for Endocrine Disorders ............................................................………… Chapter 15: Use of Antiinfectives ...........................................................................................…................ Chapter 16: Use of Antineoplastic Agents, including Endocrine Therapy …………………..................... Chapter 17: Use of Systemic Corticosteroids and Immunosuppressive Agents......................…………… Chapter 18: Use of Medicines for Rheumatological and Bone Disorders …............................................ Chapter 19: Use of Opioid Analgesics … ………….. ..................................................…………………. Chapter 20: Use of Medicines for Neurological Disorders …….............................................…………… Chapter 21: Use of Medicines for Psychiatric Disorders .......................................................................... Chapter 22: Use of Medicines for Obstructive Airway Diseases .............................................................. Chapter 23: Use of Antihistamines & Nasal Decongesants ...……......................................……………. Chapter 24: Use of Ophthalmologicals …………..................................................................……………. Chapter 25: Use of Otologicals ...............................................................................……………………… 1 5 9 13 15 19 21 25 31 39 43 51 57 61 65 77 83 89 93 95 103 111 115 119 127 Appendix 1: Participants of the National Medicines Use Survey xii METHODS Authors: Lian LM1, Lim CM1, Tang RY2, Lim JY2, Hoo LP3, Faridah AMY1, Goh A, Lim TO1 1. Clinical Research Centre MOH, 2. Datamed Sdn. Bhd., 3. Clin Research Sdn. Bhd. Introduction The NMUS is designed, broadly speaking, to estimate the quantity and pattern of use of medicines in Malaysia, as well as to estimate our expenditure on pharmaceutical. This is an ambitious project, which requires multiple surveys at the various levels of the medicines supply and distribution chain in the country (Figure 1) in order to capture all the required data to meet its purpose. Clearly, all these could not be accomplished overnight, and of necessity must be undertaken in phases. We had realistically targeted data sources that are absolutely critical and/ or accessible initially, while piloting less accessible ones, and leaving the most inaccessible data sources for the future, hoping to build on the foundation laid by earlier surveys as well as to capitalise on early successes. Fig. 1 Medicines supply & distribution system and Sources of data Manufacturer/Importer Distributor/Wholesaler Primary care/GP Hospital Pharmacy Consumer/Patients 12 Hence, the statistics on medicines use and expenditure in this report are estimated from data from only a limited number of surveys (though they were the critical ones) that could be successfully completed nation-wide or on a more local pilot basis. The scope was also deliberately limited to prescription only medicines (obviously the pharmaceuticals of greatest interest) and excludes Over-the-Counter (OTC) medicines, traditional or herbal products and food supplements. No doubt, the NMUS will mature over time as coverage of existing nation-wide surveys broaden, local pilot surveys are rolled out nation-wide, and presently less accessible data sources become available. Over time, we should be able to provide more accurate and reliable estimates, as well as more informative and detailed analyses. xiii NMUS Surveys The NMUS conducts several surveys in order to capture data at the various levels of the medicines supply and distribution system in the country. The sources of data, surveys to collect the data, data availability, comments on data inclusion in this report are summarised in the table below. # 1.0 1.1 1.2 2.0 2.1 3.0 3.1 3.2 3.3 3.4 3.5 4.0 4.1 4.2 4.3 4.4 5.0 5.1 5.2 6.0 6.1 Data sources and Surveys Year data available Medicines import or production data Medicines import data from Royal Malaysian Customs Local pharmaceutical manufacture Domestic sales data Domestic sales data from local pharmaceutical companies Medicines pr ocurement data Public hospitals medicines procurement data from several sources: a. MOH procurement through central tender (APPL) b. MOH individual hospital local purchase (NonAPPL) c. University and Armed Forces ho spitals procurement Private hospitals procurement Private GPs procurement Private specialist practice procurement Private pharmacies procurement Medicines prescription data Public (MOH) primary care practice prescription Private GP prescription Private specialist practice prescription of highly specialised medicines. Pilot survey limited to Nephrology practices and dialysis facilities only Hospital practice prescription Medicines dispensing data Public hospital pharmacy dispensing Private free -standing pharmacy dispensing Household medicines consumption data Household survey on medicines consumption xiv Inclusion in present report 2004, 2005, 2006 Data not collected No No Data not collected No 2001 to 2006 2001 to 2006 2004, 2005, 2006 2000 to 2006 Data not collected Data not collected Data not collected Yes Yes Yes Yes No No No Limited availability 2005, 2006 Data not collected No Yes No 2001-2004 No Data not collected No Data not collect ed 2005, 2006 Not done No Yes No Thus, the statistics presented in this report are derived from only a limited number of data sources. As shown above: • Of the 6 theoretical data sources, NMUS primarily targeted data sources on hospital medicines procurement and prescription/dispensing. • Collection of prescription data is limited to general clinic practices, while hospital prescription is assumed to be included in hospital procurement data. • Similarly, hospital dispensing data are assumed to be included in hospital procurement data, except of course for private free-standing pharmacies. Dispensing survey is therefore limited to the latter only. Given that private medical practitioners in Malaysia retain dispensing rights, prescription is a far more important source of data than dispensing, unlike say in Australia. • Many private medical specialists may self-procure and dispense, rather than use hospital pharmacy dispensing service. Thus, in so far that prescription of highly specialised medicines for a particular condition is concentrated in private ambulatory specialist practices (which are unlikely as most such drugs are probably prescribed in hospital setting), they will be under-estimated in this report. Separate procurement and prescription surveys on such highly specialised medicines (if any) are required. • It is well known that consumers do access medicines through both formal as well as informal channels. Household survey will be required to obtain information on such use of medicine in the community. • Finally, medicines import and sales data from pharmaceutical companies, where available, are not used for statistical estimation, but are used for reference only, and for cross-checking the reliability of results estimated from the other data sources. Survey population, sampling and response or coverage rate The surveys conducted by NMUS 2006, its survey population and sampling unit, sample size and the survey response or coverage rates are summarized in the table below. # Surveys 1. MOH Pharmaceutical procurement Private hospitals pharmaceutical procurement University and Armed Forces hospitals pharmaceutical procurement Private GP prescription Private pharmacy dispensing 2. 3. 4. 5. Survey population and sampling unit 133 MOH hos pitals i. APPL ii. Non APPL 114 Private hospitals Sample size Coverage or response rate, and completeness 133 99 34 100% for APPL 75% for NonAPPL 30 % 3 University hospitals 2 Armed Forces h ospitals 1 University 2 Armed Forces 67% for University 100% for Armed Forces 4459 599 13 % 466 23 5% xv Data collection The surveys conducted by NMUS collected data either by 1. Download from existing databases 2. Primary data collection These are described below. # 1. Surveys MOH Pharmaceutical procurement 2. 4. Private hospitals’ pharmaceutical procurement University and Armed Forces hospitals pharmaceutical procurement Private GP prescription 5. Private Pharmacy dispensing 3. Data download from existing databases Pharmaniaga pharmaceutical procurement databases, central database as well as individual hospitals’ local purchase databases. Individual hospitals’ pharmaceutical procurement databases Individual hospitals’ pharmaceutical procurement databases A sample of GPs collected prescription data in a randomly selected week. The sample being distributed over 3 four - monthly cycle A sample of pharmacies with resident pharmacist collected dispensing data in a randomly selected week. The sample being distributed over 3 four - monthly cycle Data management The collected data, whether in databases or in paper or electronic data collection form, is compiled into a single database, appropriately processed and coded prior to statistical analysis. The NMUS database was created in Ms SQL Server 2000. The application has 3 modules: Contact Management, Data Entry and Data Processing. • Contact Management module is used to collect the establishments’ survey details, log and track all the corespondence documents with SDP, and forecast, plan and schedule the conduct of the survey. • Data Entry module is used to collect the data submitted by the SDP in paper form. It has been designed to collect data from GP prescription survey and pharmacy dispensing survey using paper CRF or prescription booklets. • Data Processing module is used to clean, manage and process the medicines data prior to statistical analysis. The automated data processing functionalities include ATC coding, DDD Assignment, Total Dosage Calculation and Unit Conversions. The database server is running on Windows 2000 Server. The server environment is Intel Xeon 2.4 Mhz, with a total of 2GB RAM memory and 67.8GP Raid5 Hard disk. xvi The data processing steps are as follows: # 1. 2. 3. 4. 5. # 1. 2. 3. 4. Data processing for downloaded database Data were downloaded from the existing database of the following data sources MOH APPL Procurement MOH Non - APPL Procurement Private Hospital Procurement University Hospital Procurement Armed Forces Hospital Procurement GP Prescription Private Pharmacy Dispensing The data downloaded could be in flat file format, e.g. TXT/XLS and etc, or database files such as Access/Oracle/SQL and etc. The structure of each of the downloaded database/data file would be studied and analysed to identify the required data fields/variables. The required variables are registration number, drug description, packaging description, supplier name, value procured, quantity procured, year procured and etc. Next, the required fields/variables would be extracted using SQL queries. The extracted data would then be normalised by separating into multiple, related tables in a single compiled database. Some of the data would require aggregation, e.g. total a few transactions on the same drug into 1 record, to speed up subsequent query performance The data would then be linked to the respective SDP in the main contact table. Data processing for primary survey data Data entry Data is entered into the Data Entry module of the database. Prior to data entry, data entry personnel are briefed on how to use the application and enter the data. Necessary precautions were given verbally, for example, to check each clinic by office id and name, as they are clinics with many branches of the same name. A demonstration was done on data entry during the briefing. Personnel were supervised while doing the first few entries to make sure they know how to do it correctly. A standard document on steps/precautions for data entry would be mailed to each personnel. They are also given a softcopy of the list of pharmaceutical products (scheduled poison and non-scheduled poison) obtained from National Pharmaceutical Control Bureau, to cross check the spelling of drugs when the writing is less legible. Edit checks Survey forms are cross - checked against the database. Selection of survey form is by data entry personnel, randomly by survey date. If number of drug entries for selected date is not sufficient, more survey dates are included. Items to check: Number of patients are same in survey form and database Number of drug entry/drug prescribed is same in survey form and database. Age, sex of patient is entered correctly. Drug particulars are entered correctly. Calculations and Derived variables Dose per day is obtained by Dosage* frequency Dose per visit is obtained by Dosage* frequency * duration Visual review and manual assessment of entries if there are misspellings. xvii # 1. 2. Common data processing steps Registered Product List An estimated 7000 ‘scheduled poison’ products registered with Drug Control Authority were manually coded to ATC INN (Level 5). The coded Drug Control Authority drug list would serve as an internal drug dictionary for medicines data coding later. Data Parsing by programming The variables ‘Drug description’ and ‘Packaging Description’ in medicines (procurement/prescription/dispensing) data are parsed into smaller parts using specially written computer program. Parsing facilitates the auto-coding process and dosage calculation later. The variable ‘Drug description’ will be parsed into ‘Brand’, ‘INN’, ‘Dosage’, ‘Unit’ and ‘Route’ e.g. Zocor Tab 80 mg Brand – Zocor INN – none Dosage – 80 Unit – mg Route – Tab The variable ‘Packaging Description’ will be parsed into ‘Big Unit’, ‘Small Unit’ and ‘Factor’ e.g. Pack of 10 tabs Big Unit – Pack Small Unit – tabs Factor – 10 3. 4. 5. 6. ATC Coding The parsed ‘Brand’ would then be linked to the coded registered drug list to obtain the ATC INN and DDD. However, if a certain brand has more than 1 DDD, the administration route has to be considered when assigning the DDD. On the other hand, the parsed ‘INN’ would be linked to the ATC Level 5 to obtain the INN and DDD. Similarly, if a certain INN has more than 1 DDD, the administration route has to be considered when assigning the DDD. Visual review and manual coding of residual medicines data to ATC; most of these residual data are due to incomplete or inconsistent data. Drug Description Dosage and Unit The Drug Description Dosage and Unit would be the parsed ‘Dosage’ and ‘Unit’ unless more than 1 dosage exists, e.g. 2MG/ML 100ML. This kind of data would require further processing. The results of this step are ‘Total Drug Description Dosage’ and ‘Total Drug Description Unit’. Remaining residual has been handled manually. Packaging Description Dosage The packaging description dosage would be taking the parsed ‘Factor’ and calculated with reference to the ‘SKU’ or ‘UOM’. The result of this step is the ‘Total Packaging Description Dosage’. Remaining residual has been handled manually. Total Dosage Calculation Total Dosage = Total Drug Description Dosage* Total Packaging Description Dosage* Quantity procured. Total Dosage Unit = Total Drug Description Unit. xviii Statistical report This statistics on use of medicines in this report are presented using the Anatomical Therapeutic Chemical (ATC) classification system, and the unit of measurement is expressed in Defined Daily Dose (DDD). This is recommended by the WHO to be used for drug utilisation research and for purpose of comparisons of drug consumption statistics between countries, between regions or population groups within country and to evaluate trends in drug use over time. Structure of the ATC Classification system In this system, medicines are divided into different groups according to the organ or system on which they act, and on their chemical, pharmacological and therapeutic properties. Medicines are classified in groups at 5 different levels as follows: Level 1 2 3 4 5 Group and subgroups Anatomical main group. There are 14 of these, eg C cardiovascular, M musculo-skeletal, R respiratory, etc Therapeutic main group Therapeutic subgroup Chemical or Therapeutic subgroup Drug chemical substance An example should make this clear. Simvastatin is coded C10AA01. The structure of its code is as follows: Level 1 2 3 4 5 Code C C10 C10A C10AA C10AA01 Group and subgroups Cardiovascular system Serum lipid reducing agents Cholesterol or triglyceride reducers HMG CoA reductase inhibitors Simvastatin Refer to the publication Guidelines for ATC Classification and DDD Assignment (WHO Collaborating Centre for Drug Statistics Methodology 2003; www.whocc.no) for details. Concept of the Defined Daily Dose (DDD) The measurement unit for medicines use adopted in this report is the DDD. The DDD is the assumed average maintenance dose per day for a drug used for its main indication in adults. The DDD is simply a technical measure of drug utilisation; it does not necessarily agree with the recommended or prescribed daily dose. Doses for individual patients and patient groups will often differ from the DDD. The DDD is often a compromise based on review of the available information about doses used in various countries. The DDD may even be a dose rarely prescribed because it is an average of two or more commonly used doses. Medicines use statistics in this report are presented for most drugs as numbers of DDDs per 1000 inhabitants per day. Some interpretative notes are as follows: • The DDDs/1000 inhabitants/day provides a rough estimate of the proportion of population treated daily with certain drugs. For example, the figure 10 DDDs/1000 inhabitants/day indicates that 1% (10/1000) of the population on average might get a certain drug or group of drugs every day in the year. • The DDDs/1000 inhabitants/day is most useful for drugs used in the treatment of chronic diseases and especially when there is a good agreement between the average prescribed daily dose and the DDD. • For most drugs, their DDDs/1000 inhabitants/day are calculated for the total population including all age and sex groups. Where a drug use is limited to particular age or sex groups, then it will be more meaningful to express the figure for the relevant age-sex groups only. For example DDDs/1000 children age<12/day, or DDDs/1000 women in reproductive age groups/day. xix For anti-infectives (or other drugs normally used in short duration), the medicine use statistics are presented as DDD per inhabitant per year. This gives an estimate of the number of days for which each inhabitant is, on average, treated annually. For example, 5 DDDs/inhabitant/year indicates that the utilisation is equivalent to the treatment of every inhabitant with a 5-days course in the year. In interpreting drug utilisation statistics using DDD, as in this report, readers are cautioned to bear in mind the following limitations: • A medicine may have several indications while the DDD is based on the main indication in adults. • Medicines procured, prescribed or dispensed, as presented here, may not necessarily be consumed. • DDD may be difficult to assign or not assigned at all for certain medicines, for example medicines with multiple ingredients, topical products, anti-neoplastic drugs and anaesthetic agents. • Medicines newly introduced into the market may yet have ATC and DDD assigned to it. • The DDD assigned to a drug is primarily based on other countries’ experience and may not reflect the commonly prescribed adult dose in Malaysia. Statistical Methods In NMUS report, the quantity of use of a medicine is expressed as, depending on the type of medicine, the number of DDDs per 1000 inhabitants per day or DDDs per inhabitants per year. These statistics are calculated as follows: DDDs/1000 inhabitants/year = DDDs/1000 inhabitants/year = Tˆ *1000 DDD * P *365 Tˆ *1000 ddd * P Where Tˆ is an estimate of the total quantity of the drug utilised in the year under consideration, DDD is the DDD assigned for the drug according to the ATC/DDD system, P is the mid-year population of Malaysia, 365 refers to the 365 days in a year In either case, an estimate of the total quantity of the drug being utilised in the year is required, and this must be expressed in the same unit as the DDD assigned for the drug. The statistical estimation of the totals varies depending on the survey method and the sampling design employed to collect the data, and if necessary with adjustment for incomplete data. These are described below. # 1 Surveys MOH Pharmaceutical procurement: APPL Estimation procedure No sampling was employed in the survey due to full response.Therefore the total is the sum of all the quantities of the drug procured in all procurement records in the year. The total is Tˆ = I ∑T i i =1 where T i is the value of the quantity of drug procured of the ith hospital in the year. 2. i) MOH Pharmaceutical procurement: Non APPL Data were available for only a sample of hospitals. The total is estimated by Tˆ = Ij 4 ∑∑ w T j i i =1 j =1 xx # Surveys Estimation procedure (# '#$%) # #$ $!%$ Ti $%'& %"&%%) #&!# &# %i% $!% !#&% %)# !# &#% j$%#% #% $%#% % $!% j$%#% #'% $!%$ j$%#% !#&% j $%#% !# &#% j$%#% $!(% $%#% Bj wj = bj j Bj$% %&# $ # $!%$% ! !&% bj $% %&# $%$! #$%#%j #'%- !#$#!% #'%!#) $!$ ,%(# % ) #$! - #!#) # #$! %% % ) #$! )$ )#*( #.)$ ) % %$$%%) T/ = I + ∑∑ w T i ij i = j = (# Tij $%'& %"&%%) #&!#$#)%it- # !#) %j%) $!(% %i%- #!#) N D wi = × n di (#N$% %&# - #!#)%! !&% n$ &# #$! - #!#)*$!D $%% % &# ( #.)$)# d i $%&# $&#'))$ i%- #!#))# Where there is sampling or where response rate of the survey was less than 100%, the procedures described above incorporate the sampling weight of the sampling unit in the estimation of total. xxi The sampling weight for each sampling unit or unit of analysis has the following components: 1. Probability of selection. The basic weight is obtained by multiplying the reciprocals of the probability of selection at each step of sampling design. Example, for GP prescription survey, this is GP practice and prescription day. 2. Adjustment for non-response. The response rate was less than 100% for some surveys; an adjustment to the sampling weight is required. The non-response adjustment weight is a ratio with the number of units in the population as the numerator and the number of responding sampling units as the denominator. The adjustment reduces the bias in an estimate to the extent that non-responding units have same characteristics as responding units. Where this is unlikely, some adjustments took into account differences in some relevant characteristics between responding and non-responding units that may influence drug utilisation, such as bed strength, staff strength, scope of services for hospitals etc. Expenditure estimation methodology Study Population The MSOM encompasses private & public healthcare providers in Malaysia consisting of 1. The public health sector which consists of hospitals and primary care clinics of the Ministry of Health, University Hospitals under the Ministry of Higher Education and Military Hospitals under the Ministry of Defence. 2. The Private health sector consisting of private hospitals and general practitioners in Malaysia. 3. Private sector retail pharmacies. Methodology The expenditure on a particular drug in a given year is the quantity of drug used in that year multiplied by the price of the drug. Total expenditure = Quantity of drug utilisation * Price of drug. Quantity of drug utilisation is determined from the drug utilisation data presented elsewhere in this report. Median prices were determined for each drug chemical substance (5th level ATC classification) and denominated in Daily Defined Doses (DDD) for the public and private sectors taking into account the availability of price data and analytical considerations. Thus there are two prices (i.e. public sector and private sector median price) for each drug chemical substance. The expenditure for each procurement item is then calculated as Ei = p50i * DDDi where p50 is the median price, DDD is the quantity of utilisation and “i” refers to the drug chemical substance. The total expenditure on a drug chemical substance in a particular sector is the sum of all procurement, prescription and dispensing of the item items in that sector. The total expenditure for the country is the sum of total expenditure in all the sectors. Prices were determined for the public sector from procurement data of MOH, University and Armed Forces health establishments surveyed by NMUS while private sector prices were determined from procurement data of private hospitals surveyed by NMUS. As the GP prescription & retail pharmacy dispensing data obtained by NMUS did not contain any data usable for calculating prices, the prices estimated from private hospitals were applied to GP and Pharmacy data as well. xxii ABBREVIATIONS ACEI AF APPL ARB ASR ATC BCF BPFK CCB CCF COAD CPG CTZ DALYs DDD Dept FDA GERD GP HCTZ HDL HMG CoA H2RA ICU INN ISAAC KL LDL LMWH MOH NCC NCI NMP NMUS NPCB NSAIDs OTC PCDOM PPI RE SDP SERM SKU SSRI UOM URTI WHO WP Angiotensin Converting Enzyme Inhibitors Atrial Fibrillation Approved Product Price List Angiotensin II Antagonists/Angiotensin Receptor Blocker Age Standardized Rate Anatomical Therapeutic Chemical Bias Correction Factor Biro Pengawalan Farmaseutikal Kebangsaan Calcium Channel Blockers Congestive Cardiac Failure Chronic Obstructive Airway Disease Clinical Practice Guidelines Chlorothiazide Disability Life Years Defined Daily Dose Department Food And Drug Administration Gastroesophageal Reflux Disease General Practitioner Hydrochlorothiazide High Density Lipoprotein 3-hydroxy-3-methylglutaryl coenzyme A H2 Receptor Antagonist Intensive Care Unit International Nonproprietary Name International Study of Asthma and Allergies in Childhood Kuala Lumpur Lipoprotein Levels Low Molecular Weight Heparin Ministry of Health National Cancer Centre National Cancer Institute National Medicines Policy National Medicines Use Survey National Pharmaceutical Control Bureau Non Steroidal Anti- Inflammatory Drugs Over-the-Counter Primary Care Doctors Organisation Malaysia Proton Pump Inhibitors Reflux Esophagitis Source Data Producer Selective Estrogen Receptor Modulator Stock Keeping Unit Serotonin Selective Reuptake Inhibitor Unit of Measurement Upper Respiratory Tract Infection World Health Organisation Wilayah Persekutuan xxiii CHAPTER 1 USE OF MEDICINES MALAYSIA Malaysian Statistics on Medicines 2006 Edited by: Lim TO1, Nadia Fareeda MG1, Lian LM1, Sameerah SAR2, Mohd. Hatta A2, Faridah AMY1 1. Clinical Research Centre MOH 2. Pharmaceutical Services Division MOH In this chapter, we report an overview of the national estimates for the use of medicines in Malaysia. It describes the most commonly used medicines by therapeutic groups and by specific drugs. The scope of the National Medicines Use Survey (NMUS) was deliberately limited to prescription medicines only and excluded Over-the-Counter (OTC) medicines, traditional or herbal products and food supplements. Generally, the measurement unit for medicines use adopted in this report is the DDD [1] which is the assumed average maintenance dose per day for a drug used for its main indication in adults. The DDD is simply a technical measure of drug utilisation; it does not necessarily agree with the recommended or prescribed daily dose. In this chapter, the utilisation data are presented only for drugs that have assigned DDDs, and the estimates are expressed as number of DDDs per 1000 population per day; medicines without DDDs are excluded. However, in other chapters of this publication, utilisation of some medicines of interest that do not have DDDs are also discussed. In those chapters, the statistics are presented in terms of weight of active ingredient/1000 population per day (Anti-neoplastic drugs), or weight or volume of drug preparations per 1000 population per day (Dermatologicals, Ophthalmologicals and Otologicals). Among the therapeutic groups, drugs used in diabetes (A10) ranked highest in terms of utilisation in Malaysia for the year 2006 (Table 1.1). An estimated 4.0% of the Malaysian population was on this group of drugs in 2006 of which glibenclamide (1.6% of the population) and metformin (1.3% of population) were most used. Other commonly used diabetic drugs include gliclazide and Insulins and analogues, intermediate-acting combined with fast-acting (human) with each ranking 9th and 37th among the top 40 drugs by utilisation. The utilisation of these drugs was heavily skewed towards the public sector with utilisation of more than four times that of the private sector, suggesting an imbalance in the disease burden borne. (Table 1.2) Of the top 40 drugs listed by utilisation, 18 were drugs used for cardiovascular diseases (ATC group C and acetylsalicylic acid B01A C06). Drugs used for the treatment of hypertension were among the highest in terms of utilisation. Collectively 6.8% of the population were on at least one of these drugs which include beta-blocking agents (2.6% of population), calcium channel blockers (1.9% of population)), agents acting on the renin-angiotensin system (2% of population) and antihypertensives (0.3% of population). Prevalence of hypertension among Malaysians aged 30 years and above in 2006 was estimated to be 42.6% and among them only 31.4% were on current treatment [2]. A study conducted by Rampal et al in 2004 estimated that only 34.6% of the study participants with hypertension were aware of their condition and on pharmacotherapy, and of these only 26.6% had adequate blood pressure control [3]. Although utilisation of medicines for the treatment of hypertension seemed high, poor awareness and under treatment of this disease are issues that need to be addressed. (Table 1.2) Lipid modifying agents ranked 5th for therapeutic groups by utilisation, with 1.7% of the population prescribed these drugs. Simvastatin, lovastatin and atorvastatin constituted 41%, 30% and 18% of the total use respectively. Utilisation of lovastatin was approximately 8 times more in the public sector compared to the private sector, and conversely the use of atorvastatin in the private sector was more than twice the utilisation in the public sector. This suggested a difference in prescribing preference and trend between these parallel healthcare providers in the country which was very much influenced by cost. Australian data showed that atorvastatin was the most used lipid modifying agent compared to simvastatin and lovastatin. Atorvastatin was the top drug ranked by DDD whereas simvastatin ranked 2nd and lovastatin was not among the top 10 [4]. Given the expected trends of increasing serum cholesterol and coronary heart disease in most Asian countries, utilisation of this group of drugs are expected to increase in the future [5]. 1 CHAPTER 1 USE OF MEDICINES MALAYSIA Malaysian Statistics on Medicines 2006 Drugs used for obstructive airway diseases (R03) ranked 6th by utilisation with inhaled salbutamol (R03AC02) being the commonest drug used (0.4% of population). Chlorpheniramine and prednisolone were clearly drugs of choice as their utilisation were highest in their groups, antihistamines for systemic use (R02) and steroids for systemic use (H02) respectively. Among the antiinflammatory and antirheumatic products (M01), utilisation of diclofenac (M01A B05) was highest (0.4% of population). Interestingly, although the prevalence of psychiatric morbidity estimated by NHMS III was 11.2%, psycholeptics (N05) and psychoanaleptics (N06) only ranked 15th and 20th among therapeutic groups listed by utilisation and none of the individual drugs in the N05 or N06 groups were in the top 40 drugs listed by utilisation. Detailed discussions on the specific therapeutic groups can be found in the respective chapters. The NMUS, amongst other objectives, is designed to support the implementation of the National Medicines Policy. Hence it is pertinent to note that 36 (90%) of the top 40 most utilised drugs were in the Malaysian National Essential Drugs List (NEDL) [5]. Of these 36 drugs, 6 of them were listed under the NEDL Supplementary List, which lists drugs that are designated as those used by specialists for tertiary level treatment. This indicated good accessibility to essential drugs generally, with reasonable availability and utilisation of higher-end drugs for specialists care. Of the four drugs in the top 40 which were not in the NEDL, two of them were the statins i.e. Lovastatin (C10A A02) and Atorvastatin (C10A A05), and the other two being Cetirizine (R06A E07), an antihistamine, and Losartan (C09C A01), a cardiovascular drug acting on the renin-angiotensin system. There are alternative drugs from the NEDL which are in the top 40 for these groups of drugs, and it may be interesting to study in greater detail the utilisation of these four drugs compared to their corresponding alternatives listed in the NEDL. Table 1.1: Top 30 Therapeutic groups by Utilisation in DDD/1000 population/day 2006 NO. ATC THERAPEUTIC GROUP PUBLIC PRIVATE TOTAL 1 2 3 A10 C07 C09 32.792 21.3322 13.8264 7.5037 4.4021 5.7554 40.2957 25.7343 19.5818 4 5 C08 C10 DRUGS USED IN DIABETES BETA BLOCKING AGENTS AGENTS ACTING ON THE RENIN-ANGIOTENSIN SYSTEM CALCIUM CHANNEL BLOCKERS LIPID MODIFYING AGENTS 15.941 8.639 3.4246 8.5206 19.3656 17.1599 6 R03 DRUGS FOR OBSTRUCTIVE AIRWAY DISEASES 9.8198 6.6997 16.5194 7 8 9 C03 R06 M01 11.775 5.1758 3.9519 2.8894 6.9945 6.0516 14.6643 12.1703 10.0035 10 11 12 13 14 15 16 17 18 19 20 B01 J01 A02 C01 H02 N05 C02 H03 M04 N03 N06 DIURETICS ANTIHISTAMINES FOR SYSTEMIC USE ANTIINFLAMMATORY AND ANTIRHEUMATIC PRODUCTS ANTITHROMBOTIC AGENTS ANTIBACTERIALS FOR SYSTEMIC USE DRUGS FOR ACID RELATED DISORDERS CARDIAC THERAPY CORTICOSTEROIDS FOR SYSTEMIC USE PSYCHOLEPTICS ANTIHYPERTENSIVES THYROID THERAPY ANTIGOUT PREPARATIONS ANTIEPILEPTICS PSYCHOANALEPTICS 5.8947 3.8147 2.5009 2.7994 1.9061 3.0503 2.9987 1.4486 1.0294 1.3457 0.8941 3.9402 5.1222 2.656 1.8969 2.5407 0.9951 0.2328 0.5478 0.5053 0.1535 0.4223 9.835 8.9369 5.1568 4.6961 4.4467 4.0454 3.2315 1.9964 1.5347 1.4992 1.3163 2 CHAPTER 1 USE OF MEDICINES MALAYSIA Malaysian Statistics on Medicines 2006 NO. ATC THERAPEUTIC GROUP PUBLIC PRIVATE TOTAL 21 22 23 24 25 26 27 28 29 30 J04 N07 N04 N02 M03 J05 M05 J02 L02 P01 ANTIMYCOBACTERIALS OTHER NERVOUS SYSTEM DRUGS ANTI-PARKINSON DRUGS ANALGESICS MUSCLE RELAXANTS ANTIVIRALS FOR SYSTEMIC USE DRUGS FOR TREATMENT OF BONE DISEASES ANTIMYCOTICS FOR SYSTEMIC USE ENDOCRINE THERAPY ANTIPROTOZOALS 0.9993 0.4341 0.8293 0.382 0.0658 0.495 0.2633 0.0519 0.1937 0.1787 0.0997 0.6421 0.0527 0.4137 0.5474 0.0688 0.1767 0.2735 0.0906 0.1013 1.099 1.0762 0.882 0.7957 0.6131 0.5638 0.4399 0.3253 0.2844 0.28 Table 1.2: Top 40 Drugs by Utilisation in DDD/1000 population/day 2006 NO. ATC THERAPEUTIC GROUP PUBLIC PRIVATE TOTAL 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 A10B B01 A10B A02 C07A B02 C07A B03 C08C A05 B01A C06 C10A A01 C03A A04 A10B B09 C08C A01 C03C A01 C09A A04 C10A A02 C09A A02 R03A C02 C09A A01 R06A B04 M01A B05 C10A A05 R03C C03 M01A G01 H02A B06 R03C C02 C02C A01 R06A X13 J01C A04 C08C A02 R03B A02 R06A E07 A02B A02 R03D A04 A02B C01 C01E B15 R06A B02 C01D A08 C03A A03 Glibenclamide Metformin Metoprolol Atenolol Nifedipine Acetylsalicylic acid Simvastatin Chlorothiazide Gliclazide Amlodipine Furosemide Perindopril Lovastatin Enalapril Salbutamol Captopril Chlorpheniramine Diclofenac Atorvastatin Terbutaline Mefenamic acid Prednisolone Salbutamol Prazosin Loratadine Amoxicillin Felodipine Budesonide Cetirizine Ranitidine Theophylline Omeprazole Trimetazidine Dexchlorpheniramine Isosorbide dinitrate Hydrochlorothiazide and potassium-sparing agents 14.0329 11.1397 11.7536 9.077 10.9355 4.8358 2.6378 6.2441 4.593 3.2803 3.9301 4.3301 4.0507 3.5113 4.024 4.1067 2.5619 1.4652 0.786 0.1697 1.2609 1.1766 0.6566 2.234 0.7417 0.698 1.3805 1.5432 0.2259 1.1741 1.1004 0.5889 0.6345 0.0486 1.2768 1.0077 1.5023 2.0109 0.5828 2.9516 0.6772 2.5826 3.9287 0.0355 1.3678 1.9924 0.9588 0.3811 0.5157 0.9827 0.3237 0.1984 1.3908 2.1248 2.537 2.8792 0.284 1.3428 1.8439 0.0961 1.436 1.4018 0.4422 0.1962 1.5065 0.539 0.4886 0.9111 0.804 1.3559 0.0932 0.3358 15.5352 13.1506 12.3365 12.0287 11.6127 7.4184 6.5665 6.2796 5.9608 5.2728 4.8889 4.7113 4.5664 4.4939 4.3477 4.3051 3.9527 3.59 3.323 3.049 1.545 2.5194 2.5005 2.3301 2.1777 2.0998 1.8227 1.7393 1.7324 1.7131 1.589 1.5 1.4386 1.4045 1.3699 1.3434 3 CHAPTER 1 USE OF MEDICINES MALAYSIA Malaysian Statistics on Medicines 2006 NO. ATC THERAPEUTIC GROUP PUBLIC PRIVATE TOTAL 37 A10A D01 1.1299 0.1955 1.3255 38 39 40 M04A A01 R06A D02 C09C A01 Insulins and analogues, intermediate-acting combined with fast-acting (human) Allopurinol Promethazine Losartan 0.9627 0.8492 0.5202 0.3601 0.4305 0.5978 1.3277 1.2797 1.1179 References: 1. Complete ATC/DDD Index and Guidelines for ATC Classification and DDD Assignment (WHO Collaborating Centre for Drug Statistics Methodology 2007; www.whocc.no) 2. Institute of Public Health (IPH) 2008. The Third National Health and Morbidity Survey (NHMS III) 2006, Vol 1. Ministry of Health, Malaysia. 3. L Rampal, S Rampal, MZ Azhar, AR Rahman. Prevalence, awareness, treatment and control of hypertension in Malaysia: A national study of 16 440 subjects. Public Health. 2008 Jan; 122 (1):11-18; 4. Commonwealth of Australia 2008. Australian Statistics on Medicines 2006 Online ISBN: 1-74186-516-6 Available from http://www.health.gov.au/internet/main/ publishing.nsf/Content/health-pbsgeneral-pubs asm.htm 5. Khoo KL, Tan H, Liew YM, Deslypere JP, Janus E. Lipids and coronary heart disease in Asia. Atherosclerosis. 2003 Jul; 169(1):1-10; 6. The National Essential Drug List (Malaysian) (http://www.pharmacy.gov.my/html/pharma_care_nedl_f.htm as at 18 March 2009) 4 CHAPTER 2 EXPENDITURE ON MEDICINES IN MALAYSIA Malaysian Statistics on Medicines 2006 Edited by: Faridah AMY1, Nour Hanah O2, Rosminah MD2, Fatimah AR2, Nadia Fareeda MG1, Goh A3 1. Clinical Research Centre MOH, 2. Pharmaceutical Services Division, MOH, 3. ClinResearch Sdn. Bhd. In this section we looked at the estimated drug expenditure in Malaysia in 2006. As expected, the highest expenditure recorded that year was for amlodipine (C08C C01). This drug was also among the top 10 drugs utilised in 2006, reflecting the high prevalence of hypertension in the Malaysian population (42.6% for adults aged 30 years and above). The highest expenditure incurred in the public and private sectors were for metoprolol (C07A B02) and atorvastatin (C10A A05) respectively. The pattern of drug expenditure differed between the public and private sectors as shown in Table 2.1 and Table 2.3. Private sector expenditure was inclined towards newer and therefore more costly drugs, such as atorvastatin and clopidogrel (B01A C04). When compared by therapeutic groups, the highest expenditure was incurred for drugs used in diabetes (A10) as shown in Table 2.2. This correlated to the high prevalence of diabetes mellitus in the country (14.9% for adults aged 30 years and above). When compared by sector, the public sector expenditure was concentrated on drugs used in diabetes whereas lipid modifying agents (C10) topped the list for the private sector as shown in Table 2.4. Looking at the Australian expenditure statistics for 2006, atorvastatin, simvastatin (C10A A01) and esomeprazole (A02B C05) were the top 3 drugs by expenditure as shown in Table 2.3 with lipid modifying agents being the highest expenditure therapeutic group as shown in Table 2.4. The analysis in this chapter was conducted on the top 150 drugs by utilisation only. Therefore drugs that were costly but very low in utilisation were not included in the analysis. Certain drugs under the antineoplastic and immuno modulating agents’ anatomical main group (L) may have appeared in the top 50 by expenditure if the group was included. Table 2.1: Top 50 Drugs by Expenditure in RM ‘000 Rank ATC Drugs Public Private Total 1 C08C A01 Amlodipine 20,870 9,913 30,783 2 C10A A05 Atorvastatin 6,691 19,876 26,568 3 C07A B02 Metoprolol 22,406 2,676 25,082 4 C10A A01 Simvastatin 7,143 14,647 21,790 5 J01D C02 Cefuroxime 13,910 7,654 21,564 6 A10B A02 Metformin 14,558 6,091 20,649 7 A10B B09 Gliclazide 12,636 6,790 19,426 8 N05A X08 Risperidone 18,622 190 18,812 9 C07A B03 Atenolol 7,785 10,683 18,468 10 C09A A01 Captopril 11 C09A A02 Enalapril 17,010 1,120 18,130 12 B01A C04 Clopidogrel 15,455 2,277 17,732 13 B03X A01 Erythropoietin 2,288 14,374 16,662 14 J01C R02 Amoxicillin and enzyme inhibitor 9,347 6,331 15,678 15 M01A B05 Diclofenac 5,755 9,459 15,214 16 A02B C01 Omeprazole 668 14,502 15,171 5 Malaysian Statistics on Medicines 2006 CHAPTER 2 EXPENDITURE ON MEDICINES IN MALAYSIA Rank ATC Drugs Public Private Total 17 A10A D01 4,429 10,209 14,639 18 C08C A05 Insulins and analogues, intermediate-acting combined with fast-acting (human) Nifedipine 11,520 1,721 13,241 19 C08C A02 Felodipine 8,750 4,165 12,916 20 R03B A01 Beclometasone 10,526 2,218 12,744 21 C09A A04 Perindopril 8,394 3,276 11,670 22 A02B A02 Ranitidine 8,212 1,861 10,073 23 C09C A01 Losartan 4,511 5,310 9,821 24 A10B F01 Acarbose 5,728 3,919 9,647 25 B01A C05 Ticlopidine 8,163 965 9,128 26 A10A B01 Insulins and analogues, fast-acting (human) 2,849 5,691 8,539 27 R06A E07 Cetirizine 5,831 2,511 8,341 28 A10A C01 Insulins and analogues, intermediate-acting (human) 197 8,052 8,249 29 J01F A01 Erythromycin 6,080 1,950 8,030 30 R03A C02 Salbutamol 5,550 2,461 8,011 31 C07A A05 Propranolol 6,613 1,001 7,614 32 R03B A02 Budesonide 129 7,480 7,609 33 M05B A04 Alendronic acid 6,097 1,038 7,136 34 A10B B01 Glibenclamide 5,659 1,384 7,043 35 R03A K06 2,513 4,294 6,807 36 R03A C13 Salmeterol and other drugs for obstructive airway diseases Formoterol 2,150 4,473 6,623 37 N03A G01 Valproic acid 6,363 61 6,424 38 J01C F02 Cloxacillin 5,663 717 6,380 39 R03C C02 Salbutamol 5,417 769 6,185 40 R06A A02 Diphenhydramine 539 5,502 6,041 41 R03C C03 Terbutaline 5,316 609 5,925 42 K07R03A 399 5,192 5,590 43 J01C A04 Formoterol and other drugs for obstructive airway diseases Amoxicillin 2,054 3,243 5,298 44 A10B G02 Rosiglitazone 1,140 4,066 5,206 45 M01A H01 Celecoxib 2,767 2,438 5,205 46 C02C A01 Prazosin 4,530 620 5,150 47 R06A X13 Loratadine 423 4,696 5,119 48 C10A B04 Gemfibrozil 4,742 83 4,825 49 M01A H05 Etoricoxib 463 4,218 4,681 50 C01E B15 Trimetazidine 1,331 3,291 4,622 Total Top 50 drugs by Expenditure 334,317 237,381 571,698 Total Top 150 drugs by Expenditure 442,837 341,550 765,356 6 CHAPTER 2 EXPENDITURE ON MEDICINES IN MALAYSIA Malaysian Statistics on Medicines 2006 Table 2.2: Top 10 Therapeutic Groups by Expenditure in RM ‘000 Rank ATC Therapeutic Group Public Private Total 1 A10 Drugs Used in Diabetes 62,752 33,317 96,069 2 C09 Agents Acting on Renin-Angiotensin System 54,523 25,405 79,928 3 J01 Antibacterials for Systemic Use 42,343 35,267 77,610 4 C10 Lipid Modifying Agents 22,516 48,120 70,636 5 R03 Drugs for Obstructive Airway Diseases 38,629 23,776 63,374 6 C07 Beta Blocking Agents 35,705 24,449 60,154 7 C08 Calcium Channel Blockers 41,462 17,549 59,011 8 A02 Drugs For Acid Related Disorders 12,604 24,650 37,254 9 M01 Antiinflammatory and Antirheumatic Products 6,945 28,019 34,964 10 B01 Antithrombotic Agents 8,538 22,724 31,262 Table 2.3: Top 10 Drugs Ranked by Expenditure Rank Malaysia Australia Public Expenditure Private Expenditure Total Expenditure Total Expenditure 1 Metoprolol Atorvastatin Amlodipine Atorvastatin 2 Amlodipine Simvastatin Atorvastatin Simvastatin 3 Risperidone Diclofenac Metoprolol Esomeprazole 4 Captopril Clopidogrel Simvastatin Salmeterol and Fluticasone 5 Enalapril Atenolol Cefuroxime Clopidogrel 6 Metformin Omeprazole Metformin Olanzapine 7 Cefuroxime Amlodipine Gliclazide Omeprazole 8 Gliclazide Amoxicillin and enzyme inhibitor Risperidone Vanlafaxine 9 Insulins and analogues, intermediate-acting combined with fast-acting (human) Felodipine Cetirizine Atenolol Pantoprazole Cefuroxime Captopril Alendronic Acid 10 Table 2.4: Top 10 Therapeutic Groups Ranked by Expenditure Rank Malaysia Australia Public Expenditure Private Expenditure Total Expenditure Total Expenditure Drugs Used in Diabetes (A10) Agents Acting on ReninAngiotensin System (C09) Lipid Modifying Agents (C10) Antibacterials for Systemic Use (J01) Lipid Modifying Agents (C10) 3 Antibacterials for Systemic Use (J01) Drugs Used in Diabetes (A10) 4 Calcium Channel Blockers (C08) Anti-inflammatory and Antirheumatic Products (M01) Drugs Used in Diabetes (A10) Agents Acting on Renin-Angiotensin System(C09) Antibacterials for Systemic Use (J01) Lipid Modifying Agents (C10) 1 2 7 Drugs For Acid Related Disorders (A02) Agents Acting on ReninAngiotensin System (C09) Psychoanaleptics (N06) CHAPTER 2 EXPENDITURE ON MEDICINES IN MALAYSIA Malaysian Statistics on Medicines 2006 Rank Malaysia Australia Public Expenditure Private Expenditure Total Expenditure Total Expenditure 5 Drugs for Obstructive Airway Diseases (R03) Beta Blocking Agents (C07) Drugs for Obstructive Airway Diseases (R03) Beta Blocking Agents (C07) Drugs for Obstructive Airway Diseases (R03) 6 Agents Acting on Renin-Angiotensin System (C09) Drugs For Acid Related Disorders (A02) 7 Psycholeptics (N05) Beta Blocking Agents (C07) Calcium Channel Blockers (C08) Drugs Used in Diabetes (A10) 8 Lipid Modifying Agents (C10) Drugs for Obstructive Airway Diseases (R03) Antineoplastic Agents (L01) 9 Drugs For Acid Related Disorders (A02) Antithrombotic Agents (B01) Drugs For Acid Related Disorders (A02) Antiinflammatory and Antirheumatic Products (M01) Psycholeptics (N05) Antithrombotic Agents (B01) References: 1. Institute of Public Health (IPH) 2008. The Third National Health and Morbidity Survey (NHMS III) 2006, Vol 1. Ministry of Health, Malaysia. 2. Commonwealth of Australia 2008. Australian Statistics on Medicines 2006 Online ISBN: 1-74186-516-6. Available from http://www.health.gov.au/internet/main/publishing.nsf/Content/health-pbs general-pubs asm.htm 3. Commonwealth of Australia 2006. Pharmaceutical Benefits Pricing Authority Annual Report for the year ended 30 June 2006. Online ISBN: 1 74186 119 5. available from: http://www.health.gov.au/internet/wcms publishing.nsf/Content/health-pbs-general-pricing-pbparpt.htm 8 CHAPTER 3 USE OF MEDICINES FOR ACID RELATED DISORDERS Malaysian Statistics on Medicines 2006 Edited by: Radzi H1, Menon J2, Zainon A3, Azuana R4 1. Alor Star Hospital, 2. Queen Elizabeth Hospital, 3. Selayang Hospital, 4. Serdang Hospital The common causes of acid related disorders include non-ulcer dyspepsia, peptic ulcer disease and gastroesophageal reflux disease (GERD). Prevalence of acid related disorders in Asian countries is low at under 10% compared to the more developed nations which can range between 10%-40% depending on the definition being used [2]. In studies using upper abdominal pain as definition, the lowest prevalence of 8% is seen in Singapore [3]. Slightly higher rates are seen amongst the Scandinavians at 14.5% to 18.4%. Prevalence rates of 23-25.8% are reported in the US [4]. In this survey, the total utilisation of drugs for acid related disorders in 2006 is 5.15685 DDD/1000 population/day, similar to the previous year’s finding of 5.1619DDD/1000 population/day. Concurring to the prevalence rate, utilisation of this group of drugs was relatively small compared to consumption in developed countries. The consumption in the Nordic Countries in 2003 for example ranged from 18.3DDD/1000 population/day in Greenland to 56.5DDD/1000 population/day in Iceland [1], which is far greater than utilisation reported here. In Australia, consumption for acid related disorder stands at a whopping 64.99 DDD/1000 population/day [7]. In addition to the low prevalence of acid related disorders in our population, another contributory factor to the low overall consumption could also be the omission of antacid and alginates from this report. These compounds are largely used as first line treatment for symptoms of acid related disorders. Self medicating in many patients with this disorder may have also resulted in under reporting of the actual usage. Additionally, drugs for acid related disorders are usually used for treatments of short durations. Thus, utilisation of drugs for acid related disorder is relatively small when compared to therapeutic groups. In the NMUS 2005 report, utilisation of acid related disorder drugs was at number 14 among the 30 therapeutics groups under study. Drugs used for diabetes top the list at 35.86DDD/1000 population/day, seven times more than utilisation reported for acid related disorders group. Overall, among the major drug classes for acid related disorders, H2 Receptor Antagonist (H2RA) tops the list with usage of 2.94DDD/1000 population/day (56.9%) in 2006, trailed closely by Proton Pump Inhibitors (PPI) at 2.21DDD/1000 population/day (42.9%). This pattern is somewhat inconsistent with other countries where usage of PPIs is usually more dominant compared to H2RA. For example in Nordic Countries, PPI was the largest group of drugs used for acid related disorders taking the share of 60-80% of the AO2 group consumption. In Finland, the usage of PPIs was about five times higher at 22.5DDD/1000 population/day compared to usage of H2RA of only 4.1DDD/1000 population/day. On the other hand, in this study, for private practice where prescribing is not restricted by formulary, this common trend is observed whereby PPI consumption was about 14% higher (1.42DDD/1000 population/day and 1.23 DDD/1000 population/day for private and public sectors respectively). Among all available agents for acid related disorders, ranitidine was utilised the most in 2006 at 1.71DDD/1000 population/day (33.2%) followed by omeprazole at 1.5DDD/1000 population/day (29.1%). In the H2RA drug class, utilisation of cimetidine is second after ranitidine representing 30.4 % of all H2RAs. Famotidine (11.3% of H2RAs) and nizatidine (0.01%) were mainly used in private practice. Omeprazole dominated the PPI drug class making up for 67.8% of all agents in this group. This was followed by esomeprazole (13.5%), lansoprazole (9.3%), pantoprazole (6.4%) and rabeprazole (3%). In 2006, omeprazole was the only PPI in generic formulation available in Malaysia. In Australia, omeprazole was also the most used acid reducing agent at 18.6DDD/1000 population/day (31.9% of all PPIs) [7]. Currently, the driving force behind the utilisation trend observed in this study was mainly the prescribing restrictions enforced through formularies, generic availability and costs. In the public sector the prescribing of PPIs are limited to specialist clinics and hospitals whilst H2RA are readily available in most primary clinics and health care centres. Availability of omeprazole in generic form has significantly reduced costs and consequently making it more accessible. 9 Malaysian Statistics on Medicines 2006 CHAPTER 3 USE OF MEDICINES FOR ACID RELATED DISORDERS In developed countries, there is an apparent consensus among physicians on using PPIs as first line treatment for GERD as it is more potent, effective and generally possess good safety profile [6]. Usage of PPIs is foreseen to eventually surpass H2RA following the trend in the western population. Based on the changing trend of prevalence locally, partly due to changing lifestyle and dietary habits, the overall utilisation trend of drugs for acid related disorders is expected escalate. Table 2.1: Top 50 Drugs by Expenditure in RM ‘000 ATC Drug Class 2006 A02B A H2-receptor antagonists 2.9354 A02B B A02B C A02B D A02B X Prostaglandins Proton pump inhibitors Combinations for eradication of Helicobacter Pylori Other drugs for peptic ulcer and gastro-oesophageal reflux disease (GORD) 0.0016 2.2125 0.0067 0.0006 Table 3.2: Use of Medicines for Acid Related Disorders by Drug Class and Agents, in DDD/1000 population/day 2006 ATC Drug Class and Agents A02B A H2-receptor antagonists A02B A01 Cimetidine A02B A02 Ranitidine A02B A03 Famotidine A02B A04 Nizatidine A02B B A02B B01 Prostaglandins Misoprostol A02B C A02B C01 Proton pump inhibitors Omeprazole A02B C02 Pantoprazole A02B C03 Lansoprazole A02B C04 Rabeprazole A02B C05 Esomep razole 2006 10 Public Private Total Public Private Total Public Private Total Public Private Total 0.515 0.3763 0.8913 1.1741 0.539 1.7131 0.0202 0.3104 0.3306 0.0004 0.0004 Public Private Total <0.0001 0.0016 0.0016 Public Private Total 0.5889 0.9111 1.5 Public Private Total Public Private Total Public Private Total Public Private Total 0.0471 0.0952 0.1423 0.1271 0.0775 0.2046 0.0094 0.0565 0.0659 0.019 0.2807 0.2997 CHAPTER 3 USE OF MEDICINES FOR ACID RELATED DISORDERS Malaysian Statistics on Medicines 2006 ATC Drug Class and Agents 2006 A02B D04 Pantoprazole, amoxicillin and clarithromycin 0.0067 0.0067 A02B X A02B X05 Public Private Total Other drugs for peptic ulcer and gastro-oesophageal reflux disease (GORD) Bismuth subcitrate Public Private Total 0.0006 0.0006 References: 1. Committee NM-S, (NOMESCO). Medicines Consumption in the Nordic Countries 1999-2003. 2. HB El-Serag NJT. The prevalence and clinical course of functional dyspepsia. Alimentary Pharmacology & Therapeutics. 2004; 19(6):643-54. 3. Ho KY, Cheung TK, Wong BC. Gastroesophageal reflux disease in Asian countries: disorder of nature or nurture? J Gastroenterol Hepatol. 2006 Sep; 21(9):1362-5. 4. Mahadeva S, Goh KL. Epidemiology of functional dyspepsia: a global perspective. World J Gastroenterol. 2006 May 7; 12(17):2661-6. 5. Mahadeva S, Raman MC, Ford AC, Follows M, Axon AT, Goh KL, et al. Gastro-oesophageal reflux is more prevalent in Western dyspeptics: a prospective comparison of British and South-East Asian patients with dyspepsia. Aliment Pharmacol Ther. 2005 Jun 15; 21(12):1483-90. 6. Modlin IM, Moss SF, Kidd M, Lye KD. Gastroesophageal reflux disease: then and now. J Clin Gastroenterol. 2004 May-Jun; 38(5):390-402. 7. Australian Government Department of Health and Ageing. Australian Statistics on Medicines. 2006 12th Edition. 11 CHAPTER 4 USE OF ANTIOBESITY MEDICINES Malaysian Statistics on Medicines 2006 Edited by: Sharmini S1, Ariza Z1, Oiyammal C2, Lim K3, Cheng MF4, Nazri D5 1.Clinical Research Centre, MOH 2.Sungai Bakap Hospital, 3.Penang Hospital, 4.Xepa-Soul Pattinson 5. Tampin Health Clinic The total consumption of anti-obesity drugs in Malaysia for 2006 was 0.72 DDD/1000 population/day. Centrally acting anti-obesity drugs were most commonly prescribed representing 94.3 percent of drugs used. Among the centrally acting agents used, phentermine was the favored choice (67%). Of the anti-obesity medicines utilised, consumption in the public sector was practically negligible. The private sector utilisation captured a market share of 97.8 percent. This was actually an under represented value considering private sector response rates were much lower than the public sector. The differing utilisation rates could be an influence of cost and availability of drugs. In Australia, the consumption of anti-obesity drugs is almost three fold higher; probably due to the higher prevalence of obesity. Table 4.1: Use of antiobesity medicine by Drug Class, in DDD/1000 population/day 2006 ATC Drug Class A08A A08A A A08A B ANTIOBESITY PREPARATIONS, EXCL. DIET PRODUCTS Centrally acting antiobesity products Peripherally acting antiobesity products 2006 0.7187 0.678 0.0408 Table 4.2: Use of antiobesity medicine by Drug Class and Agents, in DDD/1000 population/day 2006 ATC Drug Class and Agents 2006 A08A A Centrally acting an tiobesity products A08A A01 Phentermine A08A A10 Sibutramine A08A B Peripherally acting antiobesity products A08A B01 Orlistat Public Private Total Public Private Total 0.0019 0.4521 0.4541 0.0112 0.2127 0.2239 Public Private Total 0.003 0.037 7 0.0408 References: 1. Australian Statistics on Medicine 2006. Commonwealth Department of Health and Ageing Australia. 13 CHAPTER 5 USE OF ANTIDIABETICS Malaysian Statistics on Medicines 2006 Edited by: GR Letchumanan R1, Muruga V2, Sharmini S3, Ariza Z3, Oiyammal C4, Lim K5, Cheng MF6, Nazri D7 1. Taiping Hospital, 2. Sanofi Aventis, 3. Clinical Research Centre, MOH 4. Sungai Bakap Hospital, 5. Penang Hospital 6. Xepa-Soul Pattinson, 7. Tampin Health Clinic The total consumption of anti-diabetic drugs in Malaysia for 2006 was 40.3DDD/1000 population/day. This figure presented a rough estimation for Malaysian diabetic prevalence of four percent. This is lower than the National Health and Morbidity Survey 2006 findings of 9.5 percent known diabetes and 14.9 percent total diabetes prevalence [1]. When adult population values was used (aged 30 and above), the new anti-diabetic drug consumption was 98.7DDD/1000 population/day indicating a diabetes prevalence of 9.87 percent which is consistent with the National Health and Morbidity Survey 2006. Among the antidiabetic drugs, the most utilised were sulphonylureas (54.8%), followed by biguanides (32.6%), insulin (8.2%) and combination drugs (2.7%). The total anti-diabetic drug utilisation for Australia was 44.8 DDD/1000 population/day, most common being biguanides (34.0%), followed by insulin (32.5%), sulphonylureas (27.8%) and thiazolidinediones (5.2%) [2]. Among the oral hypoglycaemic drugs, sulphonylureas (22.1DDD/1000 population/day) were the most commonly consumed followed by metformin (13.2DDD/1000 population/day). Metformin usage was disappointingly lower than sulphonylurea. Similar usage pattern of metformin was also reported in MSOM 2005 and this was in contrast with current guidelines. When compared to Malaysian drug utilisation, sulphonylurea use in Australia was almost half (12.5DDD/1000 population/day) whilst metformin use was comparable (15.2DDD/1000 population/day). Alpha glucosidase inhibitors consumption in Malaysia (0.46DDD/1000 population/day) was almost doubled to that of Australian usage (0.2DDD/1000 population/ day). Thiazolidinediones use was very low (0.2DDD/1000 population/day) in Malaysia. Australia’s use was more than 10 fold (2.3DDD/1000 population/day). The reason for the extremely low consumption of thiazolidinediones may be due to its accessibility; high cost, and it being a List A drug requiring a specialist prescription in public hospitals. Private hospitals and private specialist clinics which may prescribe these drugs are underrepresented in this survey. Insulins and its analogues are underutilised in the country, representing only 8.2 percent of anti-diabetic drugs used versus 32.5 for Australia. This was only 25 percent of Australian insulin coverage. This was very low but expected because of the Malaysian culture of reluctance to use injectable drugs. This is an area which we must improve to ensure better management of diabetes in the country. The pattern of prescribing insulin, however, was consistent to that in Australia with the most preferred type of insulin being the combined intermediate/fast acting insulin, followed by fast-acting, intermediate-acting and lastly long-acting insulin. In general, anti-diabetic drug utilisation was greater in the public sector compared to the private; suggesting a disproportionate burden of disease within our health care system. Table 5.1: Use of Anti-Diabetics by Drug Class, in DDD/1000 population/day 2006 ATC Drug Class A10A A10B A A10B B A10B D A10B F A10B G A10B X INSULINS AND ANALOGUES Biguanides Sulfonamides, urea derivatives Combinations of oral blood glucose lowering drugs Alpha glucosidase inhibitors Thiazolidinediones Other blood glucose lowering drugs, excl. insulins 15 2006 3.295 13.1506 22.0883 1.0687 0.4507 0.2057 0.0367 CHAPTER 5 USE OF ANTIDIABETICS Malaysian Statistics on Medicines 2006 Table 5.2: Use of Anti-Diabetics by Drug Class and Agents, in DDD/1000 population/day 2006 ATC A10A B Drug Class and Agents Insulins and analogues for injection, fast-acting A10A B01 Insulins and analogues, fast-acting (human) A10A B04 A10A B05 Insulins and analogues, fast-acting; insulin lispro Insulins and analogues, fast-acting; Insulin aspart A10A C Insulins and analogues for injection, intermediate-acting A10A C01 Insulins and analogues, intermediate-acting (human) 2006 Public 0.6717 Private 0.283 Total 0.9547 Public 0.001 Private 0.001 Total 0.002 Public 0.0065 Private 0.0029 Total 0.0094 Public 0.7004 Private 0.2216 Total 0.922 A10A D Insulins and analogues for injection, intermediate-acting combined with fast-act A10A D01 Insulins and analogues, intermediate-acting combined with fast-acting (human) A10A D05 Insulins and analogues, intermediate-acting combined with fast-acting Insulin aspart A10A E Insulins and analogues for injection, long-acting A10A E04 Insulins and analogues, long-acting; Insulin glargine A10B A Biguanides A10B A02 Metformin A10B B Sulfonamides, urea derivatives A10B B01 Glibenclamide A10B B02 A10B B07 A10B B09 A10B B12 Chlorpropamide Glipizide Gliclazide Glimepiride 16 Public 1.1299 Private 0.1955 Total 1.3255 Public 0.0003 Private 0.0288 Total 0.0291 Public 0.0119 Private 0.0404 Total 0.0523 Public 11.1397 Total 13.1506 Private 2.0109 Public 14.0329 Private 1.5023 Total 15.5352 Public 0.0238 Private 0.0251 Total 0.0488 Public 0.0255 Private 0.0721 Total 0.0975 Public 4.593 Private 1.3678 Total 5.9608 Public 0.0261 Private 0.4199 Total 0.446 CHAPTER 5 USE OF ANTIDIABETICS Malaysian Statistics on Medicines 2006 ATC A10B D Drug Class and Agents Combinations of oral blood glucose lowering drugs A10B D02 Metformin and sulfonamides A10B D03 Alpha glucosidase inhibitors A10B F01 Acarbose A10B G Thiazolidinediones A10B G02 Rosiglitazone A10B G03 Public Metformin and rosiglitazone A10B F Pioglitazone A10B X Other blood glucose lowering drugs, excl. insulins A10B X02 Repaglinide A10B X03 2006 Nateglinide 0.0113 Private 1.0128 Total 1.02 41 Public 0.0014 Private 0.0431 Total 0.0446 Public 0.3652 Private 0.0856 Total 0.4507 Public 0.040 6 Private 0.1635 Total 0.2041 Public - Private 0.0016 Total 0.0016 Public 0.0099 Private 0.015 Total 0.0249 Publ ic 0.0009 Private 0.0109 Total 0.0118 References: 1. The National Health Morbidity Survey 3, Institute of Public Health, Ministry of Health Malaysia 2007. 2. Australian Statistics on Medicines 2006. Commonwealth Department of Health and Ageing Australia. 3. David M. Nathan, MD et al. Management of Hyperglycemia in Type 2 Diabetes: Consensus Algorithm for the Initiation and Adjustment of Therapy. A consensus statement from the American Diabetes Association and the European Association for the Study of Diabetes. DIABETES CARE, Volume 29, No. 8, August 2006; 1963-1972. 4. Malaysian Statistics of Medicines 2005, Ministry of Health Malaysia. 17 CHAPTER 6 USE OF ANTIANAEMIC MEDICINES Malaysian Statistics on Medicines 2006 Edited by: Lim YS 1, Goh AS2 1. Kuala Lumpur Hospital, 2. Pulau Pinang Hospital In this chapter only two antianaemic preparations were described namely parenteral iron and erythropoietin. There was no procurement data captured on oral iron preparations though Oncology, Obstetric and Gynaecology as well as General Medicine uses quite a fair amount for anaemia. Erythropoeitin is also known as recombinant human erythropoietin (rHuEPO) which is a protein hormone produced by specialised cells in the kidneys. When there are few red blood cells as in anaemia, erythropoietin would be released to stimulate the bone marrow to produce more red blood cells. Where the production of endogenous erythropoietin is defective as in multiple myeloma or non-Hodgkin Lymphoma, erythropoietin could ameliorate the anaemia but users are cautioned of its use with chemotherapy that are thrombogenic or in cancer patients who are at risk of thromboembolism. Haematology and Oncology hardly use any erythropoietin. In Malaysia, erythropoietin was the standard of care for many patients with end-stage renal disease (ESRD) except for those who develop antibodies to the erythropoietin, who develop pure red cell aplasia or who develop arterial hypertension. When the hidden costs of the complications of blood transfusion were taken into account, erythropoietin would be a potential and cost effective alternative to transfusion. In some cases intravenous iron without erythropoietin was just as effective in treating the anaemia. For erythropoietin to be effective, it should be supplemented with iron. Parenteral iron was more effective than oral iron. However there was no data on iron dextran nor on ferric sucrose but on trivalent parenteral iron namely saccharated iron oxide. Less than 0.0001 DDD/1000 population/ day and only the private sector used this. Hence less than 0.00001% of the population was using this daily. Australia used Iron Polymaltose Complex as the trivalent parenteral iron compound in the amount of 0.023DDD/1000 population/day and was more or less constant throughout the three years surveyed from 2001 till 2003. This was under their pharmaceutical benefits scheme. By comparison Malaysia used much less parenteral iron. Erythropoietin use in Australia in 2006 was 0.044DDD/1000 population/day and consumption of darbepoetin alpha was more favoured with use of nearly 4 times higher (0.17DDD/1000 population/day). In Malaysia, erythropoietin utilisation in 2006 was 0.178 DDD/1000 population/day and this meant that 0.018% of the population used erythropoietin on a daily basis. Usage in the government sector was 1.6 times higher than the private sector. Access to this antianaemic which was considered expensive therapy had been made possible to haemodialysis patients and other ESRD cases through the Nephrology budget. This consumption data was based on assumption that all the erythropoietin purchased were consumed and that the prescribed daily dose was the same as the defined daily dose. However neither the erythropoietin nor the trivalent parenteral iron was used every day of the year. If supplementary information was available such as the average duration of treatment rather than assuming that the medication was taken every day of the year, drug utilisation could be reported in terms of number of patients treated during the year. Table 6.1: Use of Antianaemic, in DDD/1000 population/day 2006 ATC Drug Class 2006 B03 ANTIANAEMIC PREPARATIONS 0.178 Table 6.2: Use of Antianaemic by Drug Class, in DDD/1000 population/day 2006 ATC Drug Class 2006 B03A B03A C B03X B03X A IRON PREPARATIONS Iron trivalent, parenteral preparations OTHER ANTIANAEMIC PREPARATIONS Other antianaemic preparations <0.0001 <0.0001 0.178 0.178 19 CHAPTER 6 USE OF ANTIANAEMIC MEDICINES Malaysian Statistics on Medicines 2006 Table 6.3: Use of Antianaemic by Drug Class and Agents, in DDD/1000 population/day 2006 ATC B03A C Drug Class and Agents Iron trivalent, parenteral preparations B03A C02 Saccharated iron oxide B03X A Other antianaemic preparations B03X A01 Erythropoietin 2006 Public Private Total <0.0001 <0.0001 Public Private Total 0.1094 0.0686 0.178 References: 1. Australia Department of Heath and Ageing, Australian Statistics On Medicine 2003. 2. Statistics on Drug use in Australia 2006. 20 CHAPTER 7 USE OF ANTIHAEMORRHAGIC MEDICINES Malaysian Statistics on Medicines 2006 Edited by: Lim YS 1, Goh AS2 1. Kuala Lumpur Hospital, 2. Pulau Pinang Hospital Concerns for the safety of blood transfusions are partly the cause for the development of a range of interventions to minimise blood loss during major surgeries. One of the interventions is the widespread use of anti-fibrinolytic agents especially in cardiac surgeries where they are found to reduce blood loss and decrease the need for red cell transfusions. Tranexamic acid is a synthetic derivative which exerts its anti-fibrinolytic effect through reversible blockade of lysine binding sites on plasminogen molecules. It was the most commonly prescribed anti-haemorrhagic agent in 2006 (0.068DDD/1000 population/day). Tranexamic acid is effective in reducing postoperative blood loss in patients undergoing cardiac surgeries with statistically significant reductions in transfusion requirements. In comparison, the usage of aprotinin was rather low (<0.0006DDD/1000 population/day) and was mainly used therapeutically in open heart surgeries and cardiopulmonary bypass surgeries. Interestingly the usage of aprotinin was more than 6 times higher in the private institutions reflecting that a higher number of cardiac surgeries were being done in the private sector. Aprotinin is a proteinase inhibitor from bovine organs and can only be given intravenously. The loading dose of aprotinin is 15,000 to 20,000 kallikrein inhibitory units (kiu)/kg body weight as short intravenous infusions followed by 50,000 kiu/hour by continuous infusion. On the other hand, tranexamic acid can be given orally since it is readily absorbed from gastrointestinal tract and excreted in its active form in the urine. With short plasma half-life of 80 minutes, tranexamic acid side effects are transient mainly manifesting as nausea or diarrhoea. The main indications for tranexamic acid are to prevent excessive bleeding after prostatic surgery, liver transplant, tonsillectomy, cervical conisation, primary and intrauterine device-induced menorrhagia, from gastric and intestinal sites, from epistaxis and ocular trauma, after tooth extraction in haemophilia and hereditary angioneurotic edema. It is also used in controlling bleeding in pregnancy. Tranexamic acid could be administered intravenously at a dose of 0.5–1g (10-15mg/kg body weight) two to three times a day or administered orally at 1-1.5 g three to four times daily. In renal insufficiency, this dose needs to be reduced. Tranexamic acid was reported to be more effective than mefenamic acid and norethisterone but less effective than intrauterine administration of levonorgestrel in reduction of menstrual blood loss in clinical trials. However the high incidence of amenorrhoea and adverse events such as intermenstrual bleeding reported with some hormonal therapy may be unacceptable to patients in which case tranexamic acid would be particularly useful. Hence tranexamic acid remains as the first line therapy for initial management of idiopathic menorrhagia for three to four days cycle over two to three cycles to reduce menstrual blood loss. Factor VIII and IX concentrates are used to treat bleeding episodes in haemophilia A and haemophilia B respectively. In Malaysia, patients are given factor concentrates as “on-demand therapy” without charge in government hospitals. Furthermore haemophilia is a congenital disorder so the patients are not eligible for insurance coverage. Hence, most hemophiliacs seek treatment in government hospitals and the usage of factor concentrates is very low in the private sector. Recombinant factor VIIa or Eptacog alfa (activated) has been licensed for treatment of haemophilia A and B with inhibitors in Europe since 1996 and in North America since 1999. Overall 1.5 million doses had been administered. It is indicated as an intravenous haemostatic agent in hemophilia patients with inhibitors to coagulation factors VIII and IX. On-demand therapy with Eptacog alfa was effective in controlling episodes of mild to moderate bleeding. Prophylactic treatment was also effective in maintaining haemostasis in haemophiliacs undergoing orthopaedic surgeries and it is reported that the acquisition costs of Eptacog alfa are offset by cost savings resulting from the reduction in the episodes of joint-related bleeds. The data had shown that Eptacog alfa (activated) was as sparingly used in the private as in the government sector. 21 CHAPTER 7 USE OF ANTIHAEMORRHAGIC MEDICINES Malaysian Statistics on Medicines 2006 There was no data available for the use of Vitamin K or phytomenadione as a haemostatic agent even though our Malaysian hospitals do administer the vitamin intramuscularly for prophylactic use in haemorrhagic disease of the newborn. In life threatening bleeding, Vitamin K may be used therapeutically by the intravenous route together with fresh frozen plasma or factor concentrates. Table 7.1: Use of Antihaemorrhagics in DDD/1000 population/day 2006 ATC Drug Class B02 2006 ANTI HAEMORRHAGICS 0.0713 Table 7.2: Use of Antianaemics by Drug Class, in DDD/1000 population/day 2006 ATC Drug Class B02A B02A A B02A B B02B B02B A B02B D ANTIFIBRINOLYTICS Amino acids Proteinase inhibitors VITAMIN K AND OTHER HEMOSTATICS Vitamin K Blood coagulation factors 2006 0.0695 0.0688 0.0006 0.0018 0.0018 Table 7.3: Use of Antihaemorrhagics by Drug Class and Agents, in DDD/1000 population/day 2006 ATC Drug Class and Agents 2006 B02A A Amino acids B02A A02 Tranexamic acid B02A B Proteinase inhibitors B02A B01 Aprotinin B02B A Vitamin K B02B A01 Phytomenadione B02B D Blood coagulation factors B02B D02 Coagulation factor VIII B02B D04 Coagulation factor IX B02B D08 Eptacog alfa (activated) Public Private Total 0.0524 0.0165 0.0688 Public Private Total <0.0001 0.0006 0.0006 Public Private Total - Public Private Total Public Private Total Public Private Total 0.0007 <0.0001 0.0007 0.0011 0.0011 <0.0001 <0.0001 <0.0001 References: 1. Srivasta A, Chuansumrit A, Chandy M, Duraisamy G, Karagus C. Management of haemophilia in the developing world. Hemophilia 1998 Jul; 4(4):474-80. 2. Srivasta A, You SK, Ayob Y, Chuansumrit A, de Bosch N, Perez Bianco R, Ala F Hemophilia treatment in developing countries: products and protocols. Semin. Thromb. Hemost. 2005 Nov; 31(5): 495-500. 3. Stonebraker JS, Amand RE, Nagle AJ; A country-by-country comparison of FVIII concentrate consumption and economic capacity for the global hemophilia community Hemophilia Vol 9 (3) May 2003; 245-250(6). 22 CHAPTER 7 USE OF ANTIHAEMORRHAGIC MEDICINES Malaysian Statistics on Medicines 2006 4. Panicker J et al; The overall effectiveness of prophylaxis in severe haemophilia Haemophilia Vol 9, No. 3 May 2003 : 272-278. 5. Lyseng-Williamson KA, Plosker GL Recombinant factor VIIa (Eptacog alfa) a pharmacoeconomic review of its use in haemophilia in patients with inhibitors to clotting factors VIII and IX. Pharmacoeconomics 2007 : 25 (12) pgs 1007-29. 6. Puckett RM, Offringa M, Department of Paediatrics, Amsterdam. Prophylactic Vitamin K for Vitamin K deficiency bleeding in neonates. Cochrane Database Systematic Review 2000; (4): CD 002776. 23 CHAPTER 8 USE OF MEDICINES FOR CARDIOVASCULAR DISORDERS Malaysian Statistics on Medicines 2006 Edited by: Chong WP1, Wan Azman WA1 1. University Malaya Medical Centre With contributions from: Nirmala J2, Yap YJ2, Haarathi C3, Long MS4 1. Sarawak General Hospital, 2. Kuala Lumpur Hospital, 3. Tengku Ampuan Rahimah Hospital, Klang, 4. Selayang Hospital The most commonly used antithrombotic agents in 2006 were the platelet aggregation inhibitors (9.22DDD/1000 population/day), and among these, acetylsalicylic acid or aspirin accounted for slightly over 80% of the total usage. The other less frequently used platelet aggregation inhibitors included ticlopidine (0.99DDD/1000 population/day) and clopidogrel (0.74DDD/1000-population/day). Ticlopidine was used more in the public health services while the private sector utilised more clopidogrel. The role of these drugs in the treatment and prevention (primary as well as secondary) of cardiovascular diseases is well established and accepted. But they were probably under utilised in view of the fact that 27% of adults who were 30 years or older had multiple cardiovascular risk factors in the National Health and Morbidity Survey in 1996. In Australia, the total community use of aspirin alone was 19.3DDD/1000 population/day in 2005. This was almost 3 times the usage of aspirin in Malaysia. Warfarin had a DDD rate of 0.3755, placing it as the 4th most commonly used antithrombotic agent in 2006. The other antithrombotic drugs such as heparin, different types of low molecular weight heparin, fibrinolytic agents (classified as enzymes in the table) and glycoprotein IIb/IIIa receptor antagonists (abciximab, eptifibatide and tirofiban) had very low DDD rates as they were normally administered over a short period of time for the treatment of acute coronary syndromes. Isosorbide dinitrate and trimetazidine were the other 2 cardiac drugs which were fairly frequently used at 1.37 and 1.44DDD/1000 population/day respectively. Both are indicated in the treatment of chronic stable angina. As a group, diuretics had a DDD rate of 14.66. The top 3 diuretics used in 2006 were chlorothiazide (6.28), furosemide (4.89) and hydrochlorothiazide and potassium-sparing agents in combination (1.34). In contrast, furosemide (or frusemide in some countries) had a DDD rate of 19.6 in Australia in 2005. This drug is used predominantly in the acute and long term management of heart failure. It is also used to treat fluid retention in other conditions. On the other hand, chlorothiazide and hydrochlorothiazide with potassium-sparing agents in combination are antihypertensive medications. Their rate of usage simply reflected the high prevalence of hypertension among Malaysian population and probably the availability of the drugs in the government formulary. Table 8.1: Use of Drugs for Cardiovascular disorders, in DDD/1000 population/day 2006 ATC Drug Class B01 C01A C01B C01C C01D C01E C03 C04 ANTITHROMBOTIC AGENTS CARDIAC GLYCOSIDES ANTIARRHYTHMICS, CLASS I AND III CARDIAC STIMULANTS EXCL. CARDIAC GLYCOSIDES VASODILATORS USED IN CARDIAC DISEASES OTHER CARDIAC PREPARATIONS DIURETICS PERIPHERAL VASODILATORS 25 2006 9.835 0.6509 0.1483 0.2538 2.2033 1.4398 14.6643 0.0745 Malaysian Statistics on Medicines 2006 CHAPTER 8 USE OF MEDICINES FOR CARDIOVASCULAR DISORDERS Table 8.2.1: Use of Anti-Thrombotic drugs by Drug Class, in DDD/1000 population/day 2006 ATC Drug Class 2006 B01A A B01A B B01A C B01A D B01A X Vitamin K antagonists Heparin group Platelet aggregation inhibitors excl. heparin Enzymes Other antithrombotic agents 0.3755 0.2365 9.2219 0.0009 0.0003 Table 8.2.2: Use of Anti-Thrombotic drugs by Drug Class and Agents, in DDD/1000 population/day 2006 ATC Drug Class and Agents 2006 B01A A Vitamin K antagonists B01A A03 Warfarin B01A B Heparin group B01A B01 Heparin B01A B05 Enoxaparin B01A B06 Nadroparin B01A B10 Tinzaparin B01A B11 Sulodexide B01A C Platelet aggregation inhibitors excl. heparin B01A C04 Clopidogrel B01A C05 Ticlopidine B01A C06 Acetylsalicylic acid B01A C07 Dipyridamole B01A C11 Iloprost B01A C13 Abciximab 26 Public Private Total 0.2582 0.11 73 0.3755 Public Private Total Public Private Total Public Private Total Public Private Total Public Private Total 0.0403 0.0626 0.1029 0.0701 0.0297 0.0998 0.0035 0.0018 0.0054 0.0005 0.0019 0.0024 <0.0001 0.0259 0.026 Public Private Total Public Private Total Public Private Total Public Private Total Public Private Total Public Private Total 0.0678 0.6682 0.7361 0.5478 0.4434 0.9912 4.8358 2.5826 7.4184 0.0697 0.0062 0.0759 <0.0001 <0.0001 <0.0001 <0.0001 <0.0001 CHAPTER 8 USE OF MEDICINES FOR CARDIOVASCULAR DISORDERS ATC Drug Class and Agents B01A C16 Eptifibatide B01A C17 Tirofiban B01A D Enzymes B01A D0 1 Streptokinase B01A D02 Alteplase B01A D04 Urokinase B01A D10 Drotrecogin alfa (activated) B01A D11 Tenecteplase B01A X Other antithrombotic agents B01A X05 Fondaparinux Malaysian Statistics on Medicines 2006 2006 Public Private Total Public Private Total <0.0001 <0.0001 <0.0001 <0.0001 Public Private Total Public Private Total Public Private Total Public Private Tota l Public Private Total 0.0007 0.0001 0.0009 <0.0001 <0.0001 <0.0001 <0.0001 <0.0001 Public Private Total <0.0001 0.0002 0.0003 Table 8.3.1: Use of Cardiac Glycosides by Drug Class, in DDD/1000 population/day 2006 ATC Drug Class and Agents C01A CARDIAC GLYCOSIDES C01A A05 Digoxin Public Private Total Table 8.4.1: Use of Anti-Arrhythmics by Drug Class, in DDD/1000 population/day 2006 ATC Drug Class and Agents C01B B Antiarrhythmics, class Ib C01B B01 Lidocaine C01B B02 Mexiletine C01B C Antiarrhythmics, class Ic C01B C03 Propafenone C01B C04 Flecainide 27 2006 0.4195 0.2314 0.6509 2006 Public Private Total Public Private Total 0.0013 0.0005 0.0018 - Public Private Total Public Private Total 0.0006 0.0056 0.0062 0.002 0.0093 0.0113 Malaysian Statistics on Medicines 2006 CHAPTER 8 USE OF MEDICINES FOR CARDIOVASCULAR DISORDERS ATC C01B D Drug Class and Agents Antiarrhythmics, class III C01B D01 Amiodarone 2006 Public Private Total Table 8.5.1: Use of Cardiac stimulants by Drug Class, in DDD/1000 population/day 2006 ATC Drug Class and Agents C01C A Adrenergic and dopaminergic agents C01C A02 Isoprenaline C01C A03 Norepinephrine C01C A04 Dopamine C01C A06 Phenylephrine C01C A07 Dobutamine C01C A24 Epinephrine C01C E Phosphodiesterase inhibitors C01C E02 Milrinone C01C X Other cardiac stimulants C01C X08 Levosimendan 0.0318 0.0972 0.129 2006 Public Private Total Public Private Total Public Private Total Public Private Total Public Private Total Public Private Total <0.0001 <0.0001 <0.0001 0.0206 0.0029 0.0235 0.0055 0.0053 0.0108 0.0045 0.0033 0.0077 0.0115 0.0018 0.0133 0.1495 0.0436 0.193 1 Public Private Total <0.0001 0.0053 0.0053 Public Private Total <0.0001 <0.0001 Table 8.6.1: Use of Vasodilators in Cardiac diseases by Drug Class, in DDD/1000 population/day 2006 ATC Drug Class and Agents 2006 C01D A Organic nitrates C01D A02 Glyceryl trinitrate C01D A05 Pentaerithrityl tetranitrate C01D A08 Isosorbide dinitrate C01D A14 Isosorbide mononitrate Public Private Total Public Private Total Public Private Total Public Private Total 28 0.1188 0.0517 0.1705 0.0024 0.0024 1.2768 0.0932 1.3699 0.1214 0.5391 0.6605 CHAPTER 8 USE OF MEDICINES FOR CARDIOVASCULAR DISORDERS Malaysian Statistics on Medicines 2006 Table 8.6.2: Use of other cardiac preparations in Cardiac diseases by Drug Class, in DDD/1000 population/day 2006 ATC Drug Class and Agents 2006 C01E A Prostaglandins C01E A01 Alprostadil C01E B Other cardiac preparations C01E B10 Adenosine C01E B15 Trimetazidine Public Private Total <0.0001 <0.0001 <0.0001 Public Private Total Public Private Total 0.0009 0.0002 0.0011 0.6345 0.804 1.4386 Table 8.7.1: Use of Diuretics by Drug Class, in DDD/1000 population/day 2006 ATC Drug Class and Agents C03A LOW-CEILING DIURETICS, THIAZIDES C03A A03 Hydrochlorot hiazide C03A A04 Chlorothiazide 2006 Public Private Total Public Private Total 0.2597 0.8344 1.0942 6.2441 0.0355 6.2796 Public Private Total Public Private Total Public Private Total 0.0212 0.0212 0.0017 0.0017 0.0557 0.5507 0.6064 Public Private Total Public Private Total 3.9301 0.9588 4.8889 0.0219 0.0172 0.0391 Public Private Total Public Private Total 0.2517 0.1286 0.3803 0.0024 0.0071 0.0095 C03B LOW-CEILING DIURETICS, EXCL. THIAZIDES C03B A04 Chlortalidone C03B A08 Metolazone C03B A11 Indapamide C03C HIGH-CEILING DIURETICS C03C A01 Furosemide C03C A02 Bumetanide C03D POTASSIUM-SPARING AGENTS C03D A01 Spironolactone C03D B01 Amiloride C03E DIURETICS AND POTASSIUM-SPARING AGENTS IN COMBINATION Public Hydrochlorothiazide and potassium-sparing agents C03E A01 Private Total 29 1.0077 0.3358 1.3434 Malaysian Statistics on Medicines 2006 CHAPTER 8 USE OF MEDICINES FOR CARDIOVASCULAR DISORDERS Table 8.8.1: Use of Peripheral vasodilators by Drug Class, in DDD/1000 population/day 2006 ATC Drug Class and Agents 2006 C04A D Purine derivatives C04A D03 Pentoxifylline C04A E Ergot alkaloids C04A E01 Ergoloid mesylates C04A X02 Phenoxybenzamine Public Private Total 0.0485 0.0136 0.0622 Public Private Total Public Private Total 0.0123 0.0123 <0.0 001 <0.0001 References: 1. The National Health Morbidity Survey 2, Institute of Public Health, Ministry of Health Malaysia 1996. 2. Statistics on drug use in Australia 2006, Australian Institute of Health and Welfare 2007. 30 CHAPTER 9 USE OF ANTIHYPERTENSIVES Malaysian Statistics on Medicines 2006 Edited by: Hooi LS1, Zaki M2, Lim TO3, Zawawi N4, Goh BL5, Fadilah O6, Nur Salima S6, Puteri JZ6, Zarina AG6, Manjulaa DS7 1. Sultanah Aminah Hospital, Johor Bahru, 2. International Medical University, 3. Clinical Research Centre MOH, 4. Sultanah Nur Zahirah Hospital, Terengganu, 5. Serdang Hospital, 6. Selayang Hospital, 7. Kuala Lumpur Hospital Beta blockers were the most commonly prescribed antihypertensive medication (25.7DDD/1000 population/day) in 2006 followed by the calcium channel blockers (19.4). ACE inhibitors (15.3), diuretics (8.0) and angiotensin II antagonists (4.3) were also commonly used. Usage of alpha blockers and centrally acting drugs was low. In the category of beta blockers there was a small amount which was prescribed in combination with diuretics. The second largest category was the drugs antagonising the renin-angiotensin system (ACEIs and ARBs) some of which were in combination with diuretics (total 19.6DDD/1000 population/day). The calcium channel blockers (CCBs) included those with vascular effects (e.g. amlodipine and nifedipine) and those with cardiac effects (e.g. diltiazem). Diuretics were prescribed alone (8.0) or in combination with other drugs (beta blocker or ACEI or ARB or potassium sparing agents) in the same tablet (3.1) which made its overall usage quite high (total 11.1 DDD/1000 population/day). There were 3 drugs whose contribution each made up more than 10% of total utilization – metoprolol (12.3DDD/1000 population/day), atenolol (12.0) and nifedipine (11.6). Of these, two were beta blockers and one a CCB. These 3 drugs were used mainly in the public sector (88%). Overall, 80% of all antihypertensives were utilised in the public sector and 20% in the private sector. The most popular drugs in the private sector were atenolol (3.0DDD/1000 population/day), amlodipine (2.0) and enalapril (1.0). There was a tendency to use more expensive drugs in the private sector. The use of antihypertensives should be encouraged in the private sector to reduce the burden of prescribing in the public sector. Economic considerations about treating a chronic disease in the private sector may be a deterring factor. Hypertension is a silent disease (killer) and without counseling and education the public may not be willing to pay for its long term control. Generic drugs which are efficacious should be the ones of choice. Drug prescribing may have been unduly influenced by aggressive marketing by the pharmaceutical industry. Among the beta blockers, the most popular were metoprolol and atenolol. They were favoured over the older generation beta blocker propranolol. Among the ACEIs, perindopril was the most commonly used followed by enalapril and captopril. Perindopril is relatively cheap and its daily dosing is an advantage. The use of ACEIs should be encouraged as they have cardio-and renoprotective effects. The incidence of diabetes mellitus in new patients with end-stage renal failure (ESRF) was 58% in 2006 in Malaysia (1). In the early stages of diabetic nephropathy ACEIs and ARBs may help to prevent progression to ESRF. The most commonly used ARB (with or without combination diuretics) was losartan followed by valsartan, irbesartan and telmisartan. These drugs are expensive. Among the CCBs nifedipine and amlodipine were the most commonly used. Nifedipine was extensively used, 94% in the public sector. Amlodipine was popular in both the public and private sector in spite of its high cost. Its daily dosing is an advantage for patient compliance over the three times a day dosing of nifedipine. It is a long acting dihydropryridine CCB and is not contraindicated in cardiovascular disease unlike the short acting nifedipine. Among the diuretics chlorothiazide (CTZ) and HCTZ were the most commonly prescribed. The former was used by the public sector while HCTZ was used by the private sector. Their usage was low considering that they are the recommended first line drugs for hypertension. The alpha antagonists were not popular although they may be useful in hypertensive men with prostatic hypertrophy who are not at high risk of heart failure. The use of centrally acting agents was low and this may be due to their unpleasant side-effects. They are still useful as a third line drug and methyldopa is used in hypertension during pregnancy. Hydralazine should not be removed from the drug formulary as it is useful 31 CHAPTER 9 USE OF ANTIHYPERTENSIVES Malaysian Statistics on Medicines 2006 in severe hypertension during pregnancy. Minoxidil is a third line drug that sometimes controls severe hypertension although it was used sparingly as there are side-effects. Nitroprusside is an intravenous drug which was used only in ICUs to control blood pressure temporarily. The total utilisation of antihypertensives was 77.3DDD/1000 population/day. From general practice prescription data, we estimated a patient with hypertension was prescribed a median of only one antihypertensive medication. That is, the vast majority of patients (81%) in Malaysia were on mono-therapy. Thus, the utilisation statistic of 77.5DDD/1000 population/day suggested that about 6 to 7% of the population were on drug treatment for hypertension. About 40% of the population was aged > 30 years in 2006. This means that about 16% of the population aged 30 and above was taking an antihypertensive drug in 2006. There is a high prevalence of hypertension in Malaysia (43% in 2006) and a substantial number of patients were not on drug therapy or had undiagnosed hypertension (2). People with hypertension in Malaysia may need more drug treatment as less than half of those who are hypertensive were on antihypertensives. This shortfall may be greater than stated as many on treatment need more than one category of drug to control their blood pressure to the recommended target. Overall, compared to the Nordic countries (3) the use of beta blockers, agents acting on the renin-angiotensin system, calcium channel blockers and diuretics was low in Malaysia. Beta blocker use in 2003 ranged from 13.9DDD/1000 population/day in Greenland to 65.8 in Finland in 2003. For drugs acting on the renin-angiotensin system, the usage ranged from 30.7DDD/1000 population/day in Greenland to 107.8 in Finland. For calcium channel blockers the range was 15.6 in Greenland to 45.3 in Norway. The use of thiazides alone or in combination with potassium-sparing agents ranged from 10.9DDD/1000 population/day in Norway to 50.5 in Denmark in 2003. The local Clinical Practice Guideline (CPG) on hypertension (4) recommends beta blockers or diuretics as drugs of first choice for control of uncomplicated hypertension. The utilisation pattern for 2006 was not consistent with the CPG as antagonists of the renin-angiotensin system were second to beta blockers followed by the calcium channel blockers. Diuretics lagged behind in fourth place. Many of the drugs in all 4 categories except the ARBs are generic and the order of preference may reflect economic considerations. The ACEIs and ARBs are weak antihypertensives but have effects beyond blood pressure lowering. These include cardioprotection post myocardial infarction, reduction of proteinuria and renoprotection in diabetic and non-diabetic renal disease. The incidence of diabetes mellitus in Malaysia is high (14.9% in 2006) (2) and many diabetics are hypertensive. This may have some bearing when physicians in Malaysia choose an antihypertensive drug for their diabetic patients (4,5). The calcium channel blockers have few side-effects and are efficacious. Diuretics may be less used inspite of their extremely low cost because of marketing of other (more expensive) drugs by the pharmaceutical industry or the belief that they have side-effects. Table 9.1: Use of Antihypertensives by Drug Class, in DDD/1000 population/day 2006 ATC Drug Class C02A C02C A C02D C02K C03A C03B C03E C07 C08 C09A C09B C09C C09D ANTIADRENERGIC AGENTS, CENTRALLY ACTING ALPHA-ADRENORECEPTOR ANTAGONISTS ARTERIOLAR SMOOTH MUSCLE, AGENTS ACTING ON OTHER ANTIHYPERTENSIVES LOW-CEILING DIURETICS, THIAZIDES LOW-CEILING DIURETICS, EXCL. THIAZIDES DIURETICS AND POTASSIUM-SPARING AGENTS IN COMBINATION BETA BLOCKING AGENTS CALCIUM CHANNEL BLOCKERS ACE INHIBITORS, PLAIN ACE INHIBITORS, COMBINATIONS ANGIOTENSIN II ANTAGONISTS, PLAIN ANGIOTENSIN II ANTAGONISTS, COMBINATIONS 32 2006 0.6553 2.5693 0.0063 0.0006 7.3738 0.6293 1.3434 25.7343 19.3656 15.2135 0.0738 2.7293 1.5652 CHAPTER 9 USE OF ANTIHYPERTENSIVES Malaysian Statistics on Medicines 2006 Table 9.2: Use of Antihypertensives by Drug Class and Agents, in DDD/1000 population/day 2006 ATC Drug Class and Agents 2006 C02A ANTIADRENERGIC AGENTS, CENTRALLY ACTING C02A B01 Methyldopa (levorotatory) C02A C01 Clonidine C02A C05 Moxonidine C02C A Alpha-adrenoreceptor antagonists C02C A01 Prazosin C02C A04 Doxazosin C02D ARTERIOLAR SMOOTH MUSCLE, AGENTS C02D B01 Dihydralazine C02D B02 Hydralazine C02D C01 Minoxidil C02D D01 Nitroprusside C02K OTHER ANTIHYPERTENSIVES C02K X01 Bosentan C03A LOW-CEILING DIURETICS, THIAZIDES C03A A03 Hydrochlorothiazide C03A A04 Chlorothiazide C03B LOW-CEILING DIURETICS, EXCL. THIAZIDES C03B A04 Chlortalidone C03B A08 Metolazone 33 Public Private Total Public Private Total Public Private Total 0.5827 0.018 0.6007 <0.000 1 <0.0001 0.0002 0.0544 0.0545 Public Private Total Public Private Total 2.234 0.0961 2.3301 0.1764 0.0628 0.2393 Public 0.0004 Private - Total 0.0004 Public Private Total Public Private Total Public Private Total <0.0001 <0.0001 0.0047 0.0002 0.0049 0.0001 0.0008 0.001 Public Private Total <0.0001 0.0006 0.0006 Public Private Total Public Private Total 0.2597 0.8344 1.0942 6.2441 0.0355 6.2796 Public Private Total Public Private Total 0.0212 0.0212 0.0017 0.0017 CHAPTER 9 USE OF ANTIHYPERTENSIVES Malaysian Statistics on Medicines 2006 ATC Drug Class and Agents C03B A11 Indapamide 2006 C03E DIURETICS AND POTASSIUM-SPARING AGENTS IN COMBINATION C03E A01 Hydrochlorothiazide and potassium-sparing agents C07A BETA BLOCKING AGENTS C07A A05 Propranolol C07A A07 Sotalol C07A B02 Metoprolol C07A B03 Atenolol C07A B04 Acebutolol C07A B05 Betaxolol C07A B07 Bisoprolol C07A B09 Esmolol C07A G01 Labetalol C07A G02 Carvedilol C07C BETA BLOCKING AGENTS AND OTHER DIURETICS C07C A03 Pindolol and other diuretics C07C B02 Metoprolol and other diuretics C07C B03 Atenolol and other diuretics 34 Public Private Total 0.0557 0.5507 0.6064 Public Private Total 1.0077 0.3358 1.3434 Public Private Total Public Private Total Public Private Total Public Private Total Public Private Total Public Private Total Public Private Total Public Private Total Public Private Total Public Private Total 0.255 0.1815 0.4364 0.0146 0.0146 11.7536 0.5828 12.3365 9.077 2.9516 12.0287 0.0019 0.0019 0.0004 0.0703 0.0708 0.0349 0.1517 0.1866 <0.0001 <0.0001 <0.0001 0.1303 0.019 0.1493 0.0808 0.2633 0.3441 Public Private Total Public Private Total Public Private Total 0.0021 0.0021 0.0167 0.0167 <0.0001 0.1466 0.1467 CHAPTER 9 USE OF ANTIHYPERTENSIVES Malaysian Statistics on Medicines 2006 ATC C08C Drug Class and Agents SELECTIVE CALCIUM CHANNEL BLOCKERS WITH MAINLY VASCULAR EFFECTS C08C A01 Amlodipine C08C A02 Felodipine C08C A03 Isradipine C08C A04 Nicardipine C08C A05 Nifedipine C08C A06 Nimodipine C08C A09 Lacidipine C08C A13 Lercanidipine C08C SELECTIVE CALCIUM CHANNEL BLOCKERS WITH DIRECT CARDIAC EFFECTS C08D A01 Verapamil C08D B01 Diltiazem C09A ACE INHIBITORS, PLAIN C09A A01 Captopril C09A A02 Enalapril C09A A03 Lisinopril C09A A04 Perindopril C09A A05 Ramipril 35 2006 Public Private Total Public Private Total Public Private Total Public Private Total Public Private Total Public Private Total Public Private Total Public Private Total 3.2803 1.9924 5.2728 1.3805 0.4422 1.8227 0.0067 0.0067 <0.0001 0.005 0.005 10.9355 0.6772 11.6127 0.0005 0.0002 0.0007 0.014 0.014 0.0679 0.0679 Public Private Total Public Private Total 0.0378 0.0442 0.0821 0.3064 0.1747 0.4811 Public Private Total Public Private Total Public Private Total Public Private Total Public Private Total 4.1067 0.1984 4.3051 3.5113 0.9827 4.4939 0.1591 0.5872 0.7463 4.3301 0.3811 4.7113 0.3409 0.5856 0.9264 CHAPTER 9 USE OF ANTIHYPERTENSIVES Malaysian Statistics on Medicines 2006 ATC Drug Class and Agents C09A A06 Quinapril C09A A09 Fosinopril C09A A16 Imidapril C09B ACE INHIBITORS, COMBINATIONS C09B A04 Perindopril and diuretics 2006 C09C ANGIOTENSIN II AN TAGONISTS, PLAIN C09C A01 Losartan C09C A03 Valsartan C09C A04 Irbesartan C09C A06 Candesartan C09C A07 Telmisartan C09C A08 Olmesartan medoxomil C09D ANGIOTENSIN II ANTAGONISTS, COMBINATIONS C09D A01 Losartan and diuretics C09D A03 Valsartan and diuretics C09D A04 Irbesartan and diuretics C09D A06 Candesartan and diuretics C09D A07 Telmisartan and diuretics 36 Public Private Total Publ ic Private Total Public Private Total 0.0014 0.0014 0.0009 0.0058 0.0067 0.0012 0.0211 0.0223 Public Private Total 0.0066 0.0672 0.0738 Public Private Total Public Private Total Public Private Total Public Private Total Public Private Total Public Private Total 0.5202 0.5978 1.1179 0.1537 0.2183 0.372 0.1987 0.364 0.5627 0.2164 0.2164 0.2038 0.2069 0.4107 0.0496 0.0496 Public Private Total Public Private Total Public Private Total Public Private Total Public Private Total 0.1154 0.405 0.5204 0.0891 0.4154 0.5045 0.0686 0.2336 0.3022 0.0006 0.1233 0.1239 0.0195 0.0947 0.1142 CHAPTER 9 USE OF ANTIHYPERTENSIVES Malaysian Statistics on Medicines 2006 References: 1. Lim YN, Lim TO (eds). Fifteenth report of the Malaysian Dialysis and Transplant Registry 2007, Kuala Lumpur 2008. http://www.msn.org.my/nrr/report2007.htm (accessed on 1 January 2009). 2. Institute for Public Health (IPH) 2008. The Third National Health and Morbidity Survey (NHMSIII) 2006, Volume 2, page 210 and 253. Ministry of Health Malaysia. ISBN 978-983-3887-30-9. 3. Nordic Medico Statistical Committee. Medicines Consumption in the Nordic Countries 1999-2003. Copenhagen 2004. ISBN 87-89702-52-2. 4. Academy of Medicine Malaysia, Ministry of Health Malaysia. Clinical practice guidelines on management of hypertension, 2002. http://www.acadmed.org.my/html/index.shtml (accessed on 10 June 2007). 5. Academy of Medicine Malaysia, Ministry of Health Malaysia. Clinical practice guidelines on diabetic nephropathy, 2004. http://www.acadmed.org.my/html/index.shtml (accessed on 10 June 20 37 CHAPTER 10 USE OF LIPID LOWERING MEDICINES Malaysian Statistics on Medicines 2006 Edited by: Chang BC1, Fong AYY1, Sim KH1 With contributions from: Chong WP2, Nirmala J3, Yap YJ3, Haarathi C4, Long MS5 1. Sarawak General Hospital, 2. Universiti Malaya Medical Centre, 3. Kuala Lumpur Hospital, 4. Tengku Ampuan Rahimah Hospital, Klang, 5. Selayang Hospital The HMG Co A reductase, or more commonly known as statins, is the mainstay of treatment of hyperlipidaemia in Malaysia. It has a good safety profile and a proven track record in reducing myocardial infarction, stroke and cardiovascular death from numerous well conducted multinational trials [1,2]. Indeed, more recent evidence points towards increasingly lower LDL treatment endpoint [3] and new indications (eg: patients with high hsCRP) [4] for using stains are emerging. Therefore the usage of statins is likely to become more widespread in the next few years. The most popular statin prescribed in the public sector was lovastatin (4.05DDD/1000 population/day); for the most part related to its lower cost. Simvastatin remained the most popular statin among the private health sector followed by atorvastatin. Rosuvastatin, the most potent statin around at the moment was not commonly prescribed (0.225DDD/1000 population/day). With the advent of lower cost generic products, it is expected this picture to change gradually and the ‘higher end’ statins made more affordable throughout Malaysia. Ezetimibe, which inhibits cholesterol absorption at intestinal brush borders, had gained some traction among Malaysian prescribers (0.42DDD/1000 population/day) despite being a relatively newcomer. It is primarily used as an adjunct to statins rather than a first line drug. Despite its effectiveness in LDL lowering, evidence of ezetimibe’s clinical benefits are still pending, awaiting studies such as IMPROVE-IT [5]. The fibrates, despite being in use for a long time and having good clinical trial data [6], were still not commonly prescribed in Malaysia (1.39DDD/1000 population/day). This could be related to the fact that increasing HDL and lowering triglyceride is still not viewed as imperative as lowering LDL cholesterol by most clinicians. Overall, Malaysia still has low utilisation of lipid lowering agent compared with other developed countries. For example, Australia with a prevalence of hypercholesterolemia of about 51% [7] (similar to Malaysia – 53.5%) [8] had a statin usage of 196.23DDD/1000 population/day in 2006 [9] compared to 15.68DDD/1000 population/day in Malaysia. This seems to indicate that we still have room for improvement in the treatment of hyperlipidaemia, for both primary and secondary prevention purposes. With our country’s expanding aged population, this is vital in reducing our cardiovascular health burden and healthcare cost in future. Table 10.1: Use of Lipid Lowering Medicines by Drug Class, in DDD/1000 population/day 2006 ATC Drug Class 2006 C10A A C10A B C10A C C10A X C10B A HMG CoA reductase inhibitors Fibrates Bile acid sequestrants Other lipid modifying agents HMG CoA reductase inhibitors in combination with other lipid modifying agents 15.3216 1.3854 0.0019 0.0917 0.3593 39 CHAPTER 10 USE OF LIPID LOWERING MEDICINES Malaysian Statistics on Medicines 2006 Table 10.2: Use of Lipid Lowering Medicines by Drug Class and Agents, in DDD/1000 population/day 2006 ATC C10A A Drug Class and Agents HMG CoA reductase inhibitors C10A A01 Simvastatin C10A A0 2 Lovastatin C10A A03 Pravastatin C10A A04 Fluvastatin C10A A05 Atorvastatin C10A A07 Rosuvastatin C10A B Fibrates C10A B01 Clofibrate C10A B02 Bezafibrate C10A B04 Gemfibrozil C10A B05 Fenofibrate C10A B08 Ciprofibrate C10A C Bile acid sequestrants C10A C01 Colestyramine C10A X Other lipid modifying agents C10A X04 Benfluorex C10A X09 Ezetimibe 2006 40 Public Private Total Public Private Total Public Private Total Public Private Total Public Private Tota l Public Private Total 2.6378 3.9287 6.5665 4.0507 0.5157 4.5664 0.1956 0.2534 0.4489 0.1862 0.1862 0.786 2.537 3.323 0.0062 0.2244 0.2306 Public Private Total Public Private Total Public Private Total Public Private Total Public Private Total 0.0002 0.0002 0.0002 0.0002 0.7413 0.0285 0.7698 0.199 0.3695 0.5684 0.0122 0.0346 0.0468 Public Private Total 0.0005 0.0014 0.0019 Public Private Total Public Private Total 0.0195 0.0195 0.0077 0.0645 0.0722 CHAPTER 10 USE OF LIPID LOWERING MEDICINES Malaysian Statistics on Medicines 2006 ATC C10B A Drug Class and Agents 2006 HMG CoA reductase inhibitors in combination with other lipid modifying agents C10B A02 Simvastatin and ezetimibe Public Private Total 0.0021 0.3571 0.3593 References: 1. Shepherd J, Cobbe SM, Ford I, et al. for the West of Scotland Coronary Prevention Group. Prevention of coronary heart disease with pravastatin in men with hypercholesterolaemia. N Eng J Med 1995; 333:1301-7 2. Scandinavian Simvastatin Survival Study Group. Randomised trial in cholesterol lowering in 4444 patients with coronary heart disease: the Scandinavian Simvastatin Survival Study (4S). Lancet 1994; 344:1383-9. 3. LaRosa JC, Grundy SM, Waters DD, et al. Intensive lipid lowering with atorvastatin in patients with stable coronary disease. N Eng J Med 2005. 4. Ridker PM, Eleanor Danielson, Fonseca F, et al. Rosuvastatin to Prevent Vascular Events in Men and Women with Elevated C-Reactive Protein (JUPITER). N Eng J Med Nov. 2008. 5. Cannon CP, Guigliano RP, et al. Rationale and design of IMPROVE-IT (IMProved Reduction of Outcomes: Vytorin Efficacy International Trial): comparison of ezetimbe/simvastatin versus simvastatin monotherapy on cardiovascular outcomes in patients with acute coronary syndromes. Am Heart J. Nov. 2008. 6. Helsinki Heart Study: primary-prevention trial with gemfibrozil in middle-aged men with dyslipidemia. Safety of treatment, changes in risk factors, and incidence of coronary heart disease. Frick MH - N Eng J Med Nov. 1987. 7. Australian Diabetes, Obesity and Lifestyle Study (AusDiab). 2001 Report. 8. Non-communicable Disease Surveillance Programme, Malaysia, 2006. 9. Australian Statistics on Medicine 2006. Department of Health and Aging, Australian Government. 41 CHAPTER 11 USE OF DERMATOLOGICALS Malaysian Statistics on Medicines 2006 Edited by: Rohna R1, Asmah J2, Roshidah B3 1. Selayang Hospital, 2. Kuala Lumpur Hospital, 3. Melaka Hospital The topical dermatological medicaments included in this study were antifungals, anti-psoriatics, antibiotics, antivirals, corticosteroids, anti-acne agents, hair growth stimulants, depigmenting agents, calcineurin inhibitors and metronidazole. Topical dermatological medicament is the major therapeutic modality used in treating patients with skin disorders. Utilisation is measured as total dose of topical medicament in g/ml/1000 population/day. There is a disparity in the utilisation of dermatological medicaments by public and private health care providers with the latter having access to a larger variety of topical medicaments (Table A). Prescribing only medicaments that are available in the Ministry of Health (MOH) drug formulary by healthcare providers in the public sector is one possible explanation for the disparity. The list of medicaments (Table A) that were utilised only by private healthcare providers was not available in the MOH drug formulary. In the public sector, prescribing of certain dermatological medicaments (e.g. topical anti-acne agents) is only by trained dermatologists and they are few in number. In private sector, the non-dermatologists have access to clindamycin and various other topical anti-acne agents such as adapalene and azelaic acid. The lower usage of the newer but expensive medicaments (e.g. tacrolimus, pimecrolimus, imiquimod and metronidazole) in government healthcare facilities was because of the availability of their cheap and effective equivalents in the MOH drug formulary. In special cases of drug resistance or contraindication, prescribing of dermatological medicaments not in the MOH formulary is permissible after seeking approval from the Director General of Health, Malaysia. In government healthcare facilities, procurement of dermatological medicaments for acute (acute cutaneous infections) and chronic skin diseases (eczema and psoriasis) took preference over hair growth stimulants (minoxidil, finasteride) and depigmentation agents8-10(hydroquinone) which are perceived as more for cosmetic benefits. Medications (acitretin and methoxalen) that require vigilant long term monitoring was utilised less in the private sector because patients requiring these agents were often referred to government hospitals for management. There was a high usage of the moderately potent and very potent topical steroids1-7 by private health care providers. The appropriateness of these prescriptions and monitoring of their side effects1-7 need further study. Similarly the usage of topical antibiotics was more in the private sector as compared to public sector. Here again, the appropriateness of topical antibiotic prescriptions and the drug resistance pattern need further study. Healthcare providers need to be aware of untoward events1-11 that can occur with inappropriate drug usage. 43 CHAPTER 11 USE OF DERMATOLOGICALS Malaysian Statistics on Medicines 2006 Table A: Utilisation of Medicament by Health Care Providers 2006 Increased medicament usage Increased medicament usage in Public Health Facilities in Private Health Facilities Topical Anti-fungal medicaments Nystatin, Miconazole Ketoconazole Isoconazole, Econazole, Terbinafine, Fluconazole Anti-psoriatic therapy Acitretin, Methoxalen Antibiotic & Antiseptics Neomycin, Silver sulfadiazine Antiviral Corticosteroids Hydrocortisone Combination Topical steroid and Antibiotic (AB)/antifungal Hydrocortisone plus AB Medicament used in Private Health Facilities only Calcipotriol combination therapy Tetracycline, Fusidic acid, Gentamicin, Mupirocin Topical aciclovir Clobetasone, Triamcinolone Betametasone, Mometasone Hydrocortisone aceponate, clobetasol Bethamethasone AB combination Bethamethasone plus other combination Anti-acne Adapalene, clindamycin, Azelaic acid Hair growth stimulants Depigmenting agent Calcineurin inhibitors Acne rosacea therapy Finasteride Hydroquinone Tacrolimus and pimecrolimus Tromantadine, Imiquimod Aclometasone, Dexamethasone Fluocinolone acetonide, Fluticasone Prednisolone plus AB, Triamcinolone/dexamethasone plus AB, Fluocinolone acetonide/clobetasol plus AB, Hydrocortisone plus other combination Topical isotretinoin Topical erythromycin and erythromycin combination Topical minoxidil Topical metronidazole Table 11.1: Use of Dermatological by Drug Class and Agents, in total dosage/1000 population/day 2006 ATC D01A A Drug Class and Agents Antibiotics Unit D01A A01 Nystatin g/ml/cc D01A C Imidazole and triazole derivatives D01A C01 Clotrimazole D01A C02 D01 A C03 D01A C05 D01A C07 D01A C08 g/ml/cc Miconazole g/ml/cc Econazole g/ml/cc Isoconazole g/ml/cc Tioconazole g/ml/cc Ketoconazole g/ml/cc 44 2006 Public 0.1064 Private 0.0089 Total 0.1153 Public 0.1469 Private 0.3403 Total 0.4872 Public 1.3178 Private 0.6315 Total 1.9493 Public - Private 0.0434 Total 0.0434 Public - Private 0.0003 Total 0.0003 Public 0.0007 Private 0.0059 Total 0.0066 Public 0.0608 Private 0.3199 Total 0.3808 CHAPTER 11 USE OF DERMATOLOGICALS Malaysian Statistics on Medicines 2006 ATC Drug Class and Agents Unit D01A C15 Fluconazole g/ml/cc D01A C20 D01A C52 Combinations Miconazole, combinations D01A E Other antifungals for topical use D01A E13 Selenium sulfide D01A E15 D01A E16 g/ml/cc g/ml/cc g/ml/cc Terbinafine g/ml/cc Amorolfine g/ml/cc 2006 Public - Private 0.0002 Total 0.0002 Public 0.0051 Private 1.7155 Total 1.7207 Public - Private 0.0229 Total 0.0229 Public 0.032 Private 0.0388 Total 0.0707 Public - Private 0.0277 Total 0.0277 Public 0.0001 Private <0.0001 Total 0.0002 Table 11.2: Use of Dermatological by Drug Class and Agents, in DDD/1000 population/day 2006 ATC Drug Class and Agents 2006 D01B A Antifungals for systemic use D01B A01 D01B A02 Griseofulvin Terbinafine Public 0.1525 Private 0.231 Total 0.3835 Public 0.0048 Private 0.0081 Total 0.0128 Table 11.3: Use of Dermatological by Drug Class and Agents, in total dosage/1000 population/day ATC D05A D Drug Class and Agents Psoralens for topical use Unit D05A D02 Methoxsalen g/ml/cc D05A X Other antipsoriatics for topical use D05A X02 Calcipotriol D05A X52 g/ml/cc Calcipotriol, combinations g/ml/cc 45 2006 Public 0.0003 Private 0.0001 Total 0.0004 Public 0.0465 Private 0.0124 Total 0.0589 Public - Private 0.0064 Total 0.0064 CHAPTER 11 USE OF DERMATOLOGICALS Malaysian Statistics on Medicines 2006 Table 11.4: Use of Dermatological by Drug Class and Agents, in DDD/1000 population/day 2006 ATC Drug Class and Agents 2006 D05B A Psoralens for systemic use D05B A02 Methoxsalen D05B B Retinoids for treatment of psoriasis D05B B01 Etretinate D05B B02 Acitretin Public 0.0012 Private 0.0007 Total 0.002 Public - Private - Total - Public 0.006 Private 0.0004 Total 0.0064 Table 11.5: Use of Dermatological by Drug Class and Agents, in total dosage/1000 population/day 2006 ATC D06A A Drug Class and Agents Tetracycline and derivatives Unit D06A A04 Tetracy cline g/ml/cc D06A X Other antibiotics for topical use D06A X01 Fusidic acid D06A X04 D06A X07 D06A X09 g/ml/cc Neomycin g/ml/cc Gentamicin g/ml/cc Mupirocin g/ml/cc 2006 Public - Private 0.0041 Total 0.0041 Public 0.0303 Private 0.2682 Total 0.2985 Public 0.8132 Private 0.2511 Total 1.0644 Public 0.0116 Private 0.2203 Total 0.2319 Public 0.0255 Private 0.0896 Total 0.1151 Table 11.6: Use of Dermatological by Drug Class and Agents, in total dosage/1000 population/day 2006 ATC D06B A Drug Class and Agents Sulfonamides Unit D06B A01 Silver sulfadiazine g/ml/cc D06B B Antivirals D06B B02 Tromantadine D06B A Sulfonamides D06B B03 Aciclovir g/ml/cc g/ml/cc 46 2006 Public 0.1782 Private 0.0919 Total 0.2701 Public - Private 0.0054 Total 0.0054 Public 0.002 Private 0.0588 Total 0.0608 CHAPTER 11 USE OF DERMATOLOGICALS Malaysian Statistics on Medicines 2006 ATC Drug Class and Agents Unit D06B B10 Imiquimod g/ml/cc D06B X Other chemotherapeutics D06B X01 Metronidazole g/ml/cc 2006 Public - Private 0.0003 Total 0.0003 Public - Private 0.0113 Total 0.0113 Table 11.7: Use of Dermatological by Drug Class and Agents, in total dosage/1000 population/day 2006 ATC D07A A Drug Class and Agents Corticosteroids, weak (group I) Unit D07A A02 Hydrocortisone g/ml/cc D07A B Corticosteroids, moderately potent (group II) D07A B01 Clobetasone D07A B03 D07A B09 D07A B10 D07A B19 Flumetasone g/ml/cc Alclometasone g/ml/cc Dexamethasone Corticosteroids, potent (group III) D07A C01 Betamethasone g/ml/cc g/ml/cc Fluocinolone acetonide D07A C Corticosteroids, potent (group III) D07A C13 Mometasone D07A C16 g/ml/cc Triamcinolone D07A C D07A C04 g/ml/cc g/ml/cc g/ml/cc Hydrocortisone aceponate g/ml/cc 47 2006 Public 1.0887 Private 0.6583 Total 1.747 Public 0.0491 Private 0.0622 Total 0.1113 Public 0.0002 Private - Total 0.0002 Public 0.0013 Private 0.085 Total 0.0863 Public - Private 0.0001 Total 0.0001 Public - Private 0.0005 Total 0.0005 Public 0.8813 Private 1.3885 Total 2.2698 Public - Private 0.0276 Total 0.0276 Public 0.0168 Private 0.0951 Total 0.1119 Public 0.0005 Private 0.0083 Total 0.0088 CHAPTER 11 USE OF DERMATOLOGICALS Malaysian Statistics on Medicines 2006 ATC Drug Class and Agents Unit D07A C17 Fluticasone g/ml/cc D07A D Corticosteroids, very potent (group IV) D07A D01 Clobetasol g/ml/cc 2006 Public - Private 0.0182 Total 0.0182 Public 0.0583 Private 0.5533 Total 0.6116 Table 11.8: Use of Dermatological by Drug Class and Agents, in total dosage/1000 population/day 2006 ATC D07C A Drug Class and Agents Unit Corticosteroids, weak, combinations with antibiotics D07C A01 Hydrocortisone and antibiotics D07C A03 g/ml/cc Prednisolone and antibiotics g/ml/cc 2006 Public 0.0573 Private 0.0407 Total 0.0981 Public - Private 0.0006 Total 0.0006 D07C B Corticosteroids, moderately potent, combinations with antibiotics D07C B01 Triamcinolone and antibiotics D07C B04 g/ml/cc Dexamethasone and antibiotics g/ml/cc D07C C Corticosteroids, potent, combinations with antibiotics D07C C01 Betamethasone and antibiotics D07C C02 D07C D01 g/ml/cc Fluocinolone acetonide and antibiotics g/ml/cc Clobetasol and antibiotics g/ml/cc Public - Private 0.049 Total 0.049 Public - Private 0.0015 Total 0.0015 Public 0.0198 Private 0.6038 Total 0.6235 Public - Private 0.0016 Total 0.0016 Public - Private 0.0013 Total 0.0013 Table 11.9: Use of Dermatological by Drug Class and Agents, in total dosage/1000 population/day 2006 ATC D07X A Drug Class and Agents Corticosteroids, weak, other combinations Unit D07X A01 Hydrocortisone g/ml/cc Public Private Total 0.0313 0.0313 D07X C Corticosteroids, potent, other combinations D07X C01 Betamethasone g/ml/cc Public Private Total 0.004 0.1847 0.1887 48 2006 CHAPTER 11 USE OF DERMATOLOGICALS Malaysian Statistics on Medicines 2006 Table 11.11: Use of Dermatological by Drug Class and Agents, in total dosage/1000 population/day 2006 ATC D10A D Drug Class and Agents Retinoids for topical use in acne Unit D10A D01 Tretinoin g/ml/cc D10A D03 Adapalene g/ml/cc D10A D04 Isotretinoin g/ml/cc D10A E01 Benzoyl peroxide g/ml/cc D10A F Antiinfectives for treatment of acne D10A F01 Clindamycin Public Private Total Public Private Total Public Private Total Public Private Total 0.0358 0.035 0.0708 0.0002 0.0357 0.0359 0.0031 0.00 31 0.0002 0.0002 g/ml/cc Public Private Total 0.0002 0.0894 0.0896 Public Private Total Public Private Total 0.0384 0.0384 0.0029 0.0029 Public Private Total 0.0007 0.012 0.0128 D10A F Antiinfectives for treatment of acne D10A F02 Erythromycin g/ml/cc D10A F52 Erythromycin, combinations g/ml/cc D10A X Other anti-acne preparations for topical use D10A X03 Azelaic acid 2006 g/ml/cc Table 11.12: Use of Dermatological by Drug Class and Agents, in DDD/1000 population/day 2006 ATC D10B A Drug Class and Agents Retinoids for treatment of acne D10B A0 1 Isotretinoin 2006 Public Private Total 0.01 0.0073 0.0173 Table 11.13: Use of Dermatological by Drug Class and Agents, in total dosage/1000population/day 2006 ATC D11A C Drug Class and Agents Medicated shampoos Unit D11A C03 Selenium compounds g/ml/cc Public Private Total 0.0604 0.1091 0.1695 D11A X Other dermatologicals D11A X01 Minoxidil g/ml/cc D11A X10 Finasteride mg Public Private Total Public Private Total 0.0231 0.0231 0.0012 0.0989 0.1001 49 2006 CHAPTER 11 USE OF DERMATOLOGICALS Malaysian Statistics on Medicines 2006 ATC Drug Class and Agents Unit D11A X11 Hydroquinone g/ml/cc D11A X14 Tacrolimus g/ml/cc D11A X Other dermatologicals D11A X15 Pimecrolimus g/ml/cc 2006 Public Private Total Public Private Total <0.0001 0.0119 0.012 0.0005 0.0098 0.0103 Public Private Total <0.0001 0.0019 0.002 References: 1. Rajesh B et al. Factors affecting prescription of ultra-high potency topical corticosteroids in skin disease: an analysis of US national practice data Journal of Drugs of Dermatology, Nov.-Dec. 2005. 2. MA Al-Dhalimi and, N. Aljawahiry. Misuse of topical corticosteroids: a clinical study in an Iraqi hospital Eastern Mediterranean Health Journal Volume 12 No 6 November 2006 Griffiths WAD, Wilkinson JD. Topical therapy. In: Champion RH et al. Textbook of dermatology, vol. 4. 6th ed. Oxford, Blackwell Science, 1998:3547-52. 3. Sulzberger MB, Witten VH. The effect of topically applied compound F in selected dermatoses. Journal of investigative dermatology, 1952, 19(2):101-2. 4. Lagos B, Maibach H. Frequency of application of topical corticosteroids: an overview. British journal of dermatology, 1998, 139(5):763-6. 5. Brodkin RH, Janniger CK. The artful use of topical steroids. Cutis, 1998, 61(3):125-6. 6. Keane FM et al. Unregulated use of clobetasol propionate. British journal of dermatology, 2001, 144(5):1095-6. 7. Fleischer AB Jr, Ford PG. How to prevent side-effects of topical corticosteroids. Skin and aging, 1998, February: 54-65. 8. Mahe A et al. Skin diseases associated with the cosmetic use of bleaching products in women from Dakar, Senegal. British journal of dermatology, 2003, 148(3):493-500. Arnold J, Anthonioz P, Marchand JP. Depigmenting action of corticosteroids. Dermatologica, 1975, 151(5):274-80. 9. Del Giudice P, Pinier Y. The widespread use of skin lightening creams in Senegal: a persistent health problem in West Africa. International journal of dermatology, 2002, 41(2):69-72. 10. Hammarstrom et al. Pharmaceutical care for patients with skin diseases: a campaign year at Swedish pharmacies. Journal of Clinical Pharmacy and Therapeutics, 1995, 20(6):327-334. 50 CHAPTER 12: USE OF GYNAECOLOGICALS, SEX HORMONES AND HORMONAL CONTRACEPTIVES Malaysian Statistics on Medicines 2006 Edited by: Muralitharan G1, Tan AL2 1. Ampang Hospital, 2. Kuala Lumpur Hospital There has been very little review on the use of gynaecological, hormone and hormonal contraceptive drugs in Malaysian literature. Obstetrics and Gynaecology have altered their pharmacotherapeutic usage in recent times. This is due to various factors. Firstly, what was thought to be first line management is currently not effective therapeutically and has therefore been abandoned and newer drugs introduced. Secondly, newer therapies have been introduced for common Obstetric and Gynaecological problems which are not addressed in Table 12.1. Thirdly, hormonal therapies have changed with newer hormonal drugs where the hormones are more closely associated with the biochemical nature of natural hormones. In the management of preterm labour, the drug of choice as a tocolytic agent has changed recently to ritodrine. However there is level A evidence that Atosiban and Nifedipine appear to be preferable as they have fewer adverse effects and comparable effectiveness. [1] These drugs will need to be looked into in future reviews. Antenatal corticosteroid therapy is an established evidence based therapy which has been associated with reduction in respiratory distress syndrome of the newborn. [2] Corticosteroids for this indication have also not been addressed in Table 12.1. Similarly, the diagnosis of preterm rupture of membranes is often difficult to ascertain. There are various new tools that are available that have not been evaluated in Malaysia and are therefore not widely used. Amniosure, a device that is FDA approved and which claims sensitivity and specificity of more than 90% will need to be evaluated for usage in Malaysia. Actin Prom and Actin Partus, devices that are widely used in first world countries in the diagnosis of preterm labour and labour need to be evaluated in future for use in Malaysia. In the management of hypertensive disease complicating pregnancy and eclampsia, the use of Magnesium Sulphate is now an integral component. [3] This needs to be addressed in future reviews of this nature. Similarly thoromboprophylactic drugs both low molecular weight heparin and conventional heparin is now widely utilised in Obstetric and Gynaecological practice. They need to be evaluated in future undertakings of this nature. Metformin therapy is now encouraged in the management of polycystic ovarian syndrome. [4] This needs to be addressed in Chapter 12. Similarly, pelvic inflammatory disease is an increasing problem in the community today. Chlamydia is an organism associated with pelvic inflammatory disease and Azithromycin is the drug of choice. Similarly, with the current increase in assisted reproductive techniques, the use of ovulatory drugs ranging from GnRH analogues and purified FSH derivatives to conventional therapy such as Clomiphene Citrate and Tamoxifen need to be addressed in future reviews. Surgical management of subfertile patients is now supplemented with the use of substances which aid in preventing adhesions which is an important cause of subfertility. Drug therapy for the management of endometriosis and subfertility is now closely associated and drugs used for the first condition are often supplemented with drugs for the subfertility. [5] Review of Table 12.2.2 reveals that there are drugs where there is a disparity in its usage in the public and private sector. The disparity is largely in the use of drugs which are expensive. There is also evidence that synthetic hormonal therapy and selective estrogen receptor modulators for menopausal women is underutilised within the public sector. In conclusion, there is a need to relook at drugs categorised under gynaecological and hormonal usage. A lot of the drugs are now not commonly used by practicing gynaecologists and have been replaced by newer drugs. The next review will need to update the use of these drugs and will need to look at medical devices that are now part of daily Obstetrics and Gynaecology practice. 51 Malaysian Statistics on Medicines 2006 CHAPTER 12: USE OF GYNAECOLOGICALS, SEX HORMONES AND HORMONAL CONTRACEPTIVES Table 12.1: Use of Gynaecologicals, Sex Hormones and Hormonal Contraceptives, in DDD/1000 population/day 2006 ATC Drug Class 2006 G01 G02 G03 GYNECOLOGICAL ANTIINFECTIVES AND ANTISEPTICS OTHER GYNECOLOGICALS SEX HORMONES AND MODULATORS OF THE GENITAL SYSTEM 0.2119 0.0947 10.7433 Table 12.2.1: Use of Gynaecologicals, Sex Hormones and Hormonal Contraceptives by Drug Class, in DDD/1000 population/day 2006 ATC Drug Class and Agents 2006 G01A G01A A G01A F G02A G02A B G02A D G02C G02C A G02C B G0 2C X G03A G03A A G03A B G03A C G03B G03B A G03B B G03C G03C A G03D G03D A G03D B G03D C G03F G03F A G03F B G03G G03G A G03G B G03H G03H A G03H B G03X G03X A G03X C ANTIINFECTIVES AND ANTISEPTICS, EXCL. COMBINATIONS WITH CORTICOSTEROIDS Antibiotics Imidazole derivatives OXYTOCICS Ergot alkaloids Prostaglandins OTHER GYNECOLOGICALS Sympathomimetics, labour repressants Prolactine inhibitors Other gynecologicals HORMONAL CONTRACEPTIVES FOR SYSTEMIC USE Progestogens and estrogens, fixed combinations Progestogens and estrogens, sequential preparations Progestogens ANDROGENS 3-oxoandrosten (4) derivatives 5-androstanon (3) derivatives ESTROGENS Natural and semisynthetic estrogens, plain PROGESTOGENS Pregnen (4) derivatives Pregnadien derivatives Estren derivatives PROGESTOGENS AND ESTROGENS IN COMBINATION Progestogens and estrogens, fixed combinations Progestogens and estrogens, sequential preparations GONADOTROPINS AND OTHER OVULATION STIMULANTS Gonadotropins Ovulation stimulants, synthetic ANTIANDROGENS Antiandrogens, plain Antiandrogens and estrogens OTHER SEX HORMONES AND MODULATORS OF THE GENITAL SYSTEM Antigonadotropins and similar agents Selective estrogen receptor modulators 52 0.2119 0.0648 0.147 0.0515 0.0059 0.0457 0.0431 0.0218 0.0213 <0.0001 8.7254 3.9443 0.0388 4.7423 0.0267 0.0245 0.0022 0.1336 0.1336 1.0514 0.367 0.1996 0.4848 0.1935 0.0794 0.1141 0.3619 0.0342 0.3277 0.0964 0.013 0.0834 0.1544 0.0251 0.1293 CHAPTER 12: USE OF GYNAECOLOGICALS, SEX HORMONES AND HORMONAL CONTRACEPTIVES Malaysian Statistics on Medicines 2006 Table 12.2.2: Use of Gynaecologicals, Sex Hormones and Hormonal Contraceptives by Drug Class and Agents, in DDD/1000 population/day 2006 ATC Drug Class and Agents 2006 G01A A G01A A01 Antibiotics Nystatin G01A A03 Amphotericin B G01A A10 Clindamycin G01A F G01A F01 Imidazole derivatives Metronidazole G01A F02 Clotrimazole G01A F04 Miconazole G01A F05 Econazole G01A F08 Tioconazole G01A F11 Ketoconazole G02A B G02A B01 Ergot alkaloids Methylergometrine G02A B03 Ergometrine G03D C02 Norethisterone G03D C05 Tibolone G03F A G03F A01 Progestogens and estrogens, fixed combinations Norethisterone and estrogen G03F A12 Medroxyprogesterone and estrogen 53 Public Private Total Public Private Total Public Priva te Total 0.0596 0.004 0.0636 0.0012 0.0012 <0.0001 <0.0001 Public Private Total Public Private Total Public Private Tota l Public Private Total Public Private Total Public Private Total 0.0539 0.0003 0.0543 0.0216 0.0579 0.0795 0.0035 0.0035 0.0069 0.0069 0.0024 0.0024 0.0004 0.0004 Public Private Total Public Private Total Public Private Total Public Private Total 0.0025 0.0025 0.003 0.0004 0.0034 0.0223 0.2787 0.301 0.1063 0.0705 0.1768 Public Private Total Public Private Total 0.0135 0.0183 0.0318 0.0279 0.0023 0.0302 Malaysian Statistics on Medicines 2006 CHAPTER 12: USE OF GYNAECOLOGICALS, SEX HORMONES AND HORMONAL CONTRACEPTIVES ATC Drug Class and Agents G03F A14 Dydrogesterone and estrogen 2006 G03F B G03F B01 Progestogens and estrogens, sequential preparations Norgestrel and estrogen G03F B05 Norethisterone and estrogen G03F B06 Medroxyprogesterone and estrogen G03F B07 Medrogestone and estrogen G03F B08 Dydrogesterone and estrogen G03G A G03G A01 Gonadotropins Chorionic gonadotrophin G03G A02 Human menopausal gonadotrophin G03G A05 Follitropin alfa G03G A06 Follitropin beta G03G A07 Lutropin alfa G03G A08 Choriogonadotropin alfa G03G B G03G B02 Ovulation stimulants, synthetic Clomifene G03H A G03H A01 Antiandrogens, plain Cyproterone G03H B G03H B0 1 Antiandrogens and estrogens Cyproterone and estrogen 54 Public Private Total 0.0103 0.007 0.0173 Public Private Total Public Private Total Public Private Total Public Private Total Public Private Total 0.0709 0.0155 0.0864 <0.0001 0.0014 0.0014 0.0244 0.0003 0.0247 0.0006 0.0006 0.001 0.001 Public Private Total Public Private Total Public Private Total Public Private Total Public Private Total Public Private Total 0.0122 0.0183 0.0305 0.0003 0.0003 0.0009 0.0008 0.0018 0.0007 0.0009 0.0016 <0.0001 <0.0001 <0.0001 <0.0001 Public Private Total 0.1178 0.2098 0.3277 Public Private Total 0.0111 0.0019 0.013 Public Private Total 0.0116 0.0718 0.0834 CHAPTER 12: USE OF GYNAECOLOGICALS, SEX HORMONES AND HORMONAL CONTRACEPTIVES ATC Drug Class and Agents G03X A G03X A01 Antigonadotropins and similar agents Danazol G03X A02 Gestrinone G03X C G03X C01 Selective estrogen receptor modulators Raloxifene Malaysian Statistics on Medicines 2006 2006 Public Private Total Public Private Total 0.0156 0.008 0.0237 0.0012 0.0003 0.0014 Public Private Total 0.0646 0.0647 0.1293 References: 1. Royal College of Obstetricians and Gynaecologists. Tocolytic Drugs For Women in Preterm Labour. Clinical Guideline No. 1 (B) October 2002. 2. Royal College of Obstetricians and Gynaecologists. Antenatal Corticosteroids To Prevent Respiratory Distress Syndrom. Guideline No. 7 Revised February 2004. 3. Royal College of Obstetricians and Gynaecologists. The Management of Severe Pre-Eclampsia/Eclampsia. Guideline No. 10 (A) March 2006. 4. Royal College of Obstetricians and Gynaecologists. Long-Term Consequences of Polycystic Ovary Syndrome. Green-top Guideline No. 33 December 2007. 5. Royal College of Obstetricians and Gynaecologists. The Investigation and Management of Endometriosis. Green-top Guideline No. 24 October 2006. 55 CHAPTER 13 USE OF UROLOGICALS Malaysian Statistics on Medicines 2006 Edited by: Malek R1, Lei CM2, Subaratnam S1, Syarihan S1 1. Selayang Hospital 2. Normah Hospital, Kuching Although urology started as a surgical specialty, medicines play an expanding role in the management of urological disease. Medicines in urology may be discussed under the following drug class: (a) Drugs used for overactive bladder, OAB: The oldest drug is Flavoxate, with rather non specific and weak anti-cholinergic action. The anti-cholinergic of choice is currently Tolterodine, reflected in its increased usage. However, there are newer anti-cholinergics with less side effects of dry mouth. When the newer agents are duly registered, it is likely to increase in usage, as seen in other countries. (b) Drugs used in erectile dysfunction: The oral prostagladin type 5 inhibitors, namely Sildenafil, Tadalafil and Vardenafil are introduced at different stages in Malaysia. It is therefore not unexpected the earlier drug, namely, Sildenafil has a bigger usage. Experience in other countries showed that the 3 drugs have almost an equal share. Alprostadil is actually an injectable although put in the same group. The usage is reported as very low. Nevertheless, this has more or less replaced Papaverine as the first line intracorporeal injection for penile erection. Alprostadil have a small but definite role in the treatment of erectile dysfunction. (c) Alpha-adrenoreceptor antagonists: There are 3 main drugs in this group used for relief of bladder outlet obstruction. Only the extended release (XL) form of Alfuzosin is available. For Doxazosin, both the extended release (XL) as well as the rapid release lower dosage is available. For Terazosin, only the rapid release incremental dosages (1, 2, 5 mg) are available. It is likely that the drug usage reported refers to the optimal dosage and not the starting dosage of this alpha-adrenoreceptor antagonist. (d) 5-alpha reductase inhibitors: There are currently 2 drugs in this class, namely, Finasteride and Dutasteride. Finasteride has been in use for more than 10 years and currently, the generic forms are available. Therefore, it is not surprising that usage of Finasteride is more than that of Dutasteride. (e) Gonadotrophin releasing hormone analogues: In urology, these drugs are used to inhibit the production of testosterone by the testes, as a treatment for advanced prostate cancer. This includes Buserelin, Leuprorelin, Goserelin and Triptorelin. Again, they are short acting as well as depot versions (with action ranging from 3 to 12 months). They are also used by the gynaecologists and the total usage probably covers both usages. (f) Anti-estrogens: These include Flutamide, Bicalutamide and Cyproterone Acetate. For some patients with prostate cancer, anti-androgens are added onto the gonadotrophin release hormone analogues for maximal androgen blockage (MAB). This is to block the action of hormones from the adrenal glands. (g) Selective immunosuppressive agents for metastatic kidney cancer: This new group of drugs includes Etanercept, Infliximab, Leflunomide, Efalizumab. These are new drugs which have shown some efficacy for metastatic renal cancer. They are often used by the urologists together with the medical oncologists. In view of the high cost, it is probable that the reported usage from the present survey is an underestimate as they are likely to be used in the private hospitals. (h) Testosterone: Testosterone is increasing used in the field of men’s health. A recent survey showed that there is a 20% incidence of testosterone deficient syndrome in patients with metabolic syndrome. Again, these drugs are likely to be given by private specialists. 57 CHAPTER 13 USE OF UROLOGICALS Malaysian Statistics on Medicines 2006 (i) Anti-diuretic hormone: The commercial preparation of this is Desmopressin (Minirin). It is used mainly to treat nocturnal polyuria which is seen in paediatric patients with enuresis and in some elderly men. Table 13.1: Use of Urological, in DDD/1000 population/day 2006 ATC Drug Class and Agents 2006 G04 UROLOGICALS 0.7232 Table 13.2.1: Use of Urological by Drug Class, in DDD/1000 population/day 2006 ATC Drug Class and Agents 2006 G04B G04C OTHER UROLOGICALS, INCL. ANTISPASMODICS DRUGS USED IN BENIGN PROSTATIC HYPERTROPHY 0.2018 0.5214 Table 13.2.2: Use of Gynecological, Sex Hormones and Hormonal Contraceptives by Drug Class and Agents, in DDD/1000 population/day 2006 ATC G04B D Drug Class and Agents Urinary antispasmodics 2006 G04B D02 Flavoxate G04B D04 Oxybutynin G04B D07 Tolterodine G04B E Drugs used in erectile dysfunction G04B E01 Alprostadil G04B E03 Sildenafil G04B E08 Tadalafil G04B E09 Vardenafil G04C A Alpha-adrenoreceptor antagonists G04C A01 Alfuzosin G04C A03 Terazosin C02CA04 Doxazosin 58 Public Private Total Public Private Tota l Public Private Total 0.0002 0.0149 0.0151 0.0029 0.0003 0.0032 0.0159 0.006 0.0219 Public Private Total Public Private Total Public Private Total Public Private Total <0.0001 <0.0001 <0.0001 0.0011 0.1173 0.1184 0.0023 0.0364 0.0387 0.0001 0.0044 0.0045 Public Private Total Public Private Total Public Private Total 0.048 0.0506 0.0986 0.2885 0.0706 0.359 0.1764 0.0628 0.2393 CHAPTER 13 USE OF UROLOGICALS Malaysian Statistics on Medicines 2006 ATC G04C B Drug Class and Agents Testosterone-5-alpha reductase inhibitors G04C B01 Finasteride G04C B02 Dutasteride 2006 Public Private Total Public Private Total 0.03 0.0039 0.0339 0.0151 0.0148 0.0299 Table 13.2.3: Use of Urologicals listed in other chapters, Gonadotropin releasing hormone analogues, anti-androgens, selective immunosuppressive agents, hormones ATC L02A E Drug Class and Agents Gonadotropin releasing hormone analogues L02A E01 Buserelin L02A E02 Leuprorelin L02A E03 Goserelin L02A E04 Triptorelin L02B A Anti-oxoandrosten (4) derivatives L02B B01 Flutamide L02B B03 Bicalutamide Cyproterone acetate L04A A Selective immunosuppressive agents L04A A11 Etanercept L04A A12 Infliximab L04A A13 Leflunomide L04A A21 Efalizumab 59 2006 Public Private Total Public Private Total Public Private Tota l Public Private Total <0.0001 <0.0001 <0.0001 0.0024 0.0085 0.0109 0.0038 0.0021 0.0059 0.0011 0.0003 0.0015 Public Private Total Public Private Total Public Private Total 0.0018 0.0007 0.0025 0.0053 0.001 0.0063 0.0111 0.0919 0.3277 Public Private Total Public Private Total Public Private Total Public Private Total <0.0001 0.0009 0.001 <0.0001 0.0036 0.0037 0.0077 0.0069 0.0146 <0.0001 <0.0001 CHAPTER 13 USE OF UROLOGICALS Malaysian Statistics on Medicines 2006 ATC G03 G03B A Drug Class and Agents Sex Hormones 3-oxoandrosten (4) derivatives 2006 G03B A03 Testosterone H01B H01B A POSTERIOR PITUITARY LOBE HORMONES Vasopressin and analogues H01B A02 Desmopressin Public Private Total 0.0112 0.0133 0.0245 Public Private Total 0.0122 0.0037 0.0159 References: 1. “Prevalence of Symptomatic BPE Among Malaysian Men Aged 50 and Above Attending Screening During Prostate Health Awareness Campaign”. GC Teh, RM Sahabudin, TC Lim, WL Chong, S Woo, M Mohan, A Khairullah, P Abrams, Institute of Urology, Kuala Lumpur Hospital, Malaysia, Bristol Urological Institute, Southmead Hospital, Bristol, UK. 2. “Impotence Clinic in a Developing Country”. CCM Lei, V Manivannan, PKK Mah, PEP. Ng, A Khairullah International J Impotence Research (1994) 6, Suppl. 1, P113. 3. “Asian Sildenafil Efficacy and Safety Study (Assess-1): a double-blind, placebo-controlled, flexible-dose study of oral Sildenafil in Malaysian, Singaporean, and Filipino men with erectile dysfunction”. Tan HM, Lei CCM, Mendoza JB et al. Urology 56 (4): 635-640, 2000. 4. “Efficacy and tolerability of Vardenafil, an oral phosphodiesterase type-5 inhibitor, in Asian men with erectile dysfunction”. HM Tan, CM Chin, CB Chua, E Gatchalian, A Kongkanand, CCM Lei, FC Ng, K Ratana-Olarn, D Serrano, A Taher, I Tambi, A Tantiwong, M Wong, AWC Yip , Asian J Andrology 2008; 10(3) 495-502. 60 CHAPTER 14 USE OF MEDICINES FOR ENDOCRINE DISORDERS Malaysian Statistics on Medicines 2006 Edited by: Zanariah H1 With contributions from: Oiyammal C2, Nazri D3 1. Putrajaya Hospital, 2. Sungai Bakap Hospital, 3. Tampin Health Clinic The total consumption of endocrine related drugs in Malaysia for 2006 was 2.11DDD/1000 population/day. Among the endocrine related drugs, the most utilised were thyroid-related drugs (94.4%), followed by pituitary and hypothalamic hormone and analogues (5.3%) and drugs for calcium homeostasis (0.3%). In comparison, there was very much higher utilisation of endocrine-related drugs in Australia for 2006 at a level of 17.0DDD/1000 population/day, with a similar trend, the most common being thyroid related drugs (98.1%), followed by pituitary and hypothalamic hormone and analogues (1.87%) and drugs for calcium homeostasis (0.01%). Thyroid therapy consisted of drugs utilised for hypothyroidism and hyperthyroidism. For treatment of hypothyroidism, thyroid hormone replacement was almost entirely (99.99%) with Levothyroxine (T4) sodium at 0.93DDD/1000 population/day in comparison to a much higher consumption in Australia at 15.87DDD/1000 population/day. Use of Liothyronine (T3) Sodium in Australia was minimal at 0.05DDD/1000 population/day, consisting 0.3% of thyroid hormone replacement therapy. This thyroid hormone formulation was hardly utilised in Malaysia. Thyroid hormone consumption with Levothyroxine Sodium was more than 10-fold higher in Australia compared to Malaysia suggesting a higher prevalence of hypothyroidism, possibly related to better screening, diagnosis and treatment among the elderly population. For treatment of hyperthyroidism, consumption of anti-thyroid preparations were higher in Malaysia (1.06DDD/1000 population/day) compared to Australia (0.77DDD/1000 population/day) in 2006. The most utilised anti-thyroid preparation in Malaysia was Carbimazole (84.2%) followed by Propylthiouracil (15.8%). The higher anti-thyroid drug utilisation in Malaysia is probably related to a preference for first-line medical therapy in hyperthyroidism, often continued over the long-term as radioactive iodine facilities for treatment of hyperthyroidism is currently still limited in accessibility and usually placed as second-line therapy. The higher consumption of carbimazole is most probably due to the convenience of daily dosing as opposed to divided dosing for Propylthiouracil. Drug utilisation of pituitary and hypothalamic hormones and analogues were generally low in Malaysia at 0.11DDD/1000 population/day and similarly in Australia at 0.32DDD/1000 population/day. Consumption of drugs for calcium homeostasis was also low in Malaysia at 0.006DDD/1000 population/day and Australia at 0.001DDD/1000 population/day. These drugs include parathyroid hormone and analogues such as Teriparatide (0.0006DDD/1000 population/day) and Calcitonin preparations (0.006DDD/1000 population/day). There was a higher consumption of Calcitonin preparations in Malaysia compared to Australia (0.001DDD/1000 population/ day). Table 14.1: Use of Drug for Endocrine Disorders, in DDD/1000 population/day 2006 ATC Drug Class and Agents 2006 H01 PIT UITARY AND HYPOTHALAMIC HORMONES AND ANALOGUES THYROID THERAPY PANCREATIC HORMONES CALCIUM HOMEOSTASIS 0.1128 H03 H04 H05 61 1.9964 <0.0001 0.0064 Malaysian Statistics on Medicines 2006 CHAPTER 14 USE OF MEDICINES FOR ENDOCRINE DISORDERS Table 14.2: Use of Pituitary and Hypothalamic Hormones and Analogues by Drug Class, in DDD/1000 population/day 2006 ATC Drug Class and Agents 2006 H01A H01A A H01A B H01A C H01B H01B A H01B B H01C H01C B H01C C ANTERIOR PITUITARY LOBE HORMONES AND ANALOGUES ACTH Thyrotropin Somatropin and somatropin agonists POSTERIOR PITUITARY LOBE HORMONES Vaso pressin and analogues Oxytocin and analogues HYPOTHALAMIC HORMONES Antigrowth hormone Anti -gonadotropin-releasing hormones 0.009 0.0045 <0.0001 0.0045 0.1025 0.0191 0.0834 0.0013 0.0012 <0.0001 Table 14.3.1: Use of Thyroid Therapy by Drug Class, in DDD/1000 population/day 2006 ATC Drug Class and Agents H03A H03A A H03B H03B A H03B B THYROID PREPARATIONS Thyroid hormones ANTITHYROID PREPARATIONS Thiouracils Sulfur-containing imidazole derivatives 2006 0.9344 0.9344 1.062 0.1679 0.8941 Table 14.3.2: Use of Thyroid Therapy by Drug Class and Agents, in DDD/1000 population/day 2006 ATC Drug Class and Agents 2006 H03A A Thyroid hormones H03A A01 Levothyroxine sodium H03A A02 Liothyronine sodium H03B A Thiouracils H03B A02 Propylthiouracil H03B B Sulfur-containing imidazole derivatives H03B B01 Carbimazole Public Private Total Public Private Total 0.7504 0.1839 0.9343 <0.0001 <0.0001 <0.0001 Public Private Total 0.0872 0.0808 0.1679 Public Private Total 0.611 0.2831 0.8941 Table 14.4.1: Use of Calcium Homeostasis by Drug Class, in DDD/1000 population/day 2006 ATC Drug Class and Agents H05A H05A A H05B H05B A PARATHYROID HORMONES AND ANALOGUES Parathyroid hormones and analogues ANTI-PARATHYROID AGENTS Calcitonin preparations 62 2006 0.0006 0.0006 0.0058 0.0058 CHAPTER 14 USE OF MEDICINES FOR ENDOCRINE DISORDERS Malaysian Statistics on Medicines 2006 Table 14.4.2: Use of Thyroid Therapy by Drug Class, in DDD/1000 population/day 2006 ATC H05A A Drug Class and Agents Parathyroid hormones and analogues H05A A02 Teriparatide H05B A Calcitonin preparations H05B A01 Calcitonin (salmon synthetic) 2006 Public Private Total <0.0001 0.0005 0.0006 Public Private Total 0.0044 0.0013 0.0058 References: 1. Australian Statistics on Medicine 2006. Commonwealth Department of Health and Ageing Australia. 63 CHAPTER 15 USE OF ANTIINFECTIVES Malaysian Statistics on Medicines 2006 Edited by: Masrahayu M1, Ngau YY2, Thong KS3, Sameerah SAR4, Jacqueline L5, Rahela AK4 1. Selayang Hospital, 2. Kuala Lumpur Hospital, 3. Raja Permaisuri Bainun Hospital, Ipoh, 4. Pharmaceutical Services Division, MOH, 5. Tawau Hospital The most commonly prescribed antiinfectives in 2006 were Antibacterials (8.94DDD/1000population/day), followed by Antimycobacterials (1.10), Antivirals for systemic use (0.56), Antimycotic for systemic use (0.33) and Antimalarials (0.08). Among the classes of antibacterials prescribed, Penicillins were most commonly used constituting 47.1% of total use of antibacterials, followed by Macrolides, Lincosamides and Streptogramins group (15.5%), Tetracyclines (12.3%), other Beta-lactam Antibacterials (10.7%), Sulfonamide and Trimethoprim (8.6%), Quinolones (4.3%), other antibacterial (0.85%), Aminoglycoside (0.51%) and Amphenicol (0.05%). Among the penicillin class, penicillins with extended spectrum were most commonly prescribed (2.52DDD/1000 population/day) constituting 59.7% of total use. Beta-lactamase resistant penicillins, penicillin combinations with beta-lactamase inhibitors and beta-lactamase sensitive penicillin constituted 19.2%, 15.9% and 5.2% of penicillin use respectively. Results also showed that Amoxicillin was the highest antibiotic used in the penicillin group for both public (0.7) and private (1.4) sectors. Cephalosporins constituted 8.8% of total antibacterial use. The first and second generation cephalosporins were the most used and use between both groups were comparable with 0.42 and 0.43DDD/1000 population/day respectively. The first-generation group constituted 44.6% of total cephalosporin use followed by the second-generation group (45.2%), the 3rd generation (8.1%) and 4th generation (2.0%). Cefalexin (0.37DDD/1000 population/day) was the most widely prescribed cephalosporin followed by cefuroxime (0.36) and cefadroxil (0.05). Ceftriaxone was the most widely prescribed third-generation cephalosporin with 0.04DDD/1000 population/day. The Carbapenems constituted 0.17% of total antibacterial use. Meropenem use (44.3%) was near equal proportion in use with imipenem (43.8%). Ertapenem was the least prescribed carbapenem but its consumption was predominantly in the private sector. Sulphonamides and trimethoprim constituted 8.6% of antibacterial use and the combination Sulfamethoxazole and trimethoprim was the highest used in this group (66.2%). For Macrolides, erythromycin was most widely prescribed (0.94), followed by clarithromycin (0.19) and roxithromycin (0.12). For tetracyclines, doxycycline (0.92) was most commonly prescribed, followed by tetracycline (0.15) and minocycline (0.03). For quinolones, ciprofloxacin (0.14) was the most commonly prescribed, followed by ofloxacin (0.11) and norfloxacin (0.08). Vancomycin was the most frequently prescribed glycopeptide antibiotic, almost ten-fold higher than teicoplanin. Vancomycin consumption was higher in the public sector. Among the antifungals, ketoconazole (0.24DDD/1000 population/day) was the most frequently prescribed, followed by itraconazole (0.05) and fluconazole (0.03). Amphotericin B was rarely prescribed and so was flucytosine, caspofungin and voriconazole. Ketoconazole (95%) and fluconazole (58%) was more frequently prescribed in the private sector, amphotericin B (93%) mainly by the public sector while itraconazole consumption was almost equal in both the public and private sectors. Among the anti-mycobacterials, isoniazid (0.46DDD/1000 population/day)) was the most frequently prescribed followed by rifampicin (0.3), pyrazinamide (0.12) and ethambutol (0.11). Usage of these drugs was predominantly in the public sector. Usage of second-line anti-mycobacterial drugs was relatively infrequent. Aminoquinolones were the most commonly prescribed anti-protozoal drugs (0.06DDD/1000 population/day), of which primaquine was the most frequently prescribed agent (52%) followed by hydroxychloroquine (28%). For the antivirals, nucleoside and nucleotide reverse transcriptase inhibitors (0.18DDD/1000 population/day) were the most commonly prescribed agents (36.4% of total drugs used), followed by neuraminidase inhibitors (0.15). Oseltamivir (0.125) was the most commonly prescribed antiviral, followed by lamivudine (0.116) 65 CHAPTER 15 USE OF ANTIINFECTIVES Malaysian Statistics on Medicines 2006 and aciclovir (0.047). While Oseltamivir was predominantly prescribed by the public sector, lamivudine was more commonly used in the private sector. Antibacterial use in Malaysia (8.94DDD/1000 population/day)) is lower when compared to the United States (24.92), Europe (19.04) and British Columbia (17.9) [1,2]. It is however comparable to countries with relatively lower antibiotic consumption such as Austria (12.5), Latvia (11.7) and the Netherlands (9.78). Antibiotic use in Malaysia was also lower than Greece (31.4), France (28.97), Luxembourg (27.34), Hungary (19.63) and Slovenia (17.1) [3]. The most frequently prescribed class of antibacterials in Malaysia was penicillins (J01C) and this was also the case for the United States and Europe. However, consumption of penicillins was twice as much in the United States (9.70) and Europe (8.71) as compared to Malaysia (4.21). Among the penicillin subclasses, penicillins with extended spectrum (2.51) were the most frequently prescribed in Malaysia, similar to the United States (5.68) and Europe (4.49) [2]. Amoxicillin was the most commonly prescribed antibacterial agent in Malaysia (2.10) and this was also similar to the United States (5.59) and Europe (4.26). However, amoxicillin consumption in Malaysia was lower than the lowest DDD in Europe, the Netherlands (3.76). The second most common antibacterial agent prescribed in Malaysia was erythromycin (0.94DDD/1000 population/day)) as compared to co-amoxiclav which was the second most commonly prescribed antibacterial agent in the United States and Europe. The third most common antibacterial agent prescribed in Malaysia was doxycycline (0.92), which was similar to United States and Europe. Erythromycin was the most common macrolide prescribed in Malaysia while in the United States and Europe, azithromycin was the more popular macrolide. Cloxacillin (0.8DDD/1000 population/day) was the fourth most common antibacterial agent prescribed in Malaysia. For the fluroquinolone group, levofloxacin was most commonly prescribed in the United States and Europe, while ciprofloxacin was the most commonly prescribed quinolone in Malaysia. The use of antimicrobial agents particularly its overuse and misuse, is the major driver of antimicrobial resistance (4). Information on the trends and patterns of antibiotic consumption is essential to formulate control measures on antibiotic prescribing, although this is mainly feasible in the public sector. The National Antibiotic Guideline 2008 a publication of the Ministry of Health Malaysia will serve as an important tool towards rational prescribing of antibiotics. Antimicrobial stewardship programs in concert with aggressive infection control efforts represent the best chance for control of resistant pathogens. Stopping antibacterials when they are not needed, switching to more narrow spectrum drug regimens, and optimal dosing using pharmacokinetic and pharmacodynamic principles are critical (5, 6). In conclusion, antibacterial agents were the most commonly prescribed antiinfective agent in Malaysia and amoxicillin was the most frequently prescribed antibiotic. There were significant prescribing differences between the government and private sectors, with the private sector consuming more beta-lactam/beta-lactamase combinations, roxithromycin, clarythromycin and cefalexin. Table 15.1: Use of Anti-Infectives, in DDD/1000 population/day 2006 and DD/population/year ATC Drug Class and Agents 2006 2006 (DDDs/population/ year) J01 J02 J04 J05 P01B ANTIBACTERIALS FOR SYSTEMIC USE ANTIMYCOTICS FOR SYSTEMIC USE ANTIMYCOBACTERIALS ANTIVIRALS FOR SYSTEMIC USE ANTIMALARIALS 8.9369 0.3253 1.099 0.5638 0.0807 3.262 0.1187 0.4011 0.2058 0.0295 66 CHAPTER 15 USE OF ANTIINFECTIVES Malaysian Statistics on Medicines 2006 Table 15.2.1: Use of Anti-Bacterials by Drug Class, in DDD/1000 population/day 2006 ATC Drug Class and Agents 2006 2006 (DDDs/population/year) J01A J01B J01C J01D J01E J01F J01G J01M J01X TETRACYCLINES AMPHENICOLS BETA -LACTAM ANTIBACTERIALS, PENICILLINS OTHER BETA-LACTAM ANTIBACTERIALS SULFONAMIDES AND TRIMETHOPRIM MACROLIDES, LINCOSAMIDES AND STREPTOGRAMINS AMINOGLYCOSIDE ANTIBACTERIALS QUINOLONE ANTIBACTERIALS OTHER ANTIBACTERIALS 1.1032 0.0045 4.2079 0.9589 0.4027 0.0017 1.5359 0.35 0.7657 1.3867 0.2795 0.5062 0.046 0.3877 0.0762 0.0168 0.1415 0.0278 Table 15.2.2: Use of Anti-Bacterials by Drug Class and Agents, in DDD/1000 population/day 2006 ATC Drug Class and Agents J01A A Tetracyclines J01A A02 Doxycycline J01A A06 Oxytetracycline J01A A07 Tetracycline J01A A08 Minocycline J01B A Amphenicols J01B A01 Chloramphen icol J01C A Penicillins with extended spectrum J01C A01 Ampicillin J01C A04 Amoxicillin J01C A06 Bacampicillin J01C A12 Piperacillin 2006 J01C E Beta-lactamase sensitive penicillins J01C E01 Benzylpenicillin 2006 (DDDs/population/year) Public Private Total Public Private Total Public Private Total Public Private Total 0.2688 0.6527 0.9215 <0.0001 <0.0001 <0.0001 0.0585 0.0885 0.147 0.0004 0.0343 0.0347 0.0981 0.2382 0.3363 <0.0001 <0.0001 <0.0001 0.0214 0.0323 0.0537 0.0001 0.0125 0.0127 Public Private Total 0.0027 0.0019 0.0045 0.001 0.0007 0.0017 Public Private Total Public Private Total Public Private Total Public Private Total 0.0692 0.0565 0.1257 0.698 1.4018 2.0998 0.2145 0.0648 0.2793 0.0002 0.0002 0.0252 0.0206 0.0459 0.2548 0.5117 0.7664 0.0783 0.0237 0.102 <0.0001 <0.0001 Public Private Total 0.0182 0.0013 0.0195 0.0067 0.0005 0.0071 67 CHAPTER 15 USE OF ANTIINFECTIVES Malaysian Statistics on Medicines 2006 ATC Drug Class and Agents J01C E02 Phenoxymethylpenicillin J01C E08 Benzathine benzylpenicillin J01C E09 Procaine benzylpenicillin 2006 2006 (DDDs/population/year) Public Private Total Public Private Total Public Private Total 0.1706 0.0173 0.188 0.0018 0.0004 0.0022 0.0077 0.0002 0.0079 0.0623 0.0063 0.0686 0.0007 0.0001 0.0008 0.0028 <0.0001 0.0029 Public Private Total Public Private Total 0.6363 0.1638 0.8002 0.0014 0.0112 0.0126 0.2323 0.0598 0.2921 0.0005 0.0041 0.0046 J01C F Beta-lactamase resistant penicillins J01C F02 Cloxacillin J01C F05 Flucloxacillin J01C R Combinations of penicillins, incl. beta-lactamase inhibitors J01C R01 Ampicillin and enzyme inhibitor J01C R02 Amoxicillin and enzyme inhibitor J01C R04 Sultamicillin J01C R05 Piperacillin and enzyme inhibitor J01D B First-generation cephalosporins J01D B01 Cefalexin J01D B04 Cefazolin J01D B05 Cefadroxil J01D B09 Cefradine J01D C Second-generation cephalosporins J01D C02 Cefuroxime J01D C04 Cefaclor Publi c Private Total Public Private Total Public Private Total Public Private Total 0.0181 0.0124 0.0306 0.1484 0.4491 0.5974 0.0113 0.0289 0.0402 0.003 0.0014 0.0044 0.0066 0.0045 0.0112 0.0542 0.1639 0.2181 0.0041 0.0105 0.0147 0.0011 0.0005 0.0016 Public Private Total Public Private Total Public Private Total Public Private Total 0.0607 0.306 0.3667 <0.0001 0.0031 0.0031 0.0489 0.0489 0.0008 0.0008 0.0222 0.1117 0.1339 <0.0001 0.0011 0.0011 0.0178 0.0178 0.0003 0.0003 Public Private Total Public Private Total 0.1619 0.2013 0.3631 0.0019 0.0462 0.0481 0.0591 0.0735 0.1325 0.0007 0.0169 0.0176 68 CHAPTER 15 USE OF ANTIINFECTIVES ATC Drug Class and Agents J01D C10 Cefprozil J01D D Third-generation cephalosporins J01D D01 Cefotaxime J01D D02 Ceftazidime J01D D04 Ceftriaxone J01D D12 Cefoperazone J01D D14 Ceftibuten J01D E Fourth-generation cephalosporins J01D E01 Cefepime J01D H Carbapenems J01D H02 Meropenem J01D H03 Ertapenem J01D H51 Imipenem and enzyme inhibitor J01E A Trimethoprim and derivatives J01E A01 Trimethoprim J01E B04 Sulfapyridine Malaysian Statistics on Medicines 2006 2006 2006 (DDDs/population/year) Public Private Total 0.0004 0.0135 0.014 0.0001 0.0049 0.0051 Public Private Total Public Private Total Public Private Total Public Private Total Public Private Total 0.004 0.0005 0.0046 0.0078 0.0027 0.0104 0.0163 0.0221 0.0384 0.0091 0.0006 0.0098 0.0134 0.01 34 0.0015 0.0002 0.0017 0.0028 0.001 0.0038 0.0059 0.0081 0.014 0.0033 0.0002 0.0036 0.0049 0.0049 Public Private Total 0.0105 0.0086 0.0191 0.0038 0.0031 0.007 Public Private Total Public Private Total Public Private Total 0.0055 0.0027 0.0082 <0.0001 0.0021 0.0022 0.0058 0.0023 0.0081 0.002 0.001 0.003 <0.0001 0.0008 0.0008 0.0021 0.0008 0.0029 Public Private Total Public Private Total 0.0178 0.0051 0.0229 0.2112 0.2112 0.0065 0.0018 0.0083 0.0771 0.0771 J01E E Combinations of sulfonamides and trimethoprim, incl. derivatives J01E E01 Sulfamethoxazole and trimethoprim J01E E02 Sulfadiazine and trimethoprim Publi c Private Total Public Private Total 69 0.2487 0.2585 0.5072 0.0245 0.0245 0.0908 0.0944 0.1851 0.0089 0.0089 CHAPTER 15 USE OF ANTIINFECTIVES Malaysian Statistics on Medicines 2006 ATC Drug Class and Agents J01F A Macrolides J01F A01 Erythromycin J01F A02 Spiramycin J01F A06 Roxithromycin J01F A09 Clarithromycin J01F A10 Azithromycin J01F F Lincosamides J01F F01 Clindamycin J01F F 02 Lincomycin J01G A Streptomycins J01G A01 Streptomycin J01G B Other aminoglycosides J01G B03 Gentamicin J01G B04 Kanamycin J01G B06 Amikacin J01G B07 Netilm icin J01M A Fluoroquinolones J01M A01 Ofloxacin J01M A02 Ciprofloxacin J01M A03 Pefloxacin 2006 2006 (DDDs/population/year) Public Private Total Public Private Total Public Private Total Public Private Total Public Private Total 0.5574 0.38 4 0.9414 <0.0001 0.0015 0.0015 0.1182 0.1182 0.0191 0.1745 0.1936 0.0119 0.0998 0.1117 0.2035 0.1401 0.3436 <0.0001 0.0005 0.0006 0.0431 0.0431 0.007 0.0637 0.0707 0.0044 0.0364 0.0408 Public Private Total Public Private Total 0.0057 0.0082 0.0139 0.0064 0.0064 0.0021 0.003 0.0051 0.0023 0.0023 Public Private Total 0.0243 0.0007 0.025 0.0089 0.0003 0.0091 Publi c Private Total Public Private Total Public Private Total Public Private Total 0.006 0.0077 0.0136 0.0002 0.0004 0.0007 0.0032 0.0014 0.0046 0.0009 0.0012 0.0021 0.0022 0.0028 0.005 <0.0001 0.0002 0.0002 0.0012 0.0005 0.0017 0.0003 0.0005 0.0008 Public Private Total Public Private Total Public Private Total 0.013 0.0935 0.1066 0.0226 0.1179 0.1405 0.0022 0.0065 0.0087 0.0047 0.0341 0.0389 0.0082 0.04 3 0.0513 0.0008 0.0024 0.0032 70 CHAPTER 15 USE OF ANTIINFECTIVES ATC Drug Class and Agents J01M A06 Norfloxacin J01M A12 Levofloxacin J01M A14 Moxifloxacin J01M A16 Gatifloxacin J01M B Other quinolones J01M B02 Nalidixic acid J01M B04 Pipemidic acid J01M B07 Flumequine J01X A Glycopeptide antibacterials J01X A01 Vancomycin J01X A02 Teicoplanin J01X B Polymyxins J01X B01 Colistin J01X B02 Polymyxin B J01X C Steroid antibacterials J01X C01 Fusidic acid J01X D Imidazole derivatives J01X D01 Metronidazole J01X D02 Tinidazole Malaysian Statistics on Medicines 2006 2006 2006 (DDDs/population/year) Public Private Total Public Private Total Public Private Total Public Private Total <0.0001 0.0818 0.0818 0.001 0.0195 0.0205 0.0002 0.0163 0.0165 0.0003 0.0043 0.0046 <0.0001 0.0299 0.0299 0.0004 0.0071 0.0075 <0.0001 0.0059 0.006 0.0001 0.0016 0.0017 Public Private Total Public Private Total Public Private Total 0.0085 0.0085 <0.0001 <0.0001 0.0031 0.0031 <0.0001 <0.0001 Public Private Total Public Private Total 0.0035 0.0013 0.0048 0.0002 0.0004 0.0005 0.0013 0.0005 0.0018 <0.0001 0.0001 0.0002 Public Private Total Public Private Total <0.0001 <0.0001 <0.0001 <0.0001 <0.0001 <0.0001 <0.0001 <0.0001 <0.0001 <0.0001 Public Private Total 0.0089 0.0016 0.013 0.0032 0.0006 0.0038 Public Private Total Public Private Total 0.0358 0.0128 0.0486 - 0.0131 0.0047 0.0177 - 71 CHAPTER 15 USE OF ANTIINFECTIVES Malaysian Statistics on Medicines 2006 ATC Drug Class and Agents J01X E Nitrofuran derivatives J01X E01 Nitrofurantoin J01X X Other antibacterials J01X X01 Fosfomycin J01X X04 Spectinomycin J01X X08 Linezolid 2006 2006 (DDDs/population/year) Publ ic Private Total 0.0064 0.0022 0.0086 0.0023 0.0008 0.0031 Public Private Total Public Private Total Public Private Total 0.0016 0.0016 <0.0001 <0.0001 0.001 0.0004 0.0014 0.0006 0.0006 <0.0001 <0.0001 0.0004 0.0001 0.0005 Table 15.3.1: Use of Anti-Mycotics by Drug Class, in DDD/1000 population/day 2006 ATC Drug Class and Agents 2006 2006 (DDDs/population/year) J02A A J02A B J02A C J02A X Antibiotics Imidazole derivatives Triazole derivatives Other antimycotics for systemic use 0.0028 0.2352 0.0872 0.0001 0.001 0.0859 0.0318 <0.0001 Table 15.3.2: Use of Anti-Mycotics by Drug Class and Agents, in DDD/1000 population/day 2006 ATC Drug Class and Agents 2006 2006 (DDDs/population/year) J02A A Antibiotics J02A A01 Amphotericin B J02A B Imidazole derivatives J02A B02 Ketoconazole J02A C Triazole derivatives J02A C01 Fluconazole J02A C02 Itraconazole J02A C03 Voriconazole J02A X Other antimycotics for systemic use J02A X01 Flucytosine J02A X04 Caspofungin Public Private Total 0.0026 0.0002 0.0028 0.001 <0.0001 0.001 Public Private Total 0.0117 0.2235 0.2352 0.0043 0.0816 0.0859 Public Private Total Public Private Total Public Private Total 0.0146 0.0203 0.035 0.0227 0.0294 0.0521 0.0002 0.0002 0.0053 0.0074 0.0128 0.0083 0.0107 0.019 <0.0001 <0.0001 Public Private Total Public Private Total <0.0001 <0.0001 <0.0001 <0.0001 <0.0001 <0.0001 <0.0001 <0.000 1 <0.0001 <0.0001 72 CHAPTER 15 USE OF ANTIINFECTIVES Malaysian Statistics on Medicines 2006 Table 15.4.1: Use of Anti-Mycobacterials by Drug Class, in DDD/1000 population/day 2006 ATC Drug Class and Agents J04A B Antibiotics J04A B01 Cycloserine J04A B02 Rifampicin 2006 2006 (DDDs/population/year) Public Private Total Public Private Total 0.0016 0.0016 0.256 0.0228 0.2788 0.0006 0.0006 0.0934 0.0083 0.1018 Public Private Total Public Private Total 0.4356 0.0242 0.4598 <0.0001 <0.0001 0.159 0.0088 0.1678 <0.0001 <0.0001 Public Private Total Public Private Total Public Private Total Public Private Total Public Private Total 0.1084 0.0143 0.1226 0.0891 0.0174 0.1065 0.0143 0.0143 0.0065 0.0065 0.0001 0.0001 0.0395 0.0052 0.0448 0.0325 0.0064 0.0389 0.0052 0.0052 0.0024 0.0024 <0.0001 <0.0001 Public Private Total Public Private Total 0.004 0.004 0.1047 <0.0001 0.1047 0.0015 0.0015 0.0382 <0.0001 0.0382 J04A C Hydrazides J04A C01 Isoniazid J04A D03 Ethionamide J04A K Other drugs for treatment of tuberculosis J04A K01 Pyrazinamide J04A K02 Ethambutol J04A M02 Rifampicin and isoniazid J04A M05 Rifampicin, pyrazinamide and isoniazid J04A M06 Rifampicin, pyrazinamide, ethambutol and isoniazid J04B A Drugs for treatment of lepra J04B A01 Clofazimine J04B A02 Dapsone Table 15.5.1: Use of Anti-Malarials by Drug Class, in DDD/1000 population/day 2006 ATC Drug Class 2006 2006 (DDDs/population/year) P01A P01B A P01B B P01B C P01B D AGENTS AGAINST AMOEBIASIS AND OTHER PRO TOZOAL DISEASES Aminoquinolines Biguanides Methanolquinolines Diaminopyrimidines 73 0.1992 0.0727 0.0648 <0.0001 0.0049 0.011 0.0236 <0.0001 0.0018 0.004 CHAPTER 15 USE OF ANTIINFECTIVES Malaysian Statistics on Medicines 2006 Table 15.5.2: Use of Anti-Malarials by Drug Class and Agents, in DDD/1000 population/day 2006 ATC Drug Class and Agents P01A 2006 (DDDs/population/year) AGENTS AGAINST AMOEBIASIS AND OTHER PROTOZOAL DISEASES P01A B01 Metronidazole P01A B02 Tinidazole P01B A Aminoquinolines P01B A01 Chloroquine P01B A02 Hydroxychloroquine P01B A03 Primaquine P01B B Biguanides P01B B51 Proguanil, combinations P01B C Methanolquinolines P01B C01 Quinine P01B C02 Mefloquine P01B D Diaminopyrimidines P01B D01 Pyrimethamine P01B D51 Pyrimethamine, combinations 2006 Public Private Total Public Private Total 0.1108 0.0839 0.1947 0.0045 0.0045 0.0404 0.0306 0.0711 0.0016 0.0016 Public Private Total Public Private Total Public Private Total 0.0082 0.0048 0.013 0.0158 0.0025 0.0183 0.031 0.0024 0.0334 0.003 0.0018 0.0048 0.0058 0.0009 0.0067 0.0113 0.0009 0.0122 Public Private Total <0.0001 <0.0001 <0.0001 <0.0001 Public Private Total Public Private Total 0.0035 0.0013 0.0048 <0.0001 <0.0001 0.0013 0.0005 0.0018 <0.0001 <0.0001 Public Priva te Total Public Private Total 0.0002 <0.0001 0.0003 0.0091 0.0017 0.0108 <0.0001 <0.0001 0.0001 0.0033 0.0006 0.0039 Table 15.6.1: Use of Anti-Virals by Drug Class, in DDD/1000 population/day 2006 ATC Drug Class 2006 2006 (DDDs/population/year) J05A B Nucleosides and nucleotides excl. reverse transcriptase inhibitors Protease inhibitors Nucleoside and nucleotide reverse transcriptase inhibitors Non-nucleoside reverse transcriptase inhibitors Neuraminidase inhibitors 0.0519 0.0189 0.0109 0.177 0.004 0.0646 0.092 0.0336 0.1544 0.0563 J05A E J05A F J05A G J05A H 74 CHAPTER 15 USE OF ANTIINFECTIVES Malaysian Statistics on Medicines 2006 Table 15.6.2: Use of Anti-Virals by Drug Class and Agents, in DDD/1000 population/day 2006 ATC Drug Class and Agents 2006 J05A B 2006 (DDDs/population/year) Nucleosides and nucleotides excl. reverse transcriptase inhibitors J05A B01 Aciclovir J05A B04 Ribavirin J05A B06 Ganciclovir J05A B09 Famciclovir J05A B11 Valaciclovir J05A B14 Valganciclovir J05A D01 Foscarnet J05A E Protease inhibitors J05A E01 Saquinavir 0.0063 0.0406 0.047 0.0026 0.0005 0.0031 0.0004 <0.0001 0.0004 <0.0001 0.0012 0.0013 <0.0001 <0.0001 <0.0001 <0.0001 <0.0001 0.0023 0.0148 0.0171 0.0009 0.0002 0.0011 0.0001 <0.0001 0.0001 <0.0001 0.0004 0.0005 <0.0001 <0.0001 <0.0001 <0.0001 <0.0001 <0.0001 <0.0001 0.0023 0.0001 0.0024 0.0008 0.0008 <0.0001 <0.0001 0.0008 0.0008 J05A F Public Private <0.0001 Total <0.0001 Indinavir Public 0.0063 Private 0.0003 Total 0.0066 Ritonavir Public 0.0021 Private Total 0.0021 Nelfinavir Public <0.0001 Private Total <0.0001 Lopinavir Public 0.0022 Private Total 0.0022 Nucleoside and nucleotide reverse transcriptase inhibitors J05A F01 Zidovudine J05A F02 Didanosine J05A F04 Stavudine J05A E02 J05A E03 J05A E04 J05A E06 Public Private Total Public Private Total Public Private Total Public Private Total Public Private Total Public Private Total Public Private Total Public Private Total Public Private Total Public Private Total 75 0.0033 0.0033 0.0089 0.0011 0.01 0.0337 0.0012 0.0349 0.0012 0.0012 0.0032 0.0004 0.0036 0.0123 0.0004 0.0128 CHAPTER 15 USE OF ANTIINFECTIVES Malaysian Statistics on Medicines 2006 ATC Drug Class and Agents J05A F05 Lamivudine J05A F08 Adefovir dipivoxil J05A F10 Entecavir 2006 2006 (DDDs/population/year) 0.1096 0.0064 0.116 0.0038 0.0061 0.0099 0.0028 0.0028 0.04 0.0023 0.0423 0.0014 0.0022 0.0036 0.001 0.001 Public Private Total Public Private Total 0.0616 0.0001 0.0618 0.0285 0.0017 0.0302 0.0225 <0.0001 0.0225 0.0104 0.0006 0.011 Public Private Total Public Private Total Public Private Total 0.0299 0.0299 0.1204 0.004 0.1245 0.0751 0.0025 0.0776 0.0109 0.0109 0.044 0.0015 0.0454 0.0274 0.0009 0.0283 Public Private Total Public Private Total Public Private Total J05A G Non-nucleoside reverse transcriptase inhibitors J05A G01 Nevirapine J05A G03 Efavirenz J05A H Neuraminidase inhibitors J05A H01 Zanamivir J05A H02 Oseltamivir J05A R01 Zidovudine and lamivudine References: 1. Patrick DM, Marra F , Hutchinson J , et al. Per capita antibiotic consumption: How does a North American Jurisdiction compare with Europe? Clin Infect Dis. 2004; 39:11-7. 2. Goossens H, Ferech M, Coenen S et al. Comparison of outpatient systemic antibacterial use in 2004 in the Unitd States & 27 European countries. Clin Infect Dis. 2007; 44: 1091-5. 3. Ferech M, Coenen S, Kumar SM et al. European Surveillance of Antimicrobial Consumption (ESAC): outpatient antibiotic use in Europe. J Antimicrob Chemother 2006; 58:401-7. 4. Health Protection Agency. Antimicrobial Resistance and Prescribing in England, Wales and Northern Ireland, 2008. London. 5. Pakyz AL, MacDougall C, Oinonen M, Polk RE. Trends in Antibacterial Use in US Academic Health Centers 2002 to 2006. Arch Intern Med. 2008; 168(20):2254-2260. 6. Avorn JL, Barrett JF, Davey PG, McEwen SA, O’Brien TF and Levy SB. 2001. Antibiotic resistance: synthesis of recommendations by expert policy groups Alliance for the Prudent Use of Antibiotics United States of America World Health Organization. 76 CHAPTER 16: USE OF ANTINEOPLASTIC AGENTS INCLUDING ENDOCRINE THERAPY Malaysian Statistics on Medicines 2006 Edited by: Lim YS1, Lim GC1, Goh AS㪉, Wan Ariffin A3, M Roslan H4, Kamarun Neasa BMK1, Yuzlina MY5 1. Kuala Lumpur Hospital, 2. Pulau Pinang Johor Bahru, 5. Putrajaya Hospital Hospital, 3. Universiti Malaya, 4. Sultan Ismail Hospital, Systemic therapy is part of the treatment for many cancer patients and for some malignancies they may be the only option. Systemic therapy in cancer is particularly complex and antineoplastic drugs are used either as monotherapy or in combination in different regimes. Antineoplastics can be used in first line or as treatment for relapse of disease. Some of the antineoplastics have been around since 6 decades ago. Taxanes came in use in 1992 followed by the molecular targeted agents such as Imatinib Mesylate in early 2000’s. Bevacizumab was the first clinically proven antiangiogenic agent for the treatment of colon cancer in 2004. The top ten antineoplastics in terms of expenditure in 2006 by public hospitals were Epirubicin (RM5.3 million), Docetaxel (RM5.2 million), Oxaliplatin (RM2.8 million), Rituximab (RM2.5 million), Gemcitabine (RM2.1 million), Irinotecan (RM2.0 million), Methotrexate (RM1.3 million), Paclitaxel (RM 1.2 million), Fluorouracil (RM1.1 million) and Capecitabine (RM1.0 million). Prices were quoted according to Hospital Kuala Lumpur catalog of drug prices for 2006. Epirubicin was used mainly for breast cancer as in the FEC regime which was a combination therapy with Flurouracil and Cyclophosphamide. Docetaxel was used mainly in breast cancer for salvage therapy. This taxane was also used in Non-Small Cell Lung Cancer (NSCLC). Another taxane, Paclitaxel was used in ovarian cancer and NSCLC in combination with Carboplatin or Cisplatin. Then in 2006, government hospitals started using Paclitaxel for a new indication in Ministry of Health (MOH) Formulary in combination with Gemcitabine for breast cancer. The earlier indication of Gemcitabine that was approved by the Drug Control Authority (DCA) was for pancreatic cancer. Furthermore Gemcitabine was widely used for NSCLC in combination with Cisplatin, a platinum compound. Irinotecan was frequently used for colorectal cancer. On the other hand, Methotrexate, a folic acid analog was used for breast cancer in combination with Cyclophosphamide and Fluorouracil. This is the popularly known CMF regime which was the first line therapy in many breast cancer patients. Fluorouracil was mainly used for colorectal cancer, breast cancer, nasopharyngeal cancer, stomach and pancreatic cancer. Capecitabine is an antimetabolite of pyrimidine analog. Capecitabine initially was used in public hospitals for colorectal cancer only, but not long afterwards was also indicated for breast cancer in metastatic setting. Tegafur was used in private hospitals exceeding ten fold more than in public hospitals. Tegafur was on case by case approval by Director General of Health until 2008 when it was indicated for NSCLC. However Tegafur found many more uses in private hospitals in addition to NSCLC such as head and neck cancer and breast cancer. Hence the disparity between quantum of Tegafur used in private compared to public hospitals. The tyrosine kinase inhibitor Imatinib was included in the MOH Formulary in 2007. Imatinib was used for CML as well as for gastro-intestinal stromal tumour (GIST) which had been incompletely resected or unresectable. The usage of Imatinib was actually higher than captured in these procurement data due to the Glivec International Assistance Program (GIPAP) in CML and GIST in Malaysia. The other molecular targeted therapy were the monoclonal antibodies Rituzimab and Trastuzumab. While Rituzimab was already in MOH Formulary since 2004, Trastuzumab was used on a named-patient basis in 2006. This accounted for the relatively low expenditure for Trastuzumab. In haematological malignancies, Rituximab and the proteosome inhibitor, Bortezomib are making real impact on patient survival and remission rates. Rituximab was already in the MOH Formulary in 2004 for Rituximab enhanced regime of Cyclophosphamide, Adriamycin, Vincristine and Prednisolone (R-CHOP) in Non-Hodgkin’s Lymphoma whereas Bortezomib was not in the MOH Formulary until 2008. However, improvement in survival comes at a cost and the soaring price of new cancer regimes are adding to the financial burden of cancer patients and causing a strain to public hospitals’ budget. 77 Malaysian Statistics on Medicines 2006 CHAPTER 16: USE OF ANTINEOPLASTIC AGENTS INCLUDING ENDOCRINE THERAPY Due to the exorbitant price of the newer drugs, only a selected number of patients may have access to these novel targeted agents. The newer drugs that are being focused on in government hospitals are those in whom overall survival benefit have been proven in published randomised controlled trials. Patients depend largely on insurance coverage in the private hospitals and adequacy of budget in individual government hospitals. The usage of Rituximab was more in public than in private hospitals. The usage of Bortezomib was low in government, university hospitals and private hospitals. Many patients would go to public hospitals if they could get the monoclonal antibodies there since they would not need to worry about the exorbitant prices of the drugs that were heavily subsidised. Other non-formulary drugs such as anagrelide and arsenic trioxide were little used in public hospitals and even less so in private hospitals. Table 16.1: Use of Antineoplastic Agents by Drug Class and Agents, in total dosage/1000 population/day 2006 ATC Drug Class and Agents Unit 2006 L01A A Nitrogen mustard analogues L01A A01 L01 A A02 L01A A03 L01A A06 mg Melphalan g Ifosfamide Alkyl sulfonates L01A B01 Busulfan L01A C Ethylene imines L01A C01 Thiotepa L01A D Nitrosoureas L01A D01 Carmustine mg mg mg mg Lomustine L01A X Other alkylating agents L01A X03 Temozolomide L01A X04 mg Chlorambucil L01A B L01A D0 2 mg Cyclophosphamide mg mg Dacarbazine 78 Public 2.2612 Private 0.6601 Total 2.9212 Public 0.0062 Private 0.0009 Total 0.0071 Public 0.0036 Private <0.0001 Total 0.0036 Public 0.0009 Private 0.0001 Total 0.0011 Public 0.0093 Private <0.0001 Total 0.0095 Public - Private <0.0001 Total <0.0001 Public 0.003 Private <0.0001 Total 0.003 Public 0.0008 Private 0.0003 Total 0.001 Public 0.0045 Private 0.022 Total 0.0265 Public 0.0631 Private 0.0198 Total 0.0829 CHAPTER 16: USE OF ANTINEOPLASTIC AGENTS INCLUDING ENDOCRINE THERAPY Malaysian Statistics on Medicines 2006 Table 16.2: Use of Antineoplastic Agents by Drug Class, in total dosage/1000population/day 2006 ATC L01B A Drug Class and Agents Folic acid analogues Unit L01B A01 Methotrexate mg L01B A04 Pemetrexed mg L01B B Purine analogues L01B B02 Mercaptopurine mg L01B B03 Tioguanine mg L01B B04 Cladribine mg L01B B05 Fludarabine mg L01B C Pyrimidine analogues L01B C01 Cytarabine mg L01B C02 Fluorouracil mg L01B C05 Gemcitabine mg L01B C06 Capecitabine mg L01B C53 Tegafur, combinations mg 2006 Public Private Total Public Private Total 0.6852 0.1102 0.7954 0.0055 0.0055 Public Private Total Public Private Total Public Private Total Public Private Total 0.6879 0.0103 0.6982 0.0133 0.0002 0.0135 <0.0 001 <0.0001 0.001 0.0018 0.0028 Public Private Total Public Private Total Public Private Total Public Private Total Public Private Total 0.7999 0.0436 0.8435 4.8107 1.4858 6.2965 0.2908 0.121 0.4118 7.5826 8.9727 16.5553 0.0272 0.326 0.3533 Table 16.3: Use of Antineoplastic Agents by Drug Class and Agents, in total dosage/1000 population/day 2006 ATC Drug Class and Agents Unit 2006 L01C A Vinca alkaloids and analogues L01C A01 Vinblastine mg L01C A02 Vincristine mg L01C A04 Vinorelbine mg 79 Public Private Total Public Private Total Public Private Total 0.0011 0.0003 0.0014 0.0018 0.0002 0.002 0.0062 0.0051 0.0113 Malaysian Statistics on Medicines 2006 CHAPTER 16: USE OF ANTINEOPLASTIC AGENTS INCLUDING ENDOCRINE THERAPY ATC L01C B Drug Class and Agents Podophyllotoxin derivatives Unit L01C B01 Etop oside mg L01C B02 Teniposide mg L01C D Taxanes L01C D01 Paclitaxel mg L01C D02 Docetaxel mg 2006 Public Private Total Public Private Total 0.1511 0.0293 0.1804 0.0015 <0.0001 0.0015 Public Private Total Public Private Total 0.0687 0.0464 0.1151 0.0152 0.0158 0.031 Table 16.4: Use of Antineoplastic Agents by Drug Class, in total dosage/1000 population/day 2006 ATC L01D A Drug Class and Agents Actinomycines Unit L01D A01 Dactinomycin mg Public Private Total <0.0001 <0.0001 <0.0001 L01D B Anthracyclines and related substances L01D B01 Doxorubicin mg L01D B02 Daunorubicin mg L01D B03 Epirubicin mg L01D B06 Idarubicin mg L01D B07 Mitoxantrone mg Public Private Total Public Private Total Public Private Total Public Private Total Public Private Total 0.0426 0.0274 0.0701 0.0085 0.0008 0.0093 0.0771 0.0123 0.0893 0.0008 <0.0001 0.0009 0.0003 0.0001 0.0004 Public Private Total Public Private Total 0.0074 0.0031 0.0105 0.002 0.001 0.003 L01D C Other cytotoxic antibiotics L01D C01 Bleomycin mg L01D C03 Mitomycin mg 80 2006 CHAPTER 16: USE OF ANTINEOPLASTIC AGENTS INCLUDING ENDOCRINE THERAPY Malaysian Statistics on Medicines 2006 Table 16.5: Use of Antineoplastic Agents by Drug Class and Agents, in total dosage/1000 population/day 2006 ATC L01X A Drug Class and Agents Platinum compounds Unit L01X A01 Cisplatin mg L01X A02 Carboplatin mg L01X A03 Oxaliplatin mg L01X B Methylhydrazines L01X B01 Procarbazine L01X C Monoclonal antibodies L01X C02 2006 Public Private Total Public Private Total Public Private Total 0.0817 0.0462 0.1278 0.3832 0.1088 0.4919 0.0123 0.0281 0.0404 mg Public Private Total 0.0269 <0.0001 0.0269 Rituximab mg L01X C0 3 Trastuzumab mg L01X C06 Cetuximab mg L01X C07 Bevacizumab mg L01X E01 Imatinib mg L01X E02 Gefitinib mg Public Private Total Public Private Total Public Private Total Public Private Total Public Private Total Public Private Total 0.0377 0.0242 0.0619 0.0008 0.0058 0.0065 0.0017 0.0335 0.0352 0.0128 0.0128 0.0942 0.2025 0.2966 0.0086 0.1336 0.1422 L01X X Other antineoplastic agents L01X X02 Asparaginase mg L01X X05 Hydroxycarbamide mg L01X X11 Estramustine mg L01X X14 Tretinoin mg L01X X17 Topotecan mg Public Private Total Publ ic Private Total Public Private Total Public Private Total Public Private Total 5.2422 0.2473 5.4895 23.5787 5.4791 29.0578 <0.0001 <0.0001 0.0301 0.0046 0.0347 - 81 Malaysian Statistics on Medicines 2006 ATC CHAPTER 16: USE OF ANTINEOPLASTIC AGENTS INCLUDING ENDOCRINE THERAPY Drug Class and Agents Unit L01 X X19 Irinotecan mg L01X X27 Arsenic trioxide mg L01X X32 Bortezomib mg L01X X35 Anagrelide mg 2006 Public Private Total Public Private Total Public Private Total Public Private Total References: 1. Australia Department of Health and Ageing, Australian Statistics On Medicine 2003. 2. Statistics on Drug use in Australia 2006. 82 0.0202 0.0097 0.03 0.0007 0.0007 <0.0001 <0.0001 <0.0001 0.0037 0.0005 0.0042 CHAPTER 17: USE OF SYSTEMIC CORTICOSTEROIDS AND IMMUNOSUPPRESIVE AGENTS Malaysian Statistics on Medicines 2006 Edited by: Hooi LS1, Zaki M2, Lim TO3, Zawawi N4, Goh BL5, Fadilah O6, Nur Salima S6, Puteri JZ6, Zarina AG6, Manjulaa DS7 1. Sultanah Aminah Hospital, Johor Bharu, 2. International Medical University, 3. Clinical Research Centre, MOH, 4. Sultanah Nur Zahirah Hospital, Terengganu, 5. Serdang Hospital, 6. Selayang Hospital, 7. Kuala Lumpur Hospital The list of drugs in this chapter include steroids, progestogens, gonadotropin releasing hormone (GnRH) analogues, tamoxifen, anti-androgens, enzyme inhibitors, granulocyte colony stimulating factor, interferons and immunosuppressants like calcineurin inhibitors, mycophenolate acid, sirolimus, etanercept, infliximab, azathioprine, thalidomide and methotrexate. The main drug in this chapter is prednisolone. Systemic glucocorticoids have non-specific anti-inflammatory and immunosuppressant properties but the side-effects are protean. The usage in 0.4% of the general population in 2006 is high. This amounts to 118,000 people on glucocorticoids daily assuming the population of Malaysia was 26.6 million in 2006 (table 17.1). About 67,000 people per day were on prednisolone (table 17.2). This may suggest overuse or even abuse of steroids, which warrants further investigation. There were a total of 490 patients treated with GnRH analogues (for cancer of the prostate), 6,000 on tamoxifen (for cancer of the breast), 230 on the anti-androgens (for cancer of the prostate) and 600 on the enzyme inhibitors (for cancer of the breast). Granulocyte colony stimulating factor was used very little (70 per day) and interferon usage was surprisingly low in view of the large numbers of patients with hepatitis B and hepatitis C in Malaysia. Multiple sclerosis is a rare disease here and the use of interferon beta-1a is low. The total usage of all classes of interferons was 480 people per day. There may be under-usage of these drugs for their justified indications but this may reflect their high cost. There were about 1,460 people on ciclosporin, 135 on tacrolimus and 540 on mycophenolic acid from the data available. From the National Transplant Registry of 2006 there were 1,120 patients with functioning kidney transplants on ciclosporin in 2006 [1]. It is used mainly in the public sector as there is a specific allocation for its use for renal transplantation. There were 254 renal transplant patients on tacrolimus in 2006 and 705 on mycophenolate mofetil (MMF) [1]. DDD/1000 population/day for MMF is 2g which is the standard when used in combination with cyclosporine. In combination with tacrolimus the dose of MMF is usually halved to 1 g/day. This may explain the lower figures reported here compared to NTR figures for mycophenolic acid. There were a negligible number of people on sirolimus, etanercept and infliximab. The last 2 mainly for rheumatoid arthritis are very costly. About 2,500 patients were on azathioprine and there were 100 people on methotrexate. Table 17.1: Use of Systemic Corticosteroids and Immunosuppressive Agents by Drug Class, in DDD/1000 population/day 2006 ATC Drug Class 2006 H02A A H02A B Mineralocorticoids Glucocorticoids 0.0034 4.4433 Table 17.2: Use of Systemic Corticosteroids and Immunosuppressive Agents by Drug Class and Agents, in DDD/1000 population/day 2006 ATC H02A A Drug Class and Agents Mineralocorticoids H02A A02 Fludrocortisone 2006 Public Private Total 83 0.0023 0.0011 0.0034 Malaysian Statistics on Medicines 2006 ATC H02A B Drug Class and Agents Glucocorticoids H02A B01 Betamethasone H02A B02 Dexamethasone H02A B04 Methylprednisolone H02A B06 Predni solone H02A B08 Triamcinolone H02A B09 Hydrocortisone CHAPTER 17: USE OF SYSTEMIC CORTICOSTEROIDS AND IMMUNOSUPPRESIVE AGENTS 2006 Public Private Total Public Private Total Public Private Total Public Private Total Public Private Total Public Private Total 0.429 0.429 0.32 0.274 0.594 0.0866 0.0561 0.1427 1.1766 1.3428 2.5194 0.0133 0.1086 0.1219 0.3073 0.3291 0.6364 Table 17.3: Use of Systemic Corticosteroids and Immunosuppressive Agents by Drug Class, in DDD/1000 population/day 2006 ATC Drug Class 2006 L02 L03 L04 ENDOCRINE THERAPY IMMUNOSTIMULANTS IMMUNOSUPPRESSIVE AGENTS 0.2844 6.149 0.2001 Table 17.4: Use of Systemic Corticosteroids and Immunosuppressive Agents by Drug Class, in DDD/1000 population/day 2006 ATC L02A B Drug Class and Agents Progestogens 2006 L02A B01 Megestrol L02A B02 Medroxyprogesterone L02A E Gonad otropin releasing hormone analogues L02A E01 Buserelin L02A E02 Leuprorelin L02A E03 Goserelin L02A E04 Triptorelin 84 Public Private Total Public Private Total 0.0067 0.0067 <0.0001 <0.0001 0.0001 Public Private Total Public Private Total Public Private Total Public Private Total <0.0001 <0.0001 <0.0001 0.0024 0.0085 0.0109 0.0038 0.0021 0.0059 0.0011 0.0003 0.0015 CHAPTER 17: USE OF SYSTEMIC CORTICOSTEROIDS AND IMMUNOSUPPRESIVE AGENTS ATC L02B A Drug Class and Agents Anti-estrogens L02B A01 Tamoxifen L02B B L02B B01 Anti -androgens Flutamide L02B B03 Bicalutamide L02B G Enzyme inhibitors L02B G03 Anastrozole L02B G04 Letrozole L02B G06 Exemestane L03A A Colony stimulating factors L03A A02 Filgrastim L03A A10 Lenograstim L03A B Interferons L03A B04 Interferon alfa-2a L03A B05 Interferon alfa-2b L03A B07 Interferon beta-1a L03A B08 Interferon beta-1b L03A B10 Peginterferon alfa-2b L03A B11 Peginterferon alfa-2a Malaysian Statistics on Medicines 2006 2006 85 Public Private Total 0.1664 0.0613 0.2277 Public Private Total Public Private Total 0.0018 0.0007 0.0025 0.0053 0.001 0.0063 Public Private Total Public Private Total Public Private Total 0.0067 0.0043 0.011 0.0055 0.0051 0.0106 0.0006 0.0005 0.0011 Public Private Total Public Private Total 0.0018 0.0006 0.0024 0.0001 <0.0001 0.0002 Public Private Total Public Private Total Public Private Total Public Private Total Public Private Total Public Private Total 0.0005 <0.0001 0.0005 0.0043 <0.0001 0.0044 0.0042 0.0042 <0.0001 <0.0001 <0.0001 0.0016 0.0013 0.0029 0.0023 0.0036 0.0059 Malaysian Statistics on Medicines 2006 CHAPTER 17: USE OF SYSTEMIC CORTICOSTEROIDS AND IMMUNOSUPPRESIVE AGENTS ATC L03A X Drug Class and Agents Other cytokines and immunomodulators L03A X03 BCG vaccine L04A A Selective immunosuppressive agents L04A A01 Ciclosporin L04A A02 Muromonab-CD3 L04A A05 Tacrolimus L04A A06 Mycophenolic acid L04A A08 Daclizumab L04A A09 Basiliximab L04A A10 Sirolimus L04A A11 Etanercept L04A A12 Infliximab L04A A13 Leflunomide L04A A21 Efali zumab L04A X Other immunosuppressive agents L04A X01 Azathioprine L04A X02 Thalidomide L04A X03 Methotrexate 86 2006 Public Private Total 5.3237 0.8046 6.1283 Public Private Total Public Private Total Public Private Total Public Private Total Public Private Total Public Private Total Public Private Total Public Private Total Public Private Total Public Private Total Public Private Total 0.0519 0.003 0.0549 0.0049 0.0002 0.0051 0.0157 0.0046 0.0203 <0.0001 <0.0001 <0.0001 0.0009 0.001 <0.0001 0.0036 0.0037 0.0077 0.0069 0.0146 <0.0001 <0.0001 Public Private Total Public Private Total Public Private 0.0856 0.0084 0.0939 0.0015 0.0012 0.0028 0.0036 CHAPTER 17: USE OF SYSTEMIC CORTICOSTEROIDS AND IMMUNOSUPPRESIVE AGENTS Malaysian Statistics on Medicines 2006 References: 1. Hooi LS, Lela Yasmin Mansor (eds). 3rd report of the National Transplant Registry Malaysia 2006. Kuala Lumpur 2007. Chapter 5. Renal Transplantation from http://www.mstorg.my/ntrSite publications_3rdReport2006.htm accessed on 3 January 2009. 87 CHAPTER 18: USE OF MEDICINES FOR RHEUMATOLOGICAL AND BONE DISORDERS Malaysian Statistics on Medicines 2006 Edited by: Ramanathan R1, Ahmad TA2, Ling HT1, Chew CS1, Aizura AR1 1. Raja Permaisuri Bainun Hospital, Ipoh, 2. Sultanah Nur Zahirah Hospital, Kuala Terengganu Antiinflammatory and antirheumatic products ranked 9th place as the most used drugs by therapeutic group in Malaysia in 2006 (10DDD/1000 population/day) with estimated 1% population utilising them. The acetic acid derivatives and related substances were the most used NSAIDs by drug class (4.05DDD/1000 population/day) followed by the Fenamates (2.68), Coxibs (1.27) and Oxicams (1.06). Diclofenac acid was the most consumed NSAID (1.47 and 2.12DDD/1000 population/day, public and private sectors respectively). The second commonest NSAID used was mefenamic acid (total DDD 2.68). The newer group, called Coxibs (DDD 1.265) with supposedly less side effects such as Etoricoxib (DDD 0.67) was mainly used by private hospitals (91%) while Celecoxib was equally used in the private and public hospitals. In Australia, Oxicams (DDD 8.679) were the highest prescribed, followed closely by Coxibs (DDD 7.250) and acetic acid derivatives (DDD 6.224). [1] Better GIT profile is probably why Cox-2 selective inhibitors are popular nowadays. Anti-Rheumatic Nimesulide was withdrawn from public hospitals due to the side effects of liver failure. Newer DMARD’S had reduced the use of Penicillamine by 50%. Muscle relaxants were prescribed 10 fold more by the private sector (examples: Chlorzoxazone and Orphenadrine), probably to supplement the action of NSAIDs. The public hospitals used Baclofen more so to treat non-inflammatory muscle spasms eg, in celebral palsy. Dantrolene, although a muscle relaxant, was reserved for malignant hyperthermia and is rarely used in Malaysia. Gout was treated with allopurinol (DDD 1.32) with 73% use by the public sector and caution regarding its gastric side effects and worsening of symptoms during acute phase use, need to be emphasised. Greater demand in usage of anti-osteoporosis drugs is expected with increasing lifespan. The three commonest drugs used in 2006 were the bisphosphonates, followed by Selective Estrogen Receptor Modulators (SERMs) and calcitonin groups. The weekly or monthly dosing of bisphophonates had made their usage popular. Strontium and parathyroid hormone have emerged as newer drugs for this condition. Bisphophonates are said to remain in the body forever. Long term studies may show its safety profile in time to come. Table 18.1: Use of Drugs for Rheumatological and Bone disorders, in DDD/1000 population/day 2006 ATC Drug Class 2006 G03X C H05B A M01 M03 M04 M05 Selective estrogen receptor modulators Calcitonin preparations ANTIINFLAMMATORY AND ANTIR HEUMATIC PRODUCTS MUSCLE RELAXANTS ANTIGOUT PREPARATIONS DRUGS FOR TREATMENT OF BONE DISEASES 0.1293 0.0058 10.0035 0.6131 1.5347 0.4399 Table 18.2.1: Use of Non-Steroidal Anti-Inflammatory drugs by Drug Class, in DDD/1000 population/day 2006 ATC Drug Class and Agents 2006 M01A B M01A C M01A E M01A G M01A H M01A X M01C C Acetic acid derivatives and related substances Oxicams Propionic acid derivatives Fenamates Coxibs Other antiinflammatory and antirheumatic agents, non-steroids Penicillamine and similar agents 89 4.0492 1.0649 0.8283 2.6834 1.265 0.1078 0.005 Malaysian Statistics on Medicines 2006 CHAPTER 18: USE OF MEDICINES FOR RHEUMATOLOGICAL AND BONE DISORDERS Table 18.2.2: Use of Non-Steroidal Anti-Inflammatory drugs by Drug Class and Agents, in DDD/1000 population/day 2006 ATC M01A B Drug Class and Agents Acetic acid derivatives and related substances M01A B01 Indometacin M01A B02 Sulindac M01A B05 Diclofenac M01A B15 Ketorolac M01A C Oxicams M01A C01 Piroxicam M01A C02 Tenoxicam M01A C06 Meloxicam M01A E Propionic acid derivatives M01A E01 Ibuprofen M01A E02 Naproxen M01A E03 Ketoprofen M01A G Fenamates M01A G01 Mefenamic acid M01A H Coxibs M01A H01 Celecoxib M01A H02 Rofecoxib M01A H03 Valdecoxib 90 2006 Public Private Total Public Private Total Public Private Total Public Private Total 0.3642 0.0897 0.4539 <0.0001 <0.0001 1.4652 2.1248 3.59 0.0007 0.0045 0.0052 Public Private Total Public Private Total Public Private Total 0.0538 0.4298 0.4836 0.0001 0.0372 0.0373 0.1999 0.3441 0.5441 Public Private Total Public Private Total Public Private Total 0.1589 0.2338 0.3927 0.0981 0.3202 0.4184 0.0106 0.0066 0.0172 Public Private Total 1.2609 1.4224 2.6834 Public Private Total Public Private Total Publ ic Private Total 0.2733 0.3152 0.5885 0.0014 0.0014 CHAPTER 18: USE OF MEDICINES FOR RHEUMATOLOGICAL AND BONE DISORDERS Malaysian Statistics on Medicines 2006 ATC Drug Class and Agents 2006 M01A H04 Parecoxib 0.0008 0.0038 0.0046 0.0604 0.6101 0.6705 M01A X Public Private Total Etoricoxib Public Private Total Other antiinflammatory and antirheumatic agents, non-steroids M01A X17 Nimesulide Public Private Total 0.1078 0.1078 Public Private Total 0.0048 0.0002 0.005 M01A H05 M01C C Penicillamine and similar agents M01C C01 Penicillamine Table 18.3.1: Use of Muscle relaxants by Drug Class and Agents, in DDD/1000 population/day 2006 ATC Drug Class and Agents 2006 M03B MUSCLE RELAXANTS, CENTRALLY ACTING AGENTS M03B B52 Chlormezanone, combinations excl. psycholeptics M03B B53 Chlorzoxazone, combinations excl. psycholeptics M03B C01 Orphenadrine (citrate) M03B X01 Baclofen M03C MUSCLE RELAXANTS, DIRECTLY ACTING AGENTS M03C A01 Dantrolene Public Private Total Public Private Total Public Private Total Public Private Total 0.056 0.056 0.4021 0.4021 0.0153 0.0848 0.1001 0.0504 0.0044 0.0548 Public Private Total - Table 18.4.1: Use of Anti-Gout preparations by Drug Class, in DDD/1000 population/day 2006 ATC M04A Drug Class and Agents ANTIGOUT PREPARATIONS M04A A01 Allopurinol M04A B 01 Probenecid M04A C01 Colchicine 2006 Public Private Total Public Private Total Public Private Total 91 0.9627 0.3601 1.3227 0.0004 0.0031 0.0036 0.0664 0.1421 0.2084 Malaysian Statistics on Medicines 2006 CHAPTER 18: USE OF MEDICINES FOR RHEUMATOLOGICAL AND BONE DISORDERS Table 18.5.1: Use of Bone diseases therapy by Drug Class, in DDD/1000 population/day 2006 ATC Drug Class and Agents 2006 M05 DRUGS FOR TREATMENT OF BONE DISEASES M05B A01 Etidronic acid M05B A02 Clodronic acid M05B A03 Pamidronic acid M05B A04 Alendronic acid M05B A06 Ibandronic acid M05B A07 Risedronic acid M05B A08 Zoledronic acid M05B B03 Alendronic acid and cholecalciferol Public Private Total Public Private Total Public Private Total Public Private Total Public Private Total Public Private Total Public Private 0.0005 0.0005 0.0018 0.002 0.0038 0.0003 <0.0001 0.0004 0.257 0.1148 0.3718 <0.0001 <0.0001 0.0036 0.0211 0.0247 <0.00 01 <0.0001 Total 0.0002 Public Private Total 0.0004 0.038 0.0385 Table 18.6.1: Use of Selective Estrogen Receptor Modulators by Drug Class, in DDD/1000 population/day 2006 ATC Drug Class and Agents 2006 G03 SEX HORMONES AND MODULATORS OF THE GENITAL SYSTEM G03X C01 Raloxifene Public Private Total 0.0646 0.0647 0.1293 Table 18.7.1: Use Calcitonin preparations of by Drug Class, in DDD/1000 population/day 2006 ATC H05 Drug Class and Agents CALCIUM HOMEOSTASIS H05B A01 Calcitonin (salmon synthetic) 2006 Public Private Total References: 1. National Health Survey: Use of Medications, Australia 2006. 2. Malaysian Statistics on Medicines 2005. 92 0.0044 0.0013 0.0058 CHAPTER 19 USE OF OPIOID ANALGESICS Malaysian Statistics on Medicines 2006 Edited by: Mary SC1, Marzida M2, Choy YC3, Faizah AR1, Norliza MA1 1. Selayang Hospital, 2. University of Malaya Medical Centre, 3. Universiti Kebangsaan Malaysia Medical Centre Drugs used for pain control belong to the following subgroups of the ATC classification: anti-inflammatory products, opioids, analgesics and antipyretics. This chapter covers only opioid analgesics. The total opioid consumption in Malaysia in 2006 was 0.7268DDD/1000 population/day. This figure is very much lower than the opioid consumption in the Nordic countries [1], which ranged from 14.0DDD/1000 population/day in Finland to 21.8DDD/1000 population /day in Sweden. Weak opioids were more commonly used than strong opioids. Of the weak opioids, tramadol was the most common, followed closely by codeine and its combinations. The most commonly used strong opioid was morphine, which had much higher use than pethidine, fentanyl and oxycodone. The combined DDD/1000 population/day of the weak opioids (dihydrocodeine, codeine, tramadol and tramadol combinations) was 0.5164, which is more than double that of the strong opioids (morphine, oxycodone, pethidine and fentanyl) which totaled to 0.2084. This pattern is different from the Nordic countries [1] where the total consumption of strong opioids was higher than that of weak opioids. In Malaysia, tramadol, tramadol combinations and codeine combinations comprise the main bulk of the weak opioids that were consumed. These drugs are not controlled under the Dangerous Drugs Act (DDA), and have lower risk of respiratory depression and addiction, thus accounting for their popularity compared to the other opioids. Data from the International Narcotics Control Board (INCB) [2] for opioid consumption in Malaysia showed that in the 1990s there was an increasing trend in morphine consumption which showed plateau after the year 2000, when the newer opioids like fentanyl and oxycodone became available; the consumption of these new opioids is still increasing. This overall increased consumption in opioids probably reflects an increased awareness regarding the use of opioids to control chronic cancer pain. This is supported by the data obtained from this study, as the DDD/1000 population/day of the oral form of morphine (usually used for chronic and cancer pain) is 5 times that of the DDD for the parenteral form (used for anaesthesia and acute pain). Fentanyl is much less used than morphine, and this data only includes the transdermal form, thus reflecting only its use for chronic cancer pain. The use of morphine in the public sector is more than 10 times that in the private sector - this probably reflects the fact that the majority of patients with advanced cancer are treated in the public sector, where oral morphine is used as the mainstay of analgesia for chronic cancer pain. Table 19.1: Use of Analgesics by Drug Class, in DDD/1000 population/day 2006 ATC Drug Class N02A OPIOIDS 2006 0.7268 Table 19.1.2: Use of Analgesics by Drug Class, in DDD/1000 population/day 2006 ATC Drug Class 2006 N02A A N02A B N02A D N02A F N02A X Natural Opium alkaloids Phenylpiperidine derivatives Benzomorphone derivatives Morphinan derivatives Other opioids 0.4139 0.0226 <0.0001 0.0019 0.2883 93 CHAPTER 19 USE OF OPIOID ANALGESICS Malaysian Statistics on Medicines 2006 Table 19.2: Use of Opioid Analgesics by Drug Class, agents and Administration Route, in DDD/1000population/day 2006 ATC Drug Class and Agents Year AdmRCodeO AdmRCodeP N02A A Natural opium alkaloids N02A A01 Morphine N02A A05 Oxycodone N02A A08 Dihydrocodeine N02A A59 Codeine, combinations excl. psycholeptics N02A B Phenylpiperidine derivatives N02A B02 Pethidine N02A B03 Fentanyl N02A D Benzomorphan derivatives N02A D01 Pentazocine N02A F Morphinan derivatives N02A F02 Nalbuphine N02A X Other opioids N02A X02 Tramadol N02A X52 Tramadol, combinations Total Public Private Total Public Private Total Public Private Total Public 0.1474 0.0032 0.1506 0.0004 0.0004 0.0008 0.0161 0.0187 0.0348 - 0.0283 0.0062 0.0345 - 0.1757 0.0094 0.185 0.0004 0.0004 0.0008 0.0161 0.0187 0.0348 - Private Total 0.1933 0.1933 - 0.1933 0.1933 Public Private Total Public - 0.0085 0.0088 0.0173 Private Total - 0.0085 0.0088 0.0173 AdmRCodeTD 0.0048 0.0005 0.0053 Public Private Total - AdmRCodeP <0.0001 <0.0001 <0.0001 <0.0001 Public Private Total - 0.0013 0.0006 0.0019 0.0013 0.0006 0.0019 Public Private Total Public Private Total 0.146 0.0399 0.1859 0.0003 0.0907 0.091 0.0084 0.003 0.0114 - 0.1544 0.0429 0.1973 0.0003 0.0907 0.091 0.0048 0.0005 0.0053 References: 1. Medicines consumption in the Nordic countries 1999-2003. Nordic Medico Statistical Committee 2004; 2004:Copenhagen. 2. International Narcotics Control Board; United Nations population data (Malaysia), by Pain & Policy Studies Group, University of Wisconsin/WHO Collaborating Center, 2008. 94 CHAPTER 20 USE OF MEDICINES FOR NEUROLOGICAL DISORDERS Malaysian Statistics on Medicines 2006 Edited by: Zariah AA1, Hanip R2, Raymond AA3, Norhasyimah AR1, Azrinorwaty Z2 1. Sultanah Nur Zahirah Hospital, Kuala Terengganu, 2. Kuala Lumpur Hospital, 3. Universiti Kebangsaan Malaysia Medical Centre There were 4 main categories of neurological drug groups being analysed for the year 2006. These included the anticonvulsants, drugs for Parkinson’s disease, drugs for dementia and the anti-migraine preparations. The largest category consisted of the anticonvulsants with the total utilisation at 1.5DDD/1000 population/day. This translated to a rough estimate of about 0.15% of our population having epilepsy. This estimated data is slightly lower compared to data from developed countries which gave a range between 0.5% and 1%. The most commonly prescribed drugs for both public and private hospitals were phenytoin (0.5DDD/1000 population/day), sodium valproate (0.4) and carbamazepine (0.3). The first three drugs have traditionally been used as first line drugs for generalised tonic clonic seizures. Although phenytoin has not been a popular drug for many clinicians worldwide, surprisingly it is still commonly prescribed by both the public and private sector doctors in our country. Its usage has been minimal especially in developed countries like the UK and Scandinavia, due to its very narrow toxicity range and its hideous side effects of hirsutism in females. In the local consensus guidelines on the management of epilepsy, phenytoin is recommended as the second and not first choice for generalised seizure due to similar reason. The most probable reasons for its relatively high usage locally are likely due to its cost, availability and partly contributed by the wide use in the elderly with post stroke epilepsy. It also has a major role in the treatment of status epilepticus. Sodium valproate being a versatile drug is the treatment of choice as monotherapy or adjunctive therapy in both partial and generalised seizures. Carbamazepine despite of having its greatest risk of causing Steven-Johnsons syndrome, was almost as popular, being one of the treatment of choice for women of child bearing age due to its comparatively lower risk of teratogenecity. Use of phenobarbitone (0.1), clonazepam (0.04), and primidone (0.001) was limited most likely related to its sedative side effect particularly with clonazepam. Benzodiazepines however, have a particularly prominent role in myoclonus and movement disorders. Among the newer anticonvulsants, lamotrigine (0.04), gabapentin (0.03) and levetiracetam (0.01) were more commonly used compared to others like topiramate (0.006), oxcarbazepine (0.003) and vigabatrin (0.0004). Gabapentin usage is more related to neuropathic pain rather than as an anticonvulsant. Vigabatrin unlike Lamotrigine, Levetiracetam, Topiramate and Oxcarbazepine is currently indicated for second line use in patients with refractory partial epilepsy. Overall usage for the newer AEDs is low due to their higher cost and specialist level prescribing rights. Anticonvulsant usage in private practice is very much lower with both the traditional as well as the newer drugs. This probably reflects the populations’ preference in seeking treatment at public hospitals. The most likely reason for this would have to be the high cost of these medications. The trend in prescribing AED in Australia is similar (see Table 20.7) whereby there is a higher usage of the conventional/older AED like valproic acid (3.6) and carbamazepine (1.89) and there was lower usage of phenytoin (1.65). In descending order of frequency, the most commonly used newer anticonvulsants were lamotrigine (0.98), followed by gabapentin (0.48), levetiracetam (0.4), topiramate (0.27), oxcarbazepine (0.06) and vigabatrin (0.054). In the group, drugs used for Parkinson’s disease, there were 5 main classes of drugs available. They were the levodopa (+ peripheral dopa decarboxylase inhibitors), dopamine agonists, anticholinergics/antimuscarinics, amantadine and the enzyme inhibitors (monoamine oxidase type B inhibitors, catechol-o-methyl transferase 95 Malaysian Statistics on Medicines 2006 CHAPTER 20 USE OF MEDICINES FOR NEUROLOGICAL DISORDERS inhibitors. Artane was the most commonly prescribed drug with a DDD/1000 population/day of 0.6. Its popularity was likely due to its availability, cost, usefulness in reducing tremor and rigidity and served as an alternative to reduce risk of development of motor complications associated with levodopa therapy. Levodopa (+ peripheral dopa decarboxylase inhibitors) although is the gold standard and the most effective drug therapy in Parkinson’s disease came second in its usage at 0.16 DDD/1000 population/day. Stalevo, a 3-in-one preparation with levodopa, carbidopa and entacapone showed very little usage at 0.0017DDD/1000 population/day. It is currently not available in the Ministry of Health (public sector) Among the dopamine agonists, the commonly used drugs in descending order of frequency were; piribedil (0.009), bromocriptine (0.006), ropinirole (0.001) and pramipexole (0.0003). Bromocriptine and piribedil both ergot derived DA had been in the market longer than the other newer dopamine agonists. Pramipexole was only made available in Malaysia in June 2006. Hence in spite of the current practice of using DA as first choice in de novo and young parkinsonian patients and with possible neuroprotective effects, the non availability and cost were the likely factors for their low usage. Amantadine (0.007), a tricyclic amine was used previously as an antiviral. It was mainly used in levodopa induced dyskinesias and hence has a limited role in PD therapy. Among the enzyme inhibitors, selegiline (0.06) had been available in Malaysia for many years and usually used in the early stage of PD, whereas comtan (0.012) was a relatively newer addition, used in combination with levodopa. The prescribing practice in Australia differed slightly (see Table 20.8), with the levodopa group (1.43) having the higher usage compared to the anticholinergics. Among the anticholinergic, unlike in Malaysia where benzhexol was very popular, benzatropine (0.49) had a higher usage. The dopamine agonists both older and newer ones together with amantadine showed the lowest ratings (0.02 for bromocriptine, ropinirole, pramipexole and 0.003 for amantadine). Their use of comtan (0.1) and stalevo (0.05) were much higher. In dementia, drugs available for cognitive improvement were the cholinesterase inhibitors, usage at 0.02DDD/1000 population/day and the NMDA receptor antagonist, memantine usage at 0.001DDD/1000 population/day. In 2006 and till currently memantine and galantamine are still unavailable in the public sector. Although an estimated 5 to 10% of the adult population age 65 years and older is affected by a dementia disorder, lack of awareness by both the public and health care professionals could explain the least usage of these drugs (0.02) among the four subgroup neurological disorders surveyed. No data from Australia was available for comparison. The total use of anti-migraine preparations in 2006 in Malaysia was 0.0689DDD/1000 population/day. The most utilised class of drug was ergot alkaloid (0.0337DDD/1000 population/day), followed by pizotifen (0.0265DDD/1000 population/day) and selective serotonin (5HT1) agonist, sumatriptan (0.0087DDD/1000 population/day). Ergot alkaloids constituted 48.9% by drug class with the breakdown of ergotamine combinations excluding psycholeptics (94%), ergotamine combinations with psycholeptics (5.6%) and ergotamine (0.4%). Ergot alkaloid had not been approved and was unavailable in public hospitals hence its low usage in acute migraine attack. However, it had its usage in private practice despite the alarming side effects with chronic use. The only available ergot combination in Malaysia in 2006 was Cafergot® which contained ergotamine and caffeine. Sumatriptan used in acute attacks showed a usage of 0.009 DDD/1000 population/day, being used more in the private practice (0.006) compared to public hospitals (0.002). There was no survey made on other drugs for acute attacks like paracetamol, cox-2 inhibitors, NSAIDs, opioids or corticosteroids. In Australia, sumatriptan showed the highest usage amongst the drugs for aborting acute attacks, followed by the ergot alkaloid methysergide (0.03), the newer triptans, zolmitriptans (0.03) and naratriptan (0.02). Pizotifen used as migraine prophylaxis was the only prophylaxis surveyed with usage of 0.002DDD/1000 population/day. It would be interesting to look at the results of other migraine prophylaxis which was not 96 CHAPTER 20 USE OF MEDICINES FOR NEUROLOGICAL DISORDERS Malaysian Statistics on Medicines 2006 surveyed, including the newer anticonvulsants like topiramate, levetiracetam as well as the conventional choices like beta blockers and calcium channel blockers. As such, analyses as to the practice of use of antimigraine drugs are rather limited due to the restricted choices of drugs surveyed. Table 20.1: Use of Drugs for Neurological Disorder, in DDD/1000 population/day 2006 ATC Drug Class 2006 N02C N03 N04 N06D N07 ANTIMIGRAINE PREPARATIONS ANTIEPILEPTICS ANTIPARKINSON DRUGS ANTIDEMENTIA DRUGS OTHER NERVOUS SYSTEM DRUGS 0.0689 1.4992 0.882 0.0258 0.9054 Table 20.2.1: Use of Analgesics by Drug Class, in DDD/1000 population/day 2006 ATC Drug Class 2006 N02C N02C A N02C C N02C X ANTIMIGRAINE PREPARATIONS Ergot alkaloids Selective serotonin (5HT1) agonists Other antimigraine preparations 0.0689 0.0337 0.0087 0.0265 Table 20.2.2: Use of Analgesics by Drug Class and Agents, in DDD/1000 population/day 2006 ATC N02C A Drug Class and Agents Ergot alkaloids 2006 N02C A02 Ergotamine N02C A52 Ergotamine, combinations excl. psycholeptics N02C A72 Ergotamine, combinations with psycholeptics N02C C Selective serotonin (5HT1) agonists N02C C01 Sumatriptan N02C X Other antimigraine preparations N02C X01 Pizotifen Public Private Total Pub lic Private Total Public Private Total 0.0001 0.0001 0.0003 0.0314 0.0317 0.0019 0.0019 Public Private Total 0.002 0.0067 0.0087 Public Private Total 0.0183 0.0082 0.0265 Table 20.3.1: Use of Anti-Epileptics by Drug Class, in DDD/1000 population/day 2006 ATC Drug Class 2006 N03A N03A A N03A B N03A D N03A E N03A F N03A G N03A X ANTIEPILEPTICS Barbiturates and derivatives Hydantoin derivatives Succinimide derivatives Benzodiazepine derivatives Carboxamide derivatives Fatty acid derivatives Other antiepileptics 1.4992 0.1231 0.5077 0.0483 0.3172 0.3985 0.1044 97 Malaysian Statistics on Medicines 2006 CHAPTER 20 USE OF MEDICINES FOR NEUROLOGICAL DISORDERS Table 20.3.2: Use of Antiepileptics by Drug Class and Agents, in DDD/1000 population/day 2006 ATC N03A A Drug Class and Agents Barbiturates and derivatives N03A A02 Phenobarbital N03A A03 Primidone N03A B Hydantoin derivatives N03A B02 Phenytoin N03A D Succinimide derivatives N03A D01 Ethosuximide N03A E Benzodiazepine derivatives N03A E01 Clonazepam N03A F Carboxamide derivatives N03A F01 Carbamazepine N03A F02 Oxcarbazepine N03A G Fatty acid derivatives N03A G01 Valproic acid N03A G04 Vigabatrin N03A X Other antiepileptics N03A X0 9 Lamotrigine N03A X11 Topiramate N03A X12 Gabapentin N03A X14 Levetiracetam 2006 98 Public Private Total Public Private Total 0.1062 0.0153 0.1215 0.0013 0.0002 0.0015 Public Private Total 0.4641 0.0436 0.5077 Public Private Total - Public Private Total 0.0399 0.0085 0.0483 Public Private Total Public Private Total 0.2905 0.0236 0.3142 0.0002 0.0027 0.003 Public Private Total Public Private Total 0.3673 0.0308 0.3981 0.0001 0.0003 0.0004 Public Private Total Public Private Total Public Private Total Public Private Total 0.038 0.0033 0.0412 0.0058 0.0003 0.0061 0.0221 0.0159 0.038 0.0101 0.0089 0.0191 CHAPTER 20 USE OF MEDICINES FOR NEUROLOGICAL DISORDERS Malaysian Statistics on Medicines 2006 Table 20.4.1: Use of Antiparkinson by Drug Class, in DDD/1000 population/day 2006 ATC Drug Class N04A N04A A N04A B N04A C N04B N04B A N04B B N04B C N04B D N04B X ANTICHOLINERGIC AGENTS Tertiary amines Ethers chemically close to antihistamines Ethers of tropine or tropine derivatives DOPAMINERGIC AGENTS Dopa and dopa derivatives Adamantane derivatives Dopamine agonists Monoamine oxidase B inhibitors Other dopaminergic agents 2006 0.6121 0.6094 0.0004 0.0023 0.2698 0.1739 0.0066 0.0171 0.0604 0.0118 Table 20.4.2: Use of Antiparkinson by Drug Class and Agents, in DDD/1000 population/day 2006 ATC Drug Class and Agents 2006 N04A A Tertiary amines N04A A01 Trihexyphenidyl N04A A04 Procyclidine N04A B Ethers chemically close to antihistamines N04A B02 Orphenadrine (chloride) N04A C Ethers of tropine or tropine derivatives N04A C01 Benzatropine N04B A Dopa and dopa derivatives N04B A02 Levodopa and decarboxylase inhibitor N04B A03 Levodopa, decarboxylase inhibitor and COMT inhibitor N04B B Adamantane derivatives N04B B01 Amantadine N04B C Dopamine agonists N04B C01 Bromocriptine N04B C04 Ropinirole N04B C05 Pramipexole 99 Public Private Total Public Private Total 0.5887 0.0204 0.6091 0.0003 <0.0001 0.0003 Public Private Total 0.0004 0.0004 Public Private Total 0.002 0.0003 0.0023 Public Private Total Public Private Total 0.1549 0.0173 0.1722 0.0008 0.0009 0.0017 Public Private Total 0.0029 0.0036 0.0066 Public Private Total Publ ic Private Total Public Private Total 0.0061 0.0003 0.0063 0.0006 0.0006 0.0012 0.0003 0.0003 Malaysian Statistics on Medicines 2006 CHAPTER 20 USE OF MEDICINES FOR NEUROLOGICAL DISORDERS ATC Drug Class and Agents N04B C08 Piribedil N04B D Monoamine oxidase B inhibitors N04B D01 Selegiline N04B X02 Entacapone 2006 Public Private Total 0.0082 0.0011 0.0093 Public Private Total Public Private Total 0.054 0.0065 0.0604 0.0109 0.0009 0.0118 Table 20.5.1: Use of Antidementia Drugs by Drugs Class, in DDD/1000 population/day 2006 ATC Drug Class and Agents 2006 N06D N06D A N06D X ANTIDEMENTIA DRUGS Anticholinesterases Other anti-dementia drugs 0.0258 0.0247 0.0011 Table 20.5.2: Use of Antidementia Drugs by Drugs Class and Agents, in DDD/1000 population/day 2006 ATC N06D A Drug Class and Agents Anticholinesterases N06D A02 Donepezil N06D A03 Rivastigmine N06D A04 Galantamine N06D X Other antidementia drugs N06D X01 Memantine 2006 Publi c Private Total Public Private Total Public Private Total 0.0102 0.0032 0.0134 0.006 0.0006 0.0066 0.0047 0.0047 Public Private Total 0.0009 0.0001 0.0011 Table 20.6.1: Use of Other Nervous System Drugs by Drug Class, in DDD/1000 population/day 2006 ATC Drug Class and Agents 2006 N07A N07A A N07C N07C A N07X N07X X PARASYMPATHOMIMETICS Anticholinesterases ANTIVERTIGO PREPARATIONS Antivertigo preparations OTHER NERVOUS SYSTEM DRUGS Other nervous system drugs 0.1268 0.1268 0.778 6 0.7786 <0.0001 <0.0001 100 CHAPTER 20 USE OF MEDICINES FOR NEUROLOGICAL DISORDERS Malaysian Statistics on Medicines 2006 Table 20.6.2: Use of Other Nervous System Drugs by Drug Class and Agents, in DDD/1000 population/day 2006 ATC Drug Class and Agents 2006 N07A A Anticholinesterases N07A A01 Neostigmine N07A A02 Pyridostigmine N07A A03 Distigmine N07C A A ntivertigo preparations N07C A01 Betahistine N07C A02 Cinnarizine N07C A03 Flunarizine N07X X Other nervous system drugs N07X X02 Riluzole Public Private Total Public Private Total Public Private Total 0.0294 0.0213 0.0507 0.0704 0.0056 0.0761 <0.0001 <0.0001 Public Private Total Public Private Total Public Private Tota l 0.1257 0.242 0.3677 0.1156 0.2004 0.316 0.0183 0.0766 0.0949 Public Private Total <0.0001 <0.0001 Table 20.7: Use of drugs for epilepsy in DDD/1000 population/day comparing use in Malaysia and Australia for the year 2006 Drug Malaysia Australia Phenobarbitone Primidone Clonazepam Carbamazepine Oxcarbazepine Valproic Acid Vigabatrin Lamotrigine Public/Subsidized Private/Survey TOTAL Public/Subsidized Private/Survey TOTAL Public/Subsidized Private/S urvey TOTAL Public/Subsidized Private/Survey TOTAL Public/Subsidized Private/Survey TOTAL Public/Subsidized Private/Survey TOTAL Public/Subsidized Private/Survey TOTAL Public/Subsidized Private/Survey TOTAL 0.1062 0.0153 0.1215 0.0013 0.0002 0.0015 0.0399 0.0085 0.0484 0.2905 0.0236 0.3141 0.0002 0.0027 0.0029 0.3673 0.0308 0.3981 0.0001 0.0003 0.0004 0.038 0.0033 0.0413 101 0.110 0.020 0.130 0.092 0.001 0.093 0.163 0.205 0.368 1.838 0.048 1.886 0.058 0.000 0.058 3.603 0.039 3.642 0.054 0.000 0.054 0.792 0.18 8 0.980 Malaysian Statistics on Medicines 2006 CHAPTER 20 USE OF MEDICINES FOR NEUROLOGICAL DISORDERS Drug Topiramate Gabapentin Levetiracetam Public/Subsidized Private/Survey TOTAL Public/Subsidized Private/Survey TOTAL Public/Subsidized Private/Survey TOTAL Malaysia Australia 0.0058 0.0003 0.0061 0.0221 0.0159 0.0380 0.010 1 0.0089 0.02 0.259 0.010 0.269 0.302 0.176 0.478 0.392 0.003 0.4 Table 20.8: Use of drugs for Parkinson’s disease in DDD/1000 population/day comparing use in Malaysia and Australia for the year 2006 Drug Malaysia Australia Artane Procyclidine Ophenadrine Benzatropine Levodopa & Decarboxylase Inhibitor Stalevo Amantadine Bromocriptine Ropinirole Pramipexole Piribedil Selegiline Comtan Public/Subsidized Private/Survey Total Public/Subsidized Private/Survey Total Public/Subsidized Private/Survey Total Public/Subsidiz ed Private/Survey Total Public/Subsidized 0.59 0.02 0.61 0.0003 <0.0001 0.13 0.008 0.13 - 0.0004 0.0004 0.002 0.0003 - Private/Survey Total Public/Subsidized Private/Survey Total Public/Subsidized Private/Survey Total Public/Subsidized Private/Survey Total Public/Subsidized Private/Survey Total Public/Subsidized Private/Survey Total Public/Subsidized Private/Survey Total Public/Subsidized Private/Survey Total Public/Subsidized Private/Survey Total 0.017 0.172 0.0008 0.0009 0.0017 0.003 0.004 0.007 0.006 0.0003 0.0063 0.0006 0.0006 0.0012 0.0003 0.0003 0.008 0.001 0.009 0.054 0.0065 0.06 0.011 0.0009 0.012 0.155 References: 1. Malaysian consensus guidelines on the management of epilepsy 2005. 2. British National Formulary September 2007. 3. Malaysian consensus on Parkinson’s disease. 4. Malaysian guidelines on the management of dementia 2003. 5. Malaysian consensus guidelines on the management of headache 2005. 6. Australian statistics on medicine 2006. 102 0.465 0.03 0.49 (Madopar) 0.56 0.002 0.56 0.054 0.000 0.054 0.0 0.003 0.003 0.02 0.000 0.002 0.002 0.002 - 0.102 0.00 0.102 0.097 0.00 0.097 Sinemet 0.87 0.006 0.87 CHAPTER 21 USE OF DRUGS FOR PSYCHIATRIC DISORDERS Malaysian Statistics on Medicines 2006 Edited by: Siti Nor Aizah A1, Salina AA1, Ramli MA2, Suarn S3, Nor Hayati A4, Shamini R3, Noor Ratna N5, Mariam Bintarty R,1 Syed Fadzli SS6 1. Kuala Lumpur Hospital, 2. Selayang Hospital, 3. Bahagia Hospital, Tanjung Rambutan 4. Kajang Hospital, 5. Permai Hospital, Johor Bahru, 6. Pharmaceutical Services Division, MOH. The impact of mental and behavioural disorders does not only affect the individual concerned but extend onto the families and communities. In 2000, it was estimated that neuropsychiatric disorders accounted for 12.3% of Disability Adjusted Life Years (DALYs) [1]. Pharmacotherapy is one of the important treatment modalities in the holistic management of the various psychiatric disorders. Antipsychotics was the group of drugs most consumed, comprising 53%, followed by antidepressants (22%), anxiolytics, hypnotics and sedatives (21%) and drugs used in addictive disorders (4%). In some of the Nordic countries, the hypnotics were among the top 10 most consumed medicines in 2003 [2]. In the same publication, it was notable that the 1999-2003 drug consumption trends indicated that the antipsychotic use was increased by 4-23%; whereas the antidepressants use escalated between 43-66%. Eighty seven percent (87%) of typical antipsychotics were prescribed compared with 13% of atypical antipsychotics. This pattern did not vary much from previous year’s data [3] and the prescribing practice was the reverse in Australia [4]. The use of atypical antipsychotics was higher in the private sector (26%) as compared to the public sector (13%). Although its use is recommended as first line treatment in a number of different psychotic conditions [5, 6], the low usage of atypical antipsychotics locally might be due to its high cost. The Selective Serotonin Reuptake Inhibitors (SSRI) was the highest consumed antidepressant (67%), followed by Non-Selective Monoamine Reuptake Inhibitors (24.30%). The wide discrepancy between the SSRIs and the use of other antidepressants could be due to its favourable safety profile and its approval for indications for not only mood disorders but for anxiety disorders as well [7]. The prescription of the newer antidepressants such as Mirtazapine, Venlafaxine and Duloxetine, among others, categorised under the Other Antidepressants were much lower (7%). The anxiolytics, sedatives and hypnotics were much more widely used in the private sector (69%) comparative to the public sector (31%). This discrepancy could be explained by tendency of patients with anxiety [8] and sleep disorders [9] to seek medical consultations from primary healthcare practitioners. In both facilities, Alprazolam was the most commonly prescribed anxiolytic (N05B); 27% in private and 21% in public. Among the hypnotics and sedatives (N05C); the benzodiazepine derivatives Midazolam was prescribed more in the private sector, whereas usage of benzodiazepine related drug such as Zolpidem was comparable in both sectors. The use of drugs for addictive disorders was slightly higher in the private sector i.e. 56.3%. Drugs used for opioid dependence, Methadone (56%) and Buprenorphine (42%) were widely prescribed. Drugs used for alcohol dependence, Naltrexone; and for nicotine dependence, Nicotine; each only comprised of 1% usage. The low consumption of nicotine (0.0017DDD/1000 population/day) was of concern in up scaling the smoking cessation services considering the prevalence of established smokers in 2006 were 21.5%, of which 23.6% were defined as heavy smokers [10]. 103 Malaysian Statistics on Medicines 2006 CHAPTER 21 USE OF DRUGS FOR PSYCHIATRIC DISORDERS Table 21.1.1: Use of Anti-Psychotics by Drug Class, in DDD/1000 population/day 2006 ATC Drug Class and Agents N05A A N05A B N05A C N05A D N05A E N05A F N05A H N05A K N05A L N05A N N05A X Phenothiazines with aliphatic side-chain Phenothiazines with piperazine structure Phenothiazines with piperidine structure Butyr ophenone derivatives Indole derivatives Thioxanthene derivatives Diazepines, oxazepines and thiazepines Neuroleptics, in tardive dyskinesia Benzamides Lithium Other antipsychotics 2006 0.4881 0.8033 0.0007 0.6728 0.0013 0.0693 0.136 <0.0001 0.31 0.029 0.2061 Table 21.1.2: Use of Anti-Psychotics by Drug Class and Agents, in DDD/1000 population/day 2006 ATC Drug Class and Agents 2006 N05A A Phenothiazines with aliphatic side-chain N05A A01 Chlorpromazine N05A B Phenothiazines with piperazine structure N05A B02 Fluphenazine N05A B03 Perphenazine N05A B04 Prochlorperazine N05A B06 Trifluoperazine N05A C Phenothiazines with piperidine structure N05A C02 Thioridazine N05A D Butyrophenone derivatives N05A D01 Haloperidol N05A E Indole derivatives N05A E04 Ziprasidone N05A F Thioxanthene derivatives N05A F01 Flupentixol N05A F05 Zuclopenthixol 104 Public Private Total 0.4835 0.0046 0.4881 Public Private Total Public Private Total Public Private Total Public Private Total 0.5418 0.0115 0.5534 0.0224 0.0026 0.025 0.0818 0.0318 0.1136 0.1106 0.0009 0.1115 Public Private Total <0.0001 0.0006 0.0007 Public Private Total 0.66 0.0128 0.6728 Public Private Total 0.0003 0.001 0.0013 Public Private Total Public Private Total 0.0205 0.0015 0.022 0.0459 0.0014 0.0473 CHAPTER 21 USE OF DRUGS FOR PSYCHIATRIC DISORDERS ATC N05A H Drug Class and Agents Diazepines, oxazepines and thiazepines N05A H02 Clozapine N05A H03 Olanzapine N05A H04 Quetiapine N05A K Neuroleptics, in tardive dyskinesia N05A K01 Tetrabenazine N05A L Benzamides N05A L01 Sulpiride N05A N Lithium N05A N01 Lithium N05A X Other antipsychotics N05A X08 Risperidone N05A X12 Aripiprazole Malaysian Statistics on Medicines 2006 2006 Public Private Total Public Private Total Public Private Total 0.0887 0.0003 0.089 0.0296 0.0011 0.0307 0.0149 0.0014 0.0163 Public Private Total <0.0001 <0.0001 Public Private Total 0.307 0.003 0.31 Public Private Total 0.0275 0.0014 0.029 Public Private Total Public Private Total 0.2009 0.0034 0.2043 0.0002 0.0017 0.0018 Table 21.2.1: Use of Anti-Depressants by Drug Class, in DDD/1000 population/day 2006 ATC Drug Class and Agents N06A A N06A B N06A F N06A G N06A X Non-selective monoamine reuptake inhibitors Selective serotonin reuptake inhibitors Monoamine oxidase inhibitors, non-selective Monoamine oxidase A inhibitors Other antidepressants 2006 0.2723 0.7504 <0.0001 0.018 0.0792 Table 21.2.2: Use of Anti-Depressants by Drug Class and Agents, in DDD/1000 population/day 2006 ATC Drug Class and Agents 2006 N06A A Non-selective monoamine reuptake inhibitors N06A A02 Imipramine N06A A04 Clomipramine N06A A09 Amitriptyline Public Private Total Public Private Total Public Private Total 105 0.029 0.0046 0.0336 0.0175 0.0011 0.0186 0.0906 0.0479 0.1384 Malaysian Statistics on Medicines 2006 CHAPTER 21 USE OF DRUGS FOR PSYCHIATRIC DISORDERS ATC Drug Class and Agents 2006 N06A A10 Nortriptyline N06A A16 Dosulepin N06A A21 Maprotiline N06A B Selective serotonin reuptake inhibitors N06A B03 Fluoxetine N06A B04 Citalopram N06A B05 Paroxetine N06A B06 Sertraline N06A B08 Fluvoxamine N06A B10 Escitalopram N06A F Monoamine oxidase inhibitors, non-selective N06A F04 Tranylcypromine N06A G Monoamine oxidase A inhibitors N06A G02 Moclobemide N06A X Other antidepressants N06A X03 Mianserin N06A X06 Nefazodone N06A X11 Mirtazapine N06A X14 Tianeptine 106 Public Private Total Public Private Total Public Private Total <0.0001 <0.0001 0.0626 0.0156 0.0782 0.0018 0.0016 0.0034 Public Private Total Public Private Total Public Private Total Public Private Total Public Private Total Public Private Total 0.1119 0.028 0.1399 0.001 0.023 0.024 0.004 0.0073 0.0112 0.2392 0.0526 0.2918 0.1854 0.0276 0.213 0.0425 0.028 0.0705 Public Private Total <0.0001 <0.0001 Public Private Total 0.0171 0.0009 0.018 Public Private Tota l Public Private Total Public Private Total Public Private Total 0.0091 0.0038 0.0129 0.0171 0.0168 0.0339 0.0003 0.0065 0.0068 CHAPTER 21 USE OF DRUGS FOR PSYCHIATRIC DISORDERS ATC Drug Class and Agents N06A X16 Venlafaxine N06A X21 Duloxetine Malaysian Statistics on Medicines 2006 2006 Public Private Total Public Private Total 0.0191 0.0047 0.0238 0.0002 0.0016 0.0018 Table 21.3.1: Use of Anxiolytics, Hypnotics and Sedatives by Drug Class, in DDD/1000 population/day 2006 ATC Drug Class 2006 N05B A N05B B N05C C N05C D N05C F N05C M Benzodiazepine derivatives Diphenylmethane derivatives Aldehydes and derivatives Benzodiazepine derivatives Benzodiazepine related drugs Other hypnotics and sedatives 0.7978 0.1404 0.0139 0.2149 0.1617 <0.0001 Table 21.3.2: Use of Anxiolytics, Hypnotics and Sedatives by Drug Class and Agents, in DDD/1000 population/day 2006 ATC Drug Class and Agents 2006 N05B A Benzodiazepine derivatives N05B A01 Diazepam N05B A02 Chlordiazepoxide N05B A05 Potassium clorazepate N05B A06 Lorazepam N05B A08 Bromazepam N05B A09 Clobazam N05B A12 Alprazolam N05B B Diphenylmethane derivatives N05B B01 Hydroxyzine N05C C Aldehydes and derivatives N05C C01 Chloral hydrate 107 Public Private Total Public Private Total Public Private Total Public Private Total Public Private Total Public Private Total Public Private Total 0.0656 0.1552 0.2209 0.0061 0.0061 0.0195 0.0195 0.0834 0.0939 0.1773 0.0063 0.0219 0.0282 0.0013 0.0128 0.0141 0.0856 0.2461 0.3317 Public Private Total 0.0522 0.0882 0.1404 Public Private Total 0.006 0.008 0.0139 Malaysian Statistics on Medicines 2006 ATC Drug Class and Agents N05C C05 Paraldehyde N05C D Benzodiazepine derivatives N05C D01 Flurazepam N05C D02 Nitrazepam N05C D05 Triazolam N05C D08 Midazolam N05C F Benzodiazepine related drugs N05C F01 Zopiclone N05C F02 CHAPTER 21 USE OF DRUGS FOR PSYCHIATRIC DISORDERS 2006 Zolpidem N05C M Other hypnotics and sedatives N05C M05 Scopolamine Public Private Total <0.0001 <0.0001 <0.0001 Public Private Total Public Private Total Public Private Total Public Private Total 0.0004 0.0004 0.0019 0.0169 0.0189 0.0192 0.0192 0.0524 0.1241 0.1764 Public - Private 0.0292 Total 0.0292 Public Private Total 0.0601 0.0725 0.1325 Public Private Total <0.0001 <0.0001 <0.0001 Table 21.4.1: Use of Drugs used in Additive Disorder by Drug Class, in DDD/1000 population/day 2006 ATC Drug Class and Agents 2006 N07B N07B A N07B B N07B C DRUGS USED IN ADDICTIVE DISORDERS Drugs used in nicotine dependence Drugs used in alcohol dependence Drugs use d in opioid dependence 0.1708 0.0017 0.0014 0.1678 Table 21.4.2: Use of Drugs used in Additive Disorder by Drug Class and Agents, in DDD/1000 population/ day 2006 ATC N07B A Drug Class and Agents Drugs used in nicotine dependence N07B A01 Nicotine N07B B Drugs used in alcohol dependence N07B B04 Naltrexone N07B C Drugs used in opioid dependence N07B C01 Buprenorphine 108 2006 Public Private Total 0.0005 0.0011 0.0017 Public Private Total 0.001 0.0004 0.0014 Public Private Total 0.0018 0.0695 0.0713 CHAPTER 21 USE OF DRUGS FOR PSYCHIATRIC DISORDERS ATC Drug Class and Agents N07B C 02 Methadone N07B C51 Buprenorphine, combinations Malaysian Statistics on Medicines 2006 2006 Public Private Total Public Private Total 0.0713 0.0251 0.0964 <0.0001 <0.0001 References: 1. World Health Report 2001. 2. Nordic Medico Statistico Committee 2004. Medicines Consumption in The Nordic Countries 1999-2003. 3. Pharmaceutical Services Division and the Clinical Research Centre, Ministry of Health, Malaysia 2007. Malaysian Statistics on Medicine 2005. 4. Commonwealth of Australia 2008. Australian Statistics on Medicine 2006. 5. Kane JM, Leucht S, Carpenter D, et al, The Expert Consensus Guideline Series: Optimising pharmacologic treatment of psychotic disorders. J Clin Psychiatry 2003; 64 (Suppl 12):1-100. 6. Weiden PJ, Preskorn SH, Fahnestock PA, et al. Translating the psychopharmacology of antipsychotics to individualized treatment for severe mental illness: A roadmap. J Clin Psychiatry 2006; 68 (Suppl 7):1-46. 7. Stein DJ. Serotonergic Neurocircuitry in Mood and Anxiety Disorders. London, UK. Martin Dunitz Ltd. 2003. 8. Sartorius N, Ustun TB, Lecrubier Y, Wittchen HU. Depression comorbid with anxiety: Results from the WHO study on psychological disorders in primary health care. Br J Psychiatry 1996; 168(Suppl 30):38-43. 9. G Hajak. Insomnia in Primary Care. Sleep 2000; 23 (Suppl 3): S54-S63. 10. Institute for Public Health (IPH) 2008. The Third National Health and Morbidity Survey (NHMS III) 2006, Vol 2, Ministry of Health Malaysia. 109 CHAPTER 22: USE OF MEDICINES FOR OBSTRUCTIVE AIRWAY DISEASES Malaysian Statistics on Medicines 2006 Edited by: Pang YK1, Abdol Malek AZ2, Aziah AM3, Samsinah HH4, Joanne L5, Mat Zuki MJ6, Norhaya R7, Shahirah Z8 1. University of Malaya Medical Centre, 2. Pharmacy, Melaka Hospital, 3. Institute of Respiratory Medicine, Kuala Lumpur Hospital, 4. Department of Pharmacy, University Malaya, 5. Pharmacy, Kuala Lumpur Hospital, 6. Raja Perempuan Zainab II Hospital, Kota Bharu, 7. Sultanah Nur Zahirah Hospital, Kuala Terengganu, 7. Pharmacy, Selayang Hospital In clinical practice, asthma and chronic obstructive pulmonary disease (COPD), classified under obstructive airway diseases, are considered the two common diseases. Many of the drugs used in these diseases are quite similar, although the indications and the effects of drugs may differ considerably between the two. Data reported in this survey were based on the statistics of drug procurement and hence did not differentiate between those used in asthma from those used in COPD. To gain more insight into the prescribing trend and behaviour, it would be more appropriate in the future to separate the usage of drugs for asthma and COPD into the two different diseases. In asthma, inhaled glucocorticoids used as monotherapy or in combination with long-acting ß2 agonist are indicated for maintenance therapy. Use of long-acting ß2 agonists may prevent the need to increase the inhaled dose of glucocorticoids. Inhaled glucocorticoids and long-acting ß2 agonist are also used in patients with COPD, particularly in those with frequent exacerbations and those whose spirometry show significant FEV1 reversibility. On the other hand, short acting ß2 agonists (termed as “rescue” agents) are indicated for relief of acute reversible airway obstruction in patients with asthma and COPD. Based on these recommendations, one would expect that the usage of inhaled glucocorticoids should far exceed that of ß2 agonists; however, in this survey, the usage of ß2 agonists (4.6693) was still higher than that of glucocorticoids (2.3883). This seems to suggest that inhaled glucocorticoids are underused in the treatment of asthma and this might have resulted in many patients with uncontrolled asthma and increase usage of rescue ß2 agonists. Based on this survey, of the various inhaled glucocorticoids, budesonide was the most popular agent used. The usage of ciclesonide was still low as it was a new agent in this group. The latter is used in a small number of patients in government hospitals with specialists. Inhaled salbutamol on the other hand was the most popular ß2 agonist used to relieve symptoms. The use of oral ß2 agonists was still alarmingly high (5.5604). Although the oral route has the advantage of ease and simplicity of administration, in terms of clinical effects this is not the preferred route. This showed that the move to encourage doctors to change the prescription of reliever drugs from oral route to the inhaled method has not yet been very successful. This trend seems to be more deeply entrenched for those in the private sector. Leukotriene receptor antagonists (e.g. montelukast) are recommended for those who have mild to moderate asthma as a monotherapy or used as an add-on for those whose asthma are still not well control despite receiving other agents. This drug is also particularly useful in controlling asthma resulting from certain triggers such as exercise-induced asthma, aspirin-induced asthma and allergen-induced asthma. It is easy to take (oral tablet once at night) but is still quite costly. The survey showed that the private sector tend to use it more often than the public sector. This may be that patients in the private sector could better afford this treatment. The use of montelukast in the public hospitals is restricted by the number of patients allowed to be prescribed the drug. The use of Seretide® (accuhaler) is higher than Symbicort® (turbohaler) which is reflective of current practice. Both these drugs are costly and due to their unique presentation, the patients’ therapeutic outcomes are monitored, either in the ward or, in some government hospitals, during consultation at the Medication Therapy Adherence Clinics (MTAC) by the pharmacists. The new drug for asthma management, omalizumab (an anti-Ig E antibody) was not included in this report as it was not yet available in 2006 in Malaysia. 111 Malaysian Statistics on Medicines 2006 CHAPTER 22: USE OF MEDICINES FOR OBSTRUCTIVE AIRWAY DISEASES Table 22.1: Use of Medicines for Obstructive Airway Diseases by Drug Class, in DDD/1000 population/day 2006 ATC Drug Class and Agents 2006 R03A C R03A K R03B A R03B B R03B C R03C A R03C C R03D A R03D C Selective beta-2-adrenoreceptor agonists Adrenergics and other drugs for obstructive airway diseases Glucocorticoids Anticholinergics Antiallergic agents, excl. corticosteroids Alpha-and beta-adrenoreceptor agonists Selective beta-2-adrenoreceptor agonists Xanthines Leukotriene receptor antagonists 4.6693 1.6081 2.3883 0.5069 0.0496 5.5604 1.5931 0.1436 Table 22.2: Use of Medicines for Obstructive Airway Diseases by Drug Class and Agents, in DDD/1000 population/day 2006 ATC R03A C Drug Class and Agents Selective beta-2-adrenoreceptor agonists R03A C02 Salbutamol R03A C03 Terbutaline R03A C04 Fenoterol R03A C12 Salmeterol R03A C13 Formoterol R03A K Adrenergics and other drugs for obstructive airway diseases R03A K03 Fenoterol and other drugs for obstructive airway diseases R03A K04 Salbutamol and other drugs for obstructive airway diseases R03A K06 Salmeterol and other drugs for obstructive airway diseases R03A K07 Formoterol and other drugs for obstructive airway diseases R03B A Glucocorticoids R03B A01 Beclometasone 112 2006 Public Private Total Public Private Total Public Private Total Public Private Total Public Private Total 4.024 0.3237 4.3477 0.016 2 0.0274 0.0436 0.0073 0.001 0.0083 0.0084 0.0002 0.0086 0.2551 0.006 0.2611 Public Private Total Public Private Total Public Private Total Public Private Total 0.0226 0.0226 0.3962 0.1024 0.4986 0.2208 0.4593 0.6801 0.3086 0.0983 0.406 9 Public Private Total 0.5753 0.0277 0.6029 CHAPTER 22: USE OF MEDICINES FOR OBSTRUCTIVE AIRWAY DISEASES Malaysian Statistics on Medicines 2006 ATC Drug Class and Agents 2006 R03B A02 Budesonide Public Private Total 1.5432 0.1962 1.7393 R03B A05 Fluticasone R03B A08 Ciclesonide Public Private Total Public Private Total 0.0189 <0.0001 0.019 <0.0001 0.027 0.0271 R03B B Anticholinergics R03B B01 Ipratropium bromide R03B B04 Tiotropium bromide Public Private Total Public Private Total 0.4182 0.0527 0.4709 0.0165 0.0195 0.036 Public Private Total - Public Private Total 0.0445 0.0051 0.0496 Public Private Total Public Private Total Public Private Total Public Private Total Public Private Total 0.6566 1.8439 2.5005 0.1697 2.8792 3.049 0.0016 0.0016 0.0064 0.0064 0.003 0.003 Public Private Total Public Private Total 1.1004 0.4886 1.589 0.0028 0.0014 0.0042 Public Private Total 0.0372 0.1064 0.1436 R03B C Antiallergic agents, excl. corticosteroids R03B C01 Cromoglicic acid R03C A Alpha-and beta-adrenoreceptor agonists R03C A02 Ephedrine R03C C Selective beta-2-adrenoreceptor agonists R03C C02 Salbutamol R03C C03 Terbutaline R03C C04 Fenoterol R03C C08 Procaterol R03C C12 Bambuterol R03D A Xanthines R03D A04 Theophylline R03D A05 Aminophylline R03D C Leukotriene receptor antagonists R03D C03 Montelukast 113 Malaysian Statistics on Medicines 2006 CHAPTER 22: USE OF MEDICINES FOR OBSTRUCTIVE AIRWAY DISEASES References: 1. Global Strategy for Diagnosis, Management and Prevention of Chronic Obstructive Pulmonary Disease (Updated 2008). 114 CHAPTER 23: USE OF ANTIHISTAMINES AND NASAL DECONGESANTS Malaysian Statistics on Medicines 2006 Edited by: Saraiza AB1, Anura M2, Noormah MD3 1. Serdang Hospital, 2. University Malaya Medical Centre, 3. Medical Development Division, MOH Nasal decongestants and antihistamines are commonly used drugs for allergy and nasal symptoms in Otorhinolaryngology clinics in Malaysia. The 2006 survey showed usage of 0.9592DDD/population/year and the usage of anti-histamines for systemic use was 4.4422 DDDs/population/year. In the present survey, the drugs were classified into several types which include nasal decongestants for topical use and systemic use. For local applications it was divided into plain sympathomimetics, anti-allergic without corticosteroid and corticosteroids. The nasal decongestant for systemic use was mainly sympatomimetics. The most utilised nasal decongestants were corticosteroid based nasal decongestants. Its usage was very high compared to other topical decongestants. Newer generation corticosteroids usage was much higher in the private sector. Generic corticosteroids such as beclomethasone and budesonide had lost popularity in the private sector but not the public sector. Some plain topical decongestants especially oxymetazoline were persistently used in both private and public healthcare sectors. Pseudoephedrine combinations were widely used systemic nasal decongestants in both sectors. Antihistamines can be divided into several subgroups that is sedative and non sedative. Non sedative antihistamines are gaining popularity especially the newer generation groups. There was broad use of sedative antihistamines in the private sector but less in numbers compared to public sector. Some drugs listed were not available for use in the public sector. Usage of second and third generation antihistamines especially cetirizine, loratadine and desloratadine were frequent in public and private sectors but the usage in private was much higher. This factor may be attributed to the availability and the prescription that does not require specialist countersignature. Comparing our systemic antihistamine usage in 2006 with the Australian statistics on medicines, we found that the Australians had lower usage of antihistamines. Usage of topical nasal decongestants was comparatively lower in Malaysia then Australia. Usage of steroid based decongestant especially mometasone was high in Australia. Use of other drugs was fairly the same in both countries. Table 23.1: Use of Anti-Histamines and Nasal Decongestants, in DDD/1000 population /day 2006 and DDD/ population/year ATC Drug Class and Agents 2006 2006 (DDDs/population/year R01 R06 NASAL PREPARATIONS ANTIHISTAMINES FOR SYSTEMIC USE 2.6279 12.1703 0.9592 4.4422 Table 23.2.1: Use of Nasal Decongestants by Drug Class, in DDD/1000 population/day 2006 ATC Drug Class and Agents 2006 2006 (DDDs/population/year) R01A DECONGES TANTS AND OTHER NASAL PREPARATIONS FOR TOPICAL USE Sympathomimetics, plain Antiallergic agents, excl. corticosteroids Corticosteroids NASAL DECONGESTANTS FOR SYSTEMIC USE Sympathomimetics 1.2602 0.46 0.2781 <0.0001 0.982 1.3677 0.1015 <0.0001 0.3584 0.4992 1.3677 0.4992 R01A A R01A C R01A D R01B R01B A 115 CHAPTER 23: USE OF ANTIHISTAMINES AND NASAL DECONGESANTS Malaysian Statistics on Medicines 2006 Table 23.2.2: Use of Nasal Decongestants by Drug Class and Agents, in DDD/1000 population/day 2006 2006 ATC Drug Class and Agents 2006 (DDDs/population/year) R01A A Sympathomimetics, plain R01A A03 Ephedrine R01A A05 Oxymetazoline R01A A07 Xylometazoline Public Private Total Public Private Total Public Private Total 0.0007 0.0002 0.0008 0.0516 0.2145 0.2661 0.0112 0.0112 0.0003 <0.0001 0.0003 0.0188 0.0783 0.0971 0.0041 0.0041 Public Private Total <0.0001 <0.0001 <0.0001 <0.0001 Public Private Total Public Private Total Public Private Total Public Private Total Public Private Total 0.0637 0.0113 0.075 0.406 0.0923 0.4983 0.0003 0.1214 0.1217 0.1204 0.1337 0.2542 <0.0001 0.0328 0.0329 0.0233 0.0041 0.027 4 0.1482 0.0337 0.1819 0.0001 0.0443 0.0444 0.044 0.0488 0.0928 <0.0001 0.012 0.012 Public Private Total Public Private Total 0.0147 0.0147 0.4097 0.9432 1.353 0.0054 0.0054 0.1496 0.3443 0.4938 R01A C Antiallergic agents, excl. corticosteroids R01A C01 Cromoglicic acid R01A D Corticosteroids R01A D01 Beclometasone R01A D05 Budesonide R01A D08 Fluticasone R01A D09 Mometasone R01A D11 Triamcinolone R01B A Sympathomimetics R01B A02 Pseudoephedrine R01B A52 Pseudoephedrine, combinations Table 23.3.1: Use of Anti-Histamines by Drug Class, in DDD/1000 population/day 2006 ATC Drug Class and Agents 2006 2006 (DDDs/population/year) R06A R06A A R06A B R06A D R06A E R06A X ANTIHISTAMINES FOR SYSTEMIC USE Aminoalkyl ethers Substituted alkylamines Phenothiazine derivatives Piperazine derivatives Other antihistamines for systemic use 12.1704 0.7964 5.3686 1.2842 1.858 2.8631 116 4.4422 0.2907 1.9596 0.4687 0.6782 1.045 CHAPTER 23: USE OF ANTIHISTAMINES AND NASAL DECONGESANTS Malaysian Statistics on Medicines 2006 Table 23.3.2: Use of Anti-Histamines by Drug Class and Agents, in DDD/1000 population/day 2006 ATC Drug Class and Agents 2006 2006 (DDDs/population/year) R06A A Aminoalkyl ethers R06A A02 Diphenhydramine R06A A04 Clemastine R06A A08 Carbinoxamine R06A B Substituted alkylamines R06A B01 Brompheniramine R06A B02 Dexchlorpheniramine R06A B04 Chlorphenamine Public Private Total Public Private Total Public Private Total 0.6028 0.1772 0.78 0.0086 0.0086 0.0078 0.0078 0.22 0.0647 0.2847 0.0032 0.0032 0.0028 0.0028 Public Private Total Public Private Total Public Private Total 0.0114 0.0114 0.0486 1.3559 1.4045 2.5619 1.3908 3.9527 0.0042 0.0042 0.0177 0.4949 0.5126 0.9351 0.5076 1.4427 Public Private Total Public Private Total 0.8492 0.4305 1.2797 0.0045 0.0045 0.31 0.1571 0.4671 0.0017 0.0017 Public Private Total Public Private Total Public Private Total Public Private Total 0.0004 0.0306 0.031 0.0002 0.0041 0.0044 0.2259 1.5065 1.7324 0.0005 0.0897 0.0903 0.0001 0.0112 0.0113 <0.0001 0.0015 0.0016 0.0824 0.5499 0.6323 0.0002 0.0328 0.0329 0.0904 0.0173 0.1077 0.0014 0.0014 0.033 0.0063 0.0393 0.0005 0.0005 R06A D Phenothiazine derivatives R06A D02 Promethazine R06A D07 Mequitazine R06A E Piperazine derivatives R06A E01 Buclizine R06A E05 Meclozine R06A E07 Cetirizine R06A E09 Levocetir izine R06A X Other antihistamines for systemic use R06A X07 Triprolidine R06A X09 Azatadine Public Private Total Public Private Total 117 CHAPTER 23: USE OF ANTIHISTAMINES AND NASAL DECONGESANTS Malaysian Statistics on Medicines 2006 ATC Drug Class and Agents R06A X12 Terfenadine R06A X13 Loratadine R06A X17 Ketotifen R06A X18 Acrivastine R06A X26 Fexofenadine R06A X27 Desloratadine 2006 Public Private Total Public Private Total Public Private Total Public Private Total Public Private Total Public Private Total 0.0014 0.0014 0.7417 1.436 2.1777 0.2121 0.2121 0.0019 0.0019 0.008 0.1455 0.1535 0.0463 0.1611 0.2074 2006 (DDDs/population/year) 0.0005 0.0005 0.2707 0.5241 0.7949 0.0774 0.0774 0.0007 0.0007 0.0029 0.0531 0.056 0.0169 0.0588 0.0757 References: 1. Vernacchio L, Kelly JP, Kaufman DW, Mitchell AA, Pseudoephedrine use among US children, 1999-2006: results from the Slone survey. Pediatrics. 2008 Dec; 122(6):1299-304. 2. Ryan T, Brewer M, Small L, Over-the-counter cough and cold medication use in young children. Pediatric Nur 2008 Mar-Apr; 34(2):174-80, 184. 3. Coleman C, Moore M. Decongestants and antihistamines for acute otitis media in children. Cochrane Database Syst Rev. 2008 Jul 16; (3):CD001727. 118 CHAPTER 24 USE OF OPHTHALMOLOGICALS Malaysian Statistics on Medicines 2006 Edited by: Bethel L1, Goh PP2, Thiageswari U3, Thayanitu S4, Gong VHM5, Fadilah O2, Choong CL2 1. Tunku Jaafar Hospital, Seremban, 2. Selayang Hospital, 3. Kuala Lumpur Hospital, 4. TAR Hospital, Klang, 5. Raja Permaisuri Bainun Hospital, Ipoh The National Medicine Use Survey 2006 had results on common ophthalmological agents used in Malaysia. These include anti-infectives for the treatment of ocular infections, steroidals and steroidal and anti-infective combinations for inflammatory eye conditions and eyes following surgery, i ntraocular pressure (IOP) reducing agents for glaucoma, anticholinergic or sympathomimetic mydriatics, sympathomimetics for decongestion, antiallergics for allergic conjunctivitis, topical anaesthesia used as adjunct or as single anaesthesia during ocular surgery and antineovascularisation agents in the treatment of various retinal vascular conditions such as proliferative diabetic retinopathy and age related macular degeneration. The survey participants were mainly public health care providers (MOH and University), private hospitals and private general practitioners. It did not include individual private practice ophthalmologists. Drug utilisation statistics are generally expressed as defined daily dose (DDD), the assumed average dose per day of a drug used for its main indication by adults, as the standard unit for reference. However, except for anti-glaucoma agents, no DDD have been assigned yet by the WHO for the ophthalmologicals. Thus, for the purpose of this report on Malaysian statistics on drug utilisation, the total usage in this chapter for drugs, other than anti-glaucoma agents, is expressed in gram or ml or cc, per 1000 population (pop) per day, irrespective of the strength of the preparations. The commonest topical antibiotic used in both public and private sector for 2006 was chloramphenicol (1.12DDD/1000 population/day), followed by gentamicin (0.089), fusidic acid (0.032) and ciprofloxacin (0.019). Chloramphenicol was the commonest prescribed topical antiinfective because it is readily available, can be prescribed by all categories of medical practitioners and primary care doctors, and is affordable. Being broad spectrum, it is prescribed for the treatment of conjunctivitis, the most common eye condition presenting to primary care centres. 1,2 Among anti-inflammatory steroidal eye drops, betamethasone (0.023DDD/1000 population/day) and dexamethasone (0.022) were commonly used. Prednisolone and fluromethalone were sparingly used in the public sector as it is not freely available. Among anti-inflammatory non-steroidal eye drops, ketorolac, was more commonly used (0.0068DDD) as compared to diclofenac and indometacin. Among steroidal and anti-infective combination, dexamethasone and anti-infective combination was the commonest used (0.133DDD/1000 population/day). Steroidal and anti-infective combinations were prescribed more than plain steroidal agents because of their wider indication including post-operative prophylaxis, ocular infection and ocular trauma. Glaucoma is the second leading cause of blindness worldwide. Based on population-based studies in Singapore, the age and sex specific prevalence of glaucoma in Malays was 3.4%3, and Chinese was 3.2% 4. Prevalence of glaucoma increases with age. Most patients are treated medically and often lifelong. Some of them need more than one drug to control disease progression, and above all, anti-glaucoma agents are costly. The 2006 survey have results on 11 anti-glaucoma agents. Among them, timolol was the most commonly used (0.552DDD/1000 population/day), followed by latanoprost (0.284), dorzolamide (0.105), betaxolol (0.094). The other less commonly used anti glaucoma agents were: brimonidine (0.049), pilocarpine (0.045), brinzolamide (0.041), travoprost (0.014) and bimatoprost (0.013). The 4 most commonly prescribed anti–glaucoma agents derive from 3 pharmacologic classes, namely beta blocker (timolol and betaxolol), prostaglandin analogue (latanoprost) and carbonic anhydrase inhibitors (dorzolamide). Clinical practice guidelines on management of primary open angle glaucoma recommend that topical beta blockers and prostaglandin analogues are the most cost-effective IOP lowering agents5. The findings in this survey indicated that the prescribing pattern among ophthalmologists appear to be in compliance with the recommendation. Findings from the MOH Ophthalmology Service Census in 2007 showed that MOH Ophthalmology departments spent more than 50% of their drug allocation on anti-glaucoma agents. The expenditure on anti-glaucoma drugs will continue to rise due to increasing aging population. 119 CHAPTER 24 USE OF OPHTHALMOLOGICALS Malaysian Statistics on Medicines 2006 The commonest anti-allergic agent was cromoglicic acid and commonest local anaesthetic was proxymetacaine. Among the anti-neovascularization agents, verteporfin was the commonest used in 2006. Table 24.1: Use of Ophthalmological by Drug Class and Agents, in total dosage/1000 population/day 2006 ATC Drug Class and Agents Unit 2006 S01A A Antibiotics S01A A01 Chloramphenicol g/ml/cc S01A A02 Chlortetr acycline g/ml/cc S01A A03 Neomycin g/ml/cc S01A A09 Tetracycline g/ml/cc S01A A10 Natamycin g/ml/cc S01A A11 Gentamicin g/ml/cc S01A A12 Tobramycin g/ml/cc S01A A13 Fusidic acid g/ml/cc S01A A17 Erythromycin g/ml/cc S01A A18 Polymyxin B g/ml/cc S01A A20 Antibiotics in combination with other drugs g/ml/cc S01A A30 Combinations of different antibiotics g/ml/cc S01A B04 Sulfacetamide g/ml/cc S01A D Antivirals S01A D03 Aciclovir g/ml/cc S01A D05 Interferon g/ml/cc 120 Public Private Total Public Private Total Public Private Total Public Private Total Public Private Total Public Private Total Public Private Total Public Private Total Public Private Total Public Private Total Public Private Total Public Private Total Public Private Total 0.8457 0.2754 1.1211 0.0005 0.0012 0.0017 0.0002 0.0002 0.0009 0.0009 0.0005 0.0002 0.0007 0.0168 0.0725 0.0893 0.0001 0.005 0.0051 0.0087 0.023 1 0.0318 0.001 0.001 <0.0001 <0.0001 0.001 0.001 0.0012 0.0211 0.0222 0.003 0.003 Public Private Total Public Private Total 0.002 0.0009 0.0029 <0.0001 <0.0001 CHAPTER 24 USE OF OPHTHALMOLOGICALS Malaysian Statistics on Medicines 2006 ATC S01A X Drug Class and Agents Other antiinfectives Unit S01A X11 Ofloxacin g/ml/cc S01A X12 Norfloxacin g/ml /cc S01A X13 Ciprofloxacin g/ml/cc S01A X17 Lomefloxacin g/ml/cc S01A X19 Levofloxacin g/ml/cc S01A X22 Moxifloxacin g/ml/cc 2006 Public Private Total Public Private Total Public Private Total Public Private Total Public Private Total Public Private Total 0.0015 0.0002 0.0016 0.0006 0.0066 0.0071 0.0104 0.009 0.0194 0.0019 0.0019 <0.0001 0.0005 0.0005 0.0003 0.0003 Table 24.2: Use of Ophthalmological by Drug Class and Agents, in total dosage/1000 population/day 2006 ATC Drug Class and Agents Unit 2006 S01B A Corticosteroids, plain S01B A01 Dexamethasone g/ml/cc S01B A04 Prednisolone g/ml/cc S01B A06 Betamethasone g/ml/cc S01B A07 Fluorometholone g/ml/cc S01B C Antiinflammatory agents, non-steroids S01B C01 Indometacin g/ml/cc S01B C03 Diclofenac g/ml/cc S01B C05 Ketorolac g/ml/cc 121 Public Private Total Public Private Total Public Private Total Public Private Total 0.0191 0.003 0.0221 0.0006 0.0117 0.0123 0.0223 0.0011 0.0234 0.0023 0.0071 0.0094 Public Private Total Public Private Total Public Private Total 0.0004 0.0004 0.0002 0.0002 0.0025 0.0043 0.0068 CHAPTER 24 USE OF OPHTHALMOLOGICALS Malaysian Statistics on Medicines 2006 Table 24.3: Use of Ophthalmological by Drug Class and Agents, in total dosage/1000 population/day 2006 ATC Drug Class and Agents Unit 2006 S01C A Corticosteroids and antiinfectives in combination S01C A01 Dexamethasone and antiinfectives g/ml/cc S01C A05 Betamethasone and antiinfectives g/ml/c c S01C A07 Fluorometholone and antiinfectives g/ml/cc S01C B04 Betamethasone g/ml/cc S01C C01 Diclofenac and anti infectives g/ml/cc Public Private Total Public Private Total Public Private Total Public Private Total Public Private Total 0.0292 0.1038 0.133 0.0083 0.0062 0.0145 0.0011 0.0011 0.0006 0.0006 0.0084 0.0084 Table 24.4.1: Use of Ophthalmological by Drug Class and Agents, in DDD/1000 population/day 2006 ATC S01E A Drug Class and Agents Sympathomimetics in glaucoma therapy S01E A05 Brimonidine S01E B Parasympathomimetics S01E B01 Pilocarpine S01E B02 Carbachol S01E C Carbonic anhydrase inhibitors S01E C01 Acetazolamide S01E C03 Dorzolamide S01E C04 Brinzolamide S01E D Beta blocking agents S01E D01 Timolol S01E D02 Betaxolol 122 2006 Public Private Total 0.0309 0.0181 0.0489 Public Private Total Public Private Total 0.0374 0.0075 0.0449 0.0039 0.0011 0.005 Public Private Total Public Private Total Public Private Total 0.0214 0.0058 0.0273 0.1007 0.0046 0.1052 0.0356 0.0055 0.041 Public Private Total Public Private Total 0.4858 0.0665 0.5522 0.0683 0.0257 0.094 CHAPTER 24 USE OF OPHTHALMOLOGICALS ATC Drug Class and Agents S01E D03 Levobunolol S01E E Prostaglandin analogues S01E E01 Latanoprost S01E E03 Bimatoprost S01E E04 Travoprost Malaysian Statistics on Medicines 2006 2006 Public Private Total 0.0012 0.0012 Public Private Total Public Private Total Public Private Total 0.2684 0.0153 0.2837 <0.0001 0.0129 0.0129 0.006 0.0075 0.0135 Table 24.4.2: Use of Ophthalmological by Drug Class and Agents, in total dosage/1000 population/day 2006 ATC S01E D Drug Class and Agents Beta blocking agents Unit S01E D51 Timolol, combinations g/ml/cc 2006 Public Private Total 0.0002 0.0016 0.0018 Table 24.5: Use of Ophthalmological by Drug Class and Agents, in total dosage/1000 population/day 2006 ATC S01F A Drug Class and Agents Anticholinergics Unit S01F A01 Atropine g/ml/cc S01F A04 Cyclopentolate g/ml/cc S01F A05 Homatropine g/ml/cc S01F A06 Tropicamide g/ml/cc S01F B Sympathomimetics excl. antiglaucoma preparations S01F B0 1 Phenylephrine g/ml/cc 123 2006 Public Private Total Public Private Total Public Private Total Public Private Total 0.0063 0.001 0.0073 0.0042 0.0024 0.0066 0.0108 0.0027 0.0136 0.0202 0.0057 0.026 Public Private Total 0.009 0.0026 0.0116 CHAPTER 24 USE OF OPHTHALMOLOGICALS Malaysian Statistics on Medicines 2006 Table 24.6: Use of Ophthalmological by Drug Class and Agents, in total dosage/1000 population/day 2006 ATC Drug Class and Agents Unit 2006 S01G A Sympathomimetics used as decongestants S01G A01 Naphazoline g/ml/cc S01G A02 Tetryzoline g/ml/cc S01G A51 Naphazoline, combinations g/ml/cc S01G A52 Tetryzoline, combinations g/ml/cc S01G A55 Phenylephrine, combinations g/ml/cc S01G X Other antiallergics S01G X01 Cromoglicic acid g/ml/cc S01G X05 Lodoxamide g/ml/cc S01G X06 Emedastine g/ml/cc S01G X09 Olopatadine g/m l/cc Public Private Total Public Private Total Public Private Total Public Private Total Public Private Total 0.0073 0.0073 0.0228 0.0228 0.0072 0.0072 0.0082 0.0165 0.0247 0.0004 0.0018 0.0021 Public Private Total Public Private Total Public Private Total Public Private Total 0.0308 0.0284 0.0592 0.0029 0.0029 0.0026 0.0026 0.0007 0.006 0.0068 Table 24.7: Use of Ophthalmological by Drug Class and Agents, in total dosage/1000 population/day 2006 ATC S01H A Drug Class and Agents Local anaesthetics Unit S01H A02 Oxybuprocaine g/ml/cc S01H A03 Tetracaine g/ml/cc S01H A04 Proxymetacaine g/ml/cc 124 2006 Public Private Total Public Private Total Public Private Total 0.0003 0.0002 0.0006 0.0006 0.0001 0.0007 0.0167 0.006 0.0227 CHAPTER 24 USE OF OPHTHALMOLOGICALS Malaysian Statistics on Medicines 2006 Table 24.8: Use of Ophthalmological by Drug Class and Agents, in total dosage/1000 population/day 2006 ATC Drug Class and Agents Unit 2006 S01L A Antineovascularisation agents S01L A01 Verteporfin mg S01L A03 Pegaptanib g/ml/cc S01L A04 Ranibizumab g/ml/cc Public Private Total Public Private Total Public Private Total 0.0003 0.0003 <0.0001 <0.0001 <0.0001 <0.0001 <0.0001 Table 24.9: Use of Ophthalmological by Drug Class and Agents, in total dosage/100 population/day 2006 ATC Drug Class and Agents Unit 2006 S01X A Other ophthalmologicals S01X A13 Alteplase g/ml/cc Public Private Total <0.0001 <0.0001 Table 24.10: Use of Ophthalmological by Drug Class and Agents, in total dosage/1000 population/day 2006 ATC S03A A Drug Class and Agents Antiin fectives Unit S03A A06 Gentamicin g/ml/cc S03A A08 Chloramphenicol g/ml/cc 2006 Public Private Total Public Private Total 0.0022 0.0136 0.0158 0.0005 0.0005 Table 24.11: Use of Ophthalmological by Drug Class and Agents, in total dosage/1000 population/day 2006 ATC S03B A Drug Class and Agents Corticosteroids Unit S03B A03 Betamethasone g/ml/cc 2006 Public Private Total 0.0022 0.0012 0.0033 Table 24.12: Use of Ophthalmological by Drug Class and Agents, in total dosage/1000 population/day 2006 ATC S03C A Drug Class and Agents Unit Corticosteroids and antiinfectives in combination S03C A01 Dexamethasone and antiinfectives g/ml/cc S03C A06 Betamethasone and antiinfectives g/ml/cc 125 2006 Public Private Total Public Private Total <0.0001 0.1409 0.141 0.0028 0.0096 0.0124 CHAPTER 24 USE OF OPHTHALMOLOGICALS Malaysian Statistics on Medicines 2006 References: 1. Dart, JK. Eye disease at a community health centre. Br Med J (Clin Res Ed) 1986; 293:1477. 2. Leibowitz, HM. The red eye. N Engl J Med 2000; 343:345. 3. Sunny Y Shen, Tien Y Wong, Paul J Foster, et al. The Prevalence and Types of Glaucoma in Malay People: The Singapore Malay Eye Study. IOVS 2008 (in print). 4. Poster PJ, Oen FT, Machin D, et al. The prevalence of glaucoma in Chinese residents of Singapore: a cro sectional population survey of the Tanjong Pagar district. Arch Ophthalmol 2000; 118:1105-11. 5. Clinical Practice Guidelines on Management of Primary Open Angle Glaucoma. MOH Publication. MOH/P PAK/159.O8 (GU) Feb 2008. 126 CHAPTER 25 USE OF OTOLOGICALS Malaysian Statistics on Medicines 2006 Edited by: Saraiza AB1, Anura M2, Noormah MD3 1. Serdang Hospital, 2. University Malaya Medical Centre, 3. Medical Development Division MOH Drug utilisation statistics are generally expressed as defined daily dose (DDD), the assumed average dose per day of a drug used for its main indication by adults, as the standard unit for reference. However, no DDD have been assigned yet by the WHO for the otologicals. Thus, for the purpose of this chapter report, the total usage for otological drugs is expressed in gram or ml or cc, per 1000 population (pop) per day, irrespective of the strength of the preparations. Otological preparations used in Malaysia are classified into local antibiotic ear drops, local steroid ear drops and combination antibiotic and steroid ear drops. The 2006 national survey showed that the private sector used a wider variety of otological drugs compared to the public sector. The use of combination antibiotic and steroid ear drops were much higher in the private sector, 3.5 times more than the amount used in public hospitals; while antibiotic preparations alone were more commonly used in public hospitals, 2.7 times more than the private sector. Steroid alone preparations were used only in the public hospitals. The total usage of otological preparations were 0.2725g/ml per 1000 population per day. Table 25: Use of Otologicals by Drug Class and Agents, in total dosage/1000 population/day 2006 ATC S02A A Drug Class and Agents Antiinfectives Unit S02A A01 Chloramphenicol g/ml/cc S02A A07 Neomycin g/ml /cc S02A A11 Polymyxin B g/ml/cc S02A A14 Gentamicin g/ml/cc 2006 Public Private Total Public Private Total Public Private Total Public Private Total 0.1605 0.0507 0.2112 0.0007 0.0007 0.0067 0.0067 0.0014 0.0014 Table 25.2: Use of Otologicals by Drug Class and Agents, in total dosage/1000 population/day 2006 ATC S02B A Drug Class and Agents Corticosteroids Unit S02B A07 Betamethasone g/ml/cc 127 2006 Public Private Total 0.0017 0.0017 CHAPTER 25 USE OF OTOLOGICALS Malaysian Statistics on Medicines 2006 Table 25.3: Use of Otologicals by Drug Class and Agents, in total dosage/1000 population/day 2006 ATC S02C A Drug Class and Agents Unit Corticosteroids and antiinfectives incombination S02 C A03 Hydrocortisone and antiinfectives g/ml/cc S02C A04 Triamcinolone and antiinfectives g/ml/cc S02C A06 Dexameth asone and antiinfectives g/ml/cc 2006 Public Private Total Public Private Total Public Private Total 0.0013 0.0091 0.0104 0.0083 0.0055 0.0138 0.0259 0.0007 0.0266 References: 1. Poetker DM, Lindstrom DR, Patel NJ, Conley SF, Flanary VA, Link TR, Kerschner JE, Ofloxacin otic drops vs neomycin-polymyxin B otic drops as prophylaxis against early postoperative tympanostomy tube otorrhea: Arch Otolaryngol Head Neck Surg. 2006 Dec; 132(12):1294-8. 2. Coleman C, Moore M. Decongestants and antihistamines for acute otitis media in children. Cochrane Database Syst Rev. 2008 Jul, 16; (3):CD001727. 128 APPENDIX 1 Malaysian Statistics on Medicines 2006 PARTICIPANTS OF THE NATIONAL MEDICINES USE SURVEY Hospitals participating in NMUS survey # Ministry of Health Hospitals 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. 14. 15. 16. 17. 18. 19. 20. 21. 22. 23. 24. 25. 26. 27. 28. 29. 30. 31. 32. 33. 34. 35. 36. 37. 38. 39. 40. 41. 42. 43. 44. 45. 46. 47. Hospital Alor Gajah Hospital Ampang Hospital Bahagia Ulu Kinta Hospital Balik Pulau Hospital Baling Hospital Banting Hospital Batu Gajah Hospital Batu Pahat Hospital Bau Hospital Beaufort Hospital Beluran Hospital Bentong Hospital Besut Hospital Betong Hospital Bintulu Hospital Bukit Mertajam Hospital Changkat Melintang Hospital Daerah Lawas Hospital Daro Hospital Duchess of Kent, Sandakan Hospital Dungun Hospital Gerik Hospital Gua Musang Hospital Hulu Terengganu Hospital Jasin Hospital Jelebu Hospital Jeli Hospital Jempol Hospital Jengka Hospital Jerantut Hospital Jitra Hospital Kajang Hospital Kampar Hospital Kanowit Hospital Kapit Hospital Kemaman Hospital Keningau Hospital Kepala Batas Hospital Kinabatangan Hospital Kluang Hospital Kota Belud Hospital Kota Marudu Hospital Kota Tinggi Hospital Kuala Kangsar Hospital Kuala Krai Hospital Kuala Kubu Bharu Hospital Kuala Lipis 48. 49. 50. 51. 52. 53. 54. 55. 56. 57. 58. 59. 60. 61. 62. 63. 64. 65. 66. 67. 68. 69. 70. 71. 72. 73. 74. 75. 76. 77. 78. 79. 80. 81. 82. 83. 84. 85. 86. 87. 88. 89. 90. 91. 92. 93. 94. Hospital Kuala Lumpur Hospital Kuala Nerang Hospital Kuala Penyu Hospital Kudat Hospital Kulim Hospital Kunak Hospital Labuan Hospital Lahad Datu Hospital Langkawi Hospital Likas Hospital Limbang Hospital Lundu Hospital Machang Hospital Marudi Hospital Melaka Hospital Mersing Hospital Mesra Bukit Padang Hospital Miri Hospital Muadzam Shah Hospital Mukah Hospital Pakar Sultanah Fatimah, Muar Hospital Papar Hospital Parit Buntar Hospital Pasir Mas Hospital Pekan Hospital Permai Hospital Pitas Hospital Pontian Hospital Port Dickson Hospital Pulau Pinang Hospital Putrajaya Hospital Queen Elizabeth Hospital Raja Perempuan Bainun, Ipoh Hospital Raja Perempuan Zainab II, Kota Bharu Hospital Rajah Charles Brooke Memorial Hospital Ranau Hospital Raub Hospital Sarikei Hospital Seberang Jaya Hospital Segamat Hospital Selama Hospital Selayang Hospital Semporna Hospital Sentosa Hospital Serdang Hospital Seri Manjung Hospital Serian APPENDIX 1 Malaysian Statistics on Medicines 2006 PARTICIPANTS OF THE NATIONAL MEDICINES USE SURVEY Hospitals participating in NMUS survey # Ministry of Health Hospitals 95. 96. 97. 98. 99. 100. 101. 102. 103. 104. 105. 106. 107. 108. 109. 110. 111. 112. 113. # 1. 2. # Hospital Setiu Hospital Sibu Hospital Sik Hospital Simunjan Hospital Sipitang Hospital Slim River Hospital Sri Aman Hospital Sultan Abdul Halim, Sungai Petani Hospital Sultan Haji Ahmad Shah, Temerloh Hospital Sultan Ismail, Johor Bahru Hospital Sultanah Aminah, Johor Bahru Hospital Sultanah Bahiyah, Alor Setar Hospital Sultanah Nur Zahirah, Kuala Terengganu Hospital Sungai Bakap Hospital Sungai Buloh Hospital Sungai Siput Hospital Taiping Hospital Tambunan Hospital Tampin Universiti Kebangsaan Malaysia Medical Centre University Malaya Medical Centre Armed Forces Hospitals Lumut Armed Forces Hospital Terendak Armed Forces Hospital # Private Hospitals 1. 2. 3. 4. Amanjaya Specialist Centre Ampang Puteri Specialist Hospital Bukit Mertajam Specialist Hospital Columbia Asia Medical Centre, Sarawak Columbia Asia Medical Centre, Seremban Columbia Asia Nursing and Rehabilitation Centre Damai Service Hospital, Melawati Damansara Specialist Hospital Darul Ehsan Medical Centre 6. 7. 121. 122. 123. 124. 125. 126. 127. 128. 129. 130. 131. 132. Hospital Tanah Merah Hospital Tangkak Hospital Tanjong Karang Hospital Tapah Hospital Tawau Hospital Teluk Intan Hospital Temenggung Seri Maharaja Tun Ibrahim, Kulai Hospital Tengku Ampuan Afzan, Kuantan Hospital Tengku Ampuan Jemaah, Sabak Bernam Hospital Tengku Ampuan Rahimah, Klang Hospital Tengku Anis, Pasir Puteh Hospital Tenom Hospital Tuanku Ampuan Najihah, Kuala Pilah Hospital Tuanku Fauziah, Kangar Hospital Tuanku Ja’afar, Seremban Hospital Tumpat Hospital Umum Sarawak Hospital Yan Hospital Saratok University Hospitals 1. 2. 5. 114. 115. 116. 117. 118. 119. 120. 8. 9. 10. 11. 12. 13. 14. 15. 16. 17. Gleneagles Intan Medical Centre Ipoh Specialist Hospital Island Hospital Johor Specialist Hospital Kajang Specialist Hospital Kampung Baru Medical Centre Kempas Medical Centre Kuantan Medical Centre Kuantan Specialist Hospital Landmark Medical Centre Sdn. Bhd. APPENDIX 1 Malaysian Statistics on Medicines 2006 PARTICIPANTS OF THE NATIONAL MEDICINES USE SURVEY Hospitals participating in NMUS survey # Ministry of Health Hospitals 18. 19. 20. 21. 22. 23 23. 24. 25. 26. 27. 28. 29. 30. 31. 32 Loh Guan Lye Specialist Centre Medical Specialist Centre (JB) Sdn. Bhd. Metro Specialist Hospital Miri City Medical Centre N.S. Chinese Maternity Hospital and Medical Centre National Heart Institute NCI Cancer Hospital Pantai Ayer Keroh Hospital Sdn. Bhd. Pantai Cheras Medical Centre Pantai Indah Hospital Pantai Klang Specialist Medical Centre Sdn. Bhd. Pantai Mutiara Hospital Pantai Putri Hospital Pantai Utara Hospital Penang Adventist Hospital Perdana Specialist Hospital 33. 34. 35. 36. 37. 38. 39. 40. 41. 42. 43. 44. 45. 46. 47. 48. 49. PUSRAWI Hospital Sdn. Bhd. Puteri Klang Medical Centre Puteri Specialist Hospital Putra Medical Centre, Alor Setar Putra Specialist Hospital (Batu Pahat) Sdn. Bhd. Putra Specialist Hospital (Melaka) Sdn. Bhd. Rafflesia Medical Centre Sdn. Bhd. Sabah Medical Centre Selangor Medical Centre Sentosa Medical Centre Sdn. Bhd. KL Sri Kota Specialist Medical Centre Subang Jaya Medical Centre Sunway Medical Centre Taman Desa Medical Centre Tanjung Medical Centre Timberland Medical Centre Tung Shin Hospital Hospitals participating in NMUS survey # State/ District/Area Health Departments 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. 14. 15. 16. 17. 18. 19. 20. 21. 22. Jabatan Kesihatan Negeri Johor Jabatan Kesihatan Negeri Kelantan Jabatan Kesihatan Negeri Perlis Jabatan Kesihatan Negeri Sabah Jabatan Kesihatan Negeri Sarawak Pejabat Kesihatan Daerah Alor Gajah Pejabat Kesihatan Daerah Bachok Pejabat Kesihatan Daerah Batu Pahat Pejabat Kesihatan Daerah Baling Pejabat Kesihatan Daerah Barat Daya Pejabat Kesihatan Daerah Batang Padang Pejabat Kesihatan Daerah Bandar Baharu Pejabat Kesihatan Daerah Besut Pejabat Kesihatan Daerah Cameron Highlands Pejabat Kesihatan Daerah Dungun Pejabat Kesihatan Daerah Gombak Pejabat Kesihatan Daerah Gua Musang Pejabat Kesihatan Daerah Hilir Perak Pejabat Kesihatan Daerah Hulu Langat Pejabat Kesihatan Daerah Hulu Perak Pejabat Kesihatan Daerah Hulu Selangor Pejabat Kesihatan Daerah Hulu Terengganu 23. 24. 25. 26. 27. 28. 29. 30. 31. 32. 33. 34. 35. 36. 37. 38. 39. 40. 41. 42. 43. 44. 165 Pejabat Kesihatan Daerah Kulim Pejabat Kesihatan Daerah Langkawi Pejabat Kesihatan Daerah Larut, Matang dan Selama Pejabat Kesihatan Daerah Manjung Pejabat Kesihatan Daerah Maran Pejabat Kesihatan Daerah Marang Pejabat Kesihatan Daerah Melaka Tengah Pejabat Kesihatan Daerah Muar Pejabat Kesihatan Daerah Padang Terap Pejabat Kesihatan Daerah Pasir Mas Pejabat Kesihatan Daerah Pasir Puteh Pejabat Kesihatan Daerah Penampang Pejabat Kesihatan Daerah Pendang Pejabat Kesihatan Daerah Perak Tengah Pejabat Kesihatan Daerah Petaling Pejabat Kesihatan Daerah Pitas Pejabat Kesihatan Daerah Port Dickson Pejabat Kesihatan Daerah Putrajaya Pejabat Kesihatan Daerah Sabak Bernam Pejabat Kesihatan Daerah Segamat Pejabat Kesihatan Daerah Seremban Pejabat Kesihatan Daerah Seberang Perai Selatan APPENDIX 1 Malaysian Statistics on Medicines 2006 PARTICIPANTS OF THE NATIONAL MEDICINES USE SURVEY Hospitals participating in NMUS survey # State/ District/Area Health Departments 45. 46. 47. 48. 49. 50. 51. 52. 53. 54. 55. 56. 57. 58. 59. 60. 61. 62. 63. 64. 65. 66. 67. 68. 69. 70. 71. 72. 73. 74. 75. 76. 77. 78. 79. 80. 81. 82. 83. 84. 85. 86. 87. 88. 89. 90. 91. 92. 93. 94. 95. 96. Pejabat Kesihatan Daerah Jasin Pejabat Kesihatan Daerah Jelebu Pejabat Kesihatan Daerah Jeli Pejabat Kesihatan Daerah Jempol Pejabat Kesihatan Daerah Johor Bahru Pejabat Kesihatan Daerah Kemaman Pejabat Kesihatan Daerah Keningau Pejabat Kesihatan Daerah Kerian Pejabat Kesihatan Daerah Kinta Pejabat Kesihatan Daerah Klang Pejabat Kesihatan Daerah Kluang Pejabat Kesihatan Daerah Kota Bharu Pejabat Kesihatan Daerah Kota Setar Pejabat Kesihatan Daerah Kuala Kangsar Pejabat Kesihatan Daerah Kuala Krai Pejabat Kesihatan Daerah Kuala Langat Pejabat Kesihatan Daerah Kuala Muda Pejabat Kesihatan Daerah Kuala Penyu Pejabat Kesihatan Daerah Kuala Pilah Pejabat Kesihatan Daerah Kuala Selangor Pejabat Kesihatan Daerah Kuala Terengganu Pejabat Kesihatan Daerah Kuantan Pejabat Kesihatan Daerah Kubang Pasu Pejabat Kesihatan Daerah Kudat Pejabat Kesihatan Daerah Seberang Perai Tengah Pejabat Kesihatan Daerah Seberang Perai Utara # Others 1. 2. Department of Public Health, MOH Disease Control Division, National Public Health Laboratory Vector Borne Disease Control Section, Disease Control Division, MOH 3. 4. 5. 6. 7. 8. 166 Pejabat Kesihatan Daerah Sepang Pejabat Kesihatan Daerah Setiu Pejabat Kesihatan Daerah Sik Pejabat Kesihatan Daerah Tampin Pejabat Kesihatan Daerah Tanah Merah Pejabat Kesihatan Daerah Timur Laut Pejabat Kesihatan Daerah Tumpat Pejabat Kesihatan Daerah Yan Pejabat Kesihatan Kawasan Beaufort Pejabat Kesihatan Kawasan Beluran Pejabat Kesihatan Kawasan Kota Kinabalu Pejabat Kesihatan Kawasan Lahad Datu Pejabat Kesihatan Kawasan Sandakan Pejabat Kesihatan Kawasan Tawau Pejabat Kesihatan Kawasan Tuaran Pejabat Pergigian Bahagian Kuching Pejabat Pergigian Bahagian Miri Pejabat Pergigian Bahagian Samarahan Pejabat Pergigian Bahagian Sibu Pejabat Pergigian Bahagian Sri Aman Pejabat Pergigian Beaufort Pejabat Pergigian Daerah Petaling Pejabat Pergigian Daerah Kemaman Pejabat Pergigian Daerah Seberang Perai Utara Pejabat Pergigian Sandakan Pejabat Pergigian Tawau Ibu Pejabat Tibi/Kusta – Kota Kinabalu National Leprosy Control Centre Pegawai Kesihatan Kanan (RKPBV) Perak Pegawai Pergigian Kanan Pahang Pegawai Pergigian Kanan Perak APPENDIX 1 Malaysian Statistics on Medicines 2006 PARTICIPANTS OF THE NATIONAL MEDICINES USE SURVEY Ministry of Health Institutions participating in NMUS survey 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. College of Allied Health Science, Kuching College of Community Nursing, Kluang College of Medical Laboratory Technology College of Nursing, Ipoh College of Nursing, Kuala Terengganu College of Nursing, Kubang Kerian Institute for Medical Research (IMR) Institute for Public Health Kolej Kejururawatan Masyarakat Kolej Kejururawatan Melaka Makmal Keselamatan dan Kualiti Makanan, Pulau Pinang 12. 13. 14. 15. 16. 17. 18. 19. 20. 21. 22. Makmal Perubatan dan Stor Kuching Makmal Ubat & Stor Kapit Makmal Ubat & Stor Limbang Makmal Ubat & Stor Miri Makmal Ubat & Stor Sarikei Makmal Ubat & Stor Sibu Makmal Ubat & Stor Sri Aman National Blood Centre Pusat Bekalan Farmasi Negeri Sabah, Kota Kinabalu Stor Pergigian Negeri Selangor Stor Pergigian Pusat Kota Kinabalu Primary Care Clinics participating in NMUS survey # Ministry of Health Clinics 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. 14. 15. 16. 17. 18. 19. 20. 21. 22. 23. 24. 25. 26. 27. 28. 29. 30. Jabatan Pesakit Luar Hospital Baling Jabatan Pesakit Luar Hospital Bandar Machang Jabatan Pesakit Luar Hospital Balik Pulau Jabatan Pesakit Luar Hospital Bukit Mertajam Jabatan Pesakit Luar, Hospital Mersing Jabatan Pesakit Luar, Poliklinik Komuniti Sipitang Klinik Kesihatan Air Hangat Klinik Kesihatan Air Itam Pulau Pinang Klinik Kesihatan Ayer Molek Klinik Kesihatan Bahau Klinik Kesihatan Bakar Arang Klinik Kesihatan Bandar Bachok Klinik Kesihatan Bandar Baharu Klinik Kesihatan Bandar 32 Bera Klinik Kesihatan Bandar Gua Musang Klinik Kesihatan Bandar Miri Klinik Kesihatan Bandar Pasir Mas Klinik Kesihatan Bandar Sungai Petani Klinik Kesihatan Benta Klinik Kesihatan Beris Kubor Besar Klinik Kesihatan Beris Panchor Klinik Kesihatan Beseri Klinik Kesihatan Bintangor Klinik Kesihatan Bintulu Klinik Kesihatan Bongawan Klinik Kesihatan Bukit Mendi Klinik Kesihatan Bukit Minyak Klinik Kesihatan Beris Panchor Klinik Kesihatan Bukit Pasir, Muar Klinik Kesihatan Bukit Tunggal 167 31. 32. 33. 34. 35. 36. 37. 38. 39. 40. 41. 42. 43. 44. 45. 46. 47. 48. 49. 50. 51. 52. 53. 54. 55. 56. 57. 58. 59. 60. Klinik Kesihatan Cheng Klinik Kesihatan Cheroh Klinik Kesihatan Chini Klinik Kesihatan Dabong Klinik Kesihatan Durian Tunggal Klinik Kesihatan Dong Klinik Kesihatan Gambang Klinik Kesihatan Gual Ipoh Klinik Kesihatan Hutan Percha Klinik Kesihatan Ibu dan Anak Gombak Setia Klinik Kesihatan Ibu dan Anak (Pejabat Kesihatan Daerah Dungun) Klinik Kesihatan Ibu dan Anak Kuala Nerang Klinik Kesihatan Jalan Gereja Klinik Kesihatan Jalan Masjid Kuching Klinik Kesihatan Jalan Oya Klinik Kesihatan Jelapang Klinik Kesihatan Jelebu Klinik Kesihatan Jeli Klinik Kesihatan Juasseh Klinik Kesihatan Kapit Klinik Kesihatan Karak Klinik Kesihatan Kampung Gial Klinik Kesihatan Kepala Batas Klinik Kesihatan Kinarut Klinik Kesihatan Klebang Besar Klinik Kesihatan Kota Sentosa Klinik Kesihatan Kuah Klinik Kesihatan Kuala Penyu Klinik Kesihatan Kuala Perlis Klinik Kesihatan Kuala Sanglang APPENDIX 1 Malaysian Statistics on Medicines 2006 PARTICIPANTS OF THE NATIONAL MEDICINES USE SURVEY Primary Care Clinics participating in NMUS survey # Ministry of Health Clinics 61. 62. 63. 64. 65. 66. 67. 68. 69. 70. 71. 72. 73. 74. 75. 76. 77. 78. 79. 80. 81. 82. 83. 84. 85. 86. 87. 88. 89. 90. 91. 92. 93. 94 95. 96. 97. 98. 99. 100. 101. 102. 103. 104. 105. 106. 107. Klinik Kesihatan Kulim Klinik Kesihatan Labok Klinik Kesihatan Lanang Klinik Kesihatan Lawas Klinik Kesihatan Lenga, Muar Klinik Kesihatan Lubok China Klinik Kesihatan Lubuk Buntar Klinik Kesihatan Lubuk Merbau Klinik Kesihatan Lui Muda Klinik Kesihatan Macap Baru Klinik Kesihatan Mahligai Klinik Kesihatan Merlimau Klinik Kesihatan Menglembu Klinik Kesihatan Menggatal Klinik Kesihatan Mempaga (Felda PK Fasa 1) Klinik Kesihatan Merbau Pulas Klinik Kesihatan Naka Klinik Kesihatan Padang Besar Klinik Kesihatan Padang Matsirat Klinik Kesihatan Padang Tengku Klinik Kesihatan Paka Klinik Kesihatan Parit Raja Klinik Kesihatan Parit Yaani Klinik Kesihatan Pengkalan Chepa Klinik Kesihatan Perai Klinik Kesihatan Pulai Chondong Klinik Kesihatan Putatan Klinik Kesihatan Pokok Assam Klinik Kesihatan Rantau Panjang Klinik Kesihatan Rembau Klinik Kesihatan Sarikei Klinik Kesihatan Seberang Jaya Klinik Kesihatan Selangau Klinik Kesihatan Semerah Klinik Kesihatan Serting Hilir Klinik Kesihatan Siburan Klinik Kesihatan Simpang Bekoh Klinik Kesihatan Simpang Durian Klinik Kesihatan Simpang Empat Klinik Kesihatan Sri Aman Klinik Kesihatan Sri Medan Klinik Kesihatan Sungai Acheh Klinik Kesihatan Sungai Lembing Klinik Kesihatan Sungai Rambai Klinik Kesihatan Tanah Puteh Klinik Kesihatan Tanjung Kling Klinik Kesihatan Taman Selasih 108. 109. 110. 111. 112. 113. 114. 115. 116. 117. 118. 119. 120. 121. 122. 123. 124. 125. 126. 127. 128. 129. 130. 131. 132. 133. 134. 135. 136. 137. 138. 139. 140. 141. 142. 143. 144. 145. 146. 147. 148. 149. 150. 151. 152. 153. 154. 168 Klinik Kesihatan Teluk Bahang Klinik Kesihatan Temerloh Klinik Kesihatan Tersang Klinik Kesihatan Triang Klinik Kesihatan Tudan Klinik Kesihatan Ulu Gali Klinik Pergigian Banting Klinik Pergigian Bentong Klinik Pergigian Bintulu Klinik Pergigian Besar Baling Klinik Pergigian Besar Jalan Gambut, Kuantan Klinik Pergigian Besar Jitra Klinik Pergigian Besar Kulim Klinik Pergigian Besar Langkawi Klinik Pergigian Besar Sungai Petani Klinik Pergigian Besar Telok Wanjah Klinik Pergigian Daerah Kerian Klinik Pergigian Hospital Kuala Kangsar Klinik Pergigian Hospital Teluk Intan Klinik Pergigian Hulu Perak Klinik Pergigian Kelana Jaya Klinik Pergigian Keningau Klinik Pergigian Komuniti Tapah Klinik Pergigian Kinta Klinik Pergigian Kubang Semang Klinik Pergigian Kudat Klinik Pergigian Labuan Klinik Pergigian Limbang Klinik Pergigian Mukah Klinik Pergigian Pakar Hospital Lahad Datu Klinik Pergigian Pakar Kuching Klinik Kesihatan Selandar Klinik Pergigian Perak Tengah Klinik Pergigian Rompin Klinik Pergigian Seremban Klinik Pergigian Seri Manjung Klinik Pergigian Taiping Klinik Pergigian Wilayah Poliklinik Komuniti Ajil Poliklinik Komuniti Alor Janggus Poliklinik Komuniti Air Tawar 2 Poliklinik Komuniti AU 2 Poliklinik Komuniti Ayer Baloi Poliklinik Komuniti Bagan Terap Poliklinik Komuniti Bandar Permaisuri Poliklinik Komuniti Bandar Tenggara Poliklinik Komuniti Batu Rakit APPENDIX 1 Malaysian Statistics on Medicines 2006 PARTICIPANTS OF THE NATIONAL MEDICINES USE SURVEY Primary Care Clinics participating in NMUS survey # Ministry of Health Clinics 155. 156. 157. 158. 159. 160. 161. 162. 163. 164. 165. 166. 167. 168. 169. 170. 171. 172. 173. 174. 175. 176. 177. 178. 179. 180. 181. Poliklinik Komuniti Bukit Besi Poliklinik Komuniti Bukit Changgang Poliklinik Komuniti Bukit Payong Poliklinik Komuniti Bukit Waha Poliklinik Komuniti Endau Poliklinik Komuniti Jabi Poliklinik Komuniti Jalan Mengkibol Poliklinik Komuniti Jalan Merbau Poliklinik Komuniti Ijok Poliklinik Komuniti Inanam Poliklinik Komuniti Kahang Batu 22 Poliklinik Komuniti Kahang Timur Poliklinik Komuniti Kampung Lalang Poliklinik Komuniti Kampung Majidee Poliklinik Komuniti Kampung Rahmat Poliklinik Komuniti Kampung Soeharto Poliklinik Komuniti Kota Sarang Semut Poliklinik Komuniti Klang Poliklinik Komuniti Kuala Ketil Poliklinik Komuniti Kundasang Poliklinik Komuniti Kupang Poliklinik Komuniti Lok Heng Poliklinik Komuniti Malau Poliklinik Komuniti Manir Poliklinik Komuniti Membakut Poliklinik Komuniti Paloh, Kluang Poliklinik Komuniti Palong 4,5,6 182. 183. 184. 185. 186. 187. 188 189. 190. 191. 192. 193. 194. 195. 196. 197. 198. 199. 200. 201. 202. 203. 204. 205. 206. 207. 208. Poliklinik Komuniti Pasir Akar Poliklinik Komuniti Pekan Air Panas Poliklinik Komuniti Pekan Nanas Poliklinik Komuniti Penampang Poliklinik Komuniti Pengkalan Berangan Poliklinik Komuniti Pengerang Poliklinik Komuniti Pokok Sena Poliklinik Komuniti Pontian Poliklinik Komuniti Renggam Poliklinik Komuniti Salak Poliklinik Komuniti Seberang Takir Poliklinik Komuniti Sekinchan Poliklinik Komuniti Simpang Empat Poliklinik Komuniti Sri Medang/Gong Tok Pek Poliklinik Komuniti Sungai Air Tawar Poliklinik Komuniti Sungai Buloh Poliklinik Komuniti Sungai Selisek Poliklinik Komuniti Tamparuli Poliklinik Komuniti Tampoi Poliklinik Komuniti Tawar Poliklinik Komuniti Telipok Poliklinik Komuniti Tenggaroh II (Felda) Poliklinik Komuniti Tengkawang Poliklinik Komuniti Tunjang Poliklinik Komuniti Ulu Tiram Poliklinik Komuniti Wakaf Tapai Poliklinik Penambang Primary Care Clinics participating in NMUS survey # Private Clinics 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12 24 Jam Poliklinik Yap Ali Klinik Asia Clinic B. Kong’s Clinic Bina Kelinik Chan Clinic, Kuching Chen Dispensary Chan Clinic, Miri Cheah & Lim Medical Associates Chu Hwa Dispensary City Medical Centre City Poliklinik 13 14. 15 16 17 18 19. 20. 21. 22. 23. 24. 169 Clinic Ho Clinic Joseph Chong’s Clinic Clinic Wellness Lab, Cheras Dindings Poliklinik Ding Polyklinik Dan Surgeri Dispensary Martin dan Lalita Dispensary Sharil Dora Medical Clinic Bhd. Dr Amir Abbas-KMA Sdn.Bhd. Dr Jaafar Dan Rakan-Rakan Dr John Yeo’ Clinic, Batu Niah APPENDIX 1 Malaysian Statistics on Medicines 2006 PARTICIPANTS OF THE NATIONAL MEDICINES USE SURVEY Primary Care Clinics participating in NMUS survey # Private Clinics 25. 26. 27. 28. 29. 30. 31. 32. 33. 34. 35. 36. 37. 38. 39. 40. 41. 42. 43. 44. 45. 46. 47. 48. 49. 50. 51. 52. 53. 54. 55. 56. 57. 58. 59. 60. 61. 62. 63. 64. Dr. Kueh’s Clinic Dr. Leela Ratos dan Rakan-Rakan Sdn. Bhd. Jln. Pudu Dr. Mohamed Mydin & Rakan-Rakan Sdn. Bhd. Jln. Ampang Dr. Mohamed Mydin & Rakan-Rakan Sdn. Bhd. Jln. Tun Razak Dr. S. Vijayakumar Dr. Yap’s Clinic Fateh, Mydin dan Rakan-Rakan Poliklinik & Surgeri Drs. Young Newton & Partners Drs. Young Newton & Rakan-Rakan, Brickfields Drs. Young Newton & Rakan-Rakan, Damansara Drs. Young Newton & Rakan-Rakan, Jln. Ampang Elizabeth Medical Centre Sdn. Bhd. Gill Medical Centre Goay Klinik Goh Clinic Gul Medical Centre Healthcare Clinic Healthcare Medical Centre Horeb Sdn. Bhd. Jln. Ampang Horeb Sdn. Bhd. Leboh Ampang ING Insurance Berhad In-House Clinic Intan Poliklinik & Surgeri, Tmn. Arowana Island Klinik, Esplanade Island Klinik, Island Glades Jose Clinic & Surgery Kelinik & Surgeri Templer Kelinik Ganesan Sdn. Bhd. Kelinik Gopi, Jln. Market Kelinik Gopi, Tmn. Desa Permai Kelinik Liu Kelinik Ng Kelinik Poh Soon Sim Sdn. Bhd. Kelinik Ratna Kelinik S. Suren Kelinik Selvam Kelinik Thurai Kelinik Woo & Hong Khong Klinik Klinik Australia Klinik & Surgeri Bakti 65. 66. 67. 68. 69. 70. 71. 72. 73. 74. 75. 76. 77. 78. 79. 80. 81. 82. 83. 84. 85. 86. 87. 88. 89. 90. 91. 92. 93. 94 95. 96. 97. 98. 99. 100. 101. 102. 103. 104. 105. 106. 107. 108. 109. 110. 111. 170 Klinik & Surgeri Delima Klinik & Surgeri Dorai Klinik & Surgeri Dr. Harvinder Klinik & Surgeri Gill Klinik & Surgeri Lee, Seri Kembangan Klinik & Surgeri Lee, Taman Ros Klinik & Surgeri Ong Klinik & Surgeri Sipitang Klinik & Surgeri Stanley Chong Klinik & & Surgeri Guna Klinik & Surgeri Wisma Bersalin Bhajan Klinik Aisah Klinik Al’ Azhim, Klebang Klinik Al Farabi Jaya Gading Klinik Al-Azhim Tampin Klinik Ali Klinik Al-Insaan Klinik Alor Setar Klinik Amal Klinik Aman, Shah Alam Klinik Amardev & Surgery Klinik Aminah, Hulu Kelang Klinik Aminah, Pelabuhan Kelang Klinik Anis, Shah Alam Klinik Anita Klinik Anthony Klinik Ariffin Klinik Arun, Sentul Klinik Asean Klinik Asniza, Taman Pandan Permai Klinik Awana Kijal Klinik Baba Klinik Bala, Georgetown Klinik Bala, Paya Terubong Klinik Baling Klinik Ban Klinik Bandar Baru Klinik Bandar Raya Klinik Bandaran Sdn. Bhd. Jln. Bunga Melor Klinik Bandaran Sdn. Bhd. Section 15 Klinik Bandaran Sdn. Bhd. Section 25 Klinik Baru Jerteh Klinik Berkat Klinik Bersatu 16 Jam, Tmn. Chai Leng Klinik Bersatu Kulim Klinik Bersatu, Jln. Raja Uda Klinik Bersatu, Tmn. Ipoh Timur APPENDIX 1 Malaysian Statistics on Medicines 2006 PARTICIPANTS OF THE NATIONAL MEDICINES USE SURVEY Primary Care Clinics participating in NMUS survey # Private Clinics 112. 113. 114. 115. 116. 117. 118. 119. 120. 121. 122. 123. 124. 125. 126. 127. 128. 129. 130. 131. 132. 133. 134. 135. 136. 137. 138. 139. 140. 141. 142. 143. 144. 145. 146. 147. 148. 149. 150. 151. 152. 153. 154. 155. 156. 157. Klinik Bersatu, Tmn. Seruling Klinik Bintulu Klinik Boon Klinik Bukit Beruang Klinik Bukit Jambul Klinik Bukit Maluri & Surgeri Klinik C.F. Chong Klinik C.S. Ooi Klinik Care Poliklinik dan Surgeri Klinik Catterall, Khoo and Raja Malek, Bangunan Ming Klinik Ceria Klinik Chai Klinik Chan, Ipoh Garden Klinik Chang Klinik Chen Klinik Cheryan Klinik Chew Klinik Chiew Klinik Chin, Jln. Sultan Idris Shah Klinik Chon Klinik Chong, Kota Bharu Klinik Chong, Seremban Klinik Choo Klinik Chua, Ayer Tawar Klinik Chua, Sitiawan Klinik Cinta Sayang, Jln. Ibrahim Klinik Dan Surgeri Dr. Gan Klinik Dan Surgeri Putra Klinik Dan Surgeri Raju Klinik Dan Surgeri Soo Klinik dan Surgeri Sri Damansara Klinik Dedap Klinik Deepa Klinik Desa, Desa Petaling Klinik Doktor Wong - Dr. Wong Hua Seh Klinik Dorai Klinik Doshi Klinik Dr. (Mrs) Law Klinik Dr. Bazlan Klinik Dr. C.H. Kong Klinik Dr. Che Ku Klinik Dr. Cheu Sdn. Bhd. Klinik Dr. Chew Klinik Dr. Chin Kon Yoon Klinik Dr. Elvin Chong & Surgery Klinik Dr. Hamid 158. 159. 160. 161. 162. 163. 164. 165. 166. 167. 168. 169. 170. 171. 172. 173. 174. 175. 176. 177. 178. 179. 180. 181. 182. 183. 184. 185. 186. 187. 188. 189. 190. 191. 192. 193. 194. 195. 196. 197. 198. 199. 200. 201. 202. 203. 204. 171 Klinik Dr. Husna, Tmn. Ria Klinik Dr. Kamaludin Klinik Dr. Karim Klinik Dr. Lilian Hong Klinik Dr. Mohamad Klinik Dr. Najiha Klinik Dr. Rahim Omar & Rakan-Rakan Klinik Dr. Ramzi Klinik Dr. Roslan, Baling Klinik Dr. Roziah Klinik Dr. Shashikala Sdn. Bhd. Klinik Dr. Syed Klinik Dr. Ting Klinik Dr. Tuan Yusof Klinik Dr. Umi Klinik Dr. Wong & Dr. Lau Klinik Dr. Yong Klinik Dr. Aishah Dan Dr. Fisol Klinik Dr. S. Kumar Klinik Dr. Zakaria Klinik Eastern Klinik Efendi Klinik Ehsan Klinik Eirena Klinik Elizabeth, Tmn. Makmor Klinik Elopura Sdn. Bhd. - Jln. Tmn. Mawar Klinik Elopura Sdn. Bhd. - Sedco Complex Klinik Endau Klinik Everlasting Sdn. Bhd. Klinik Faiza Woon Klinik Famili TTDI Klinik Fateh Mohd & Rakan-Rakan Klinik Fauzi Klinik Fettes Park Klinik G.S. Klinik Ganesha Vijayam Klinik George Jinivon Klinik Glugor Klinik Gopeng Klinik Grace Klinik Gunn Klinik Gurdip Klinik Hafiz Klinik Halizah Klinik Hamidah Klinik Healthcare Klinik Hee Annandan Sdn. Bhd. APPENDIX 1 Malaysian Statistics on Medicines 2006 PARTICIPANTS OF THE NATIONAL MEDICINES USE SURVEY Primary Care Clinics participating in NMUS survey # Private Clinics 205. 206 207. 208. 209. 210. 211. 212. 213. 214. 215. 216. 217. 218. 219. 220. 221. 222. 223. 224. 225. 226. 227. 228. 229. 230. 231. 232. 233. 234. 235. 234. 235. 236. 237. 238. 239. 240. 241. 242. 243. 244. 245. 246. 247. 248. 249. Klinik Hemavathy Klinik Hikmah Klinik Hisham Klinik Hj. Ayaz Klinik Ho, Senai Klinik Hock-San Klinik Hon Klinik Hossana Klinik Hsu dan Ng Klinik H.T. Lee Klinik Husin Klinik Ian Ong Klinik Ibu Kota, Satok Klinik Idaman Klinik IHM Klinik Ikhwan & Surgeri Klinik Iman Klinik Imbi Klinik In-House Klinik Ishak Dan Surgeri Klinik J.D. Klinik Jaafar & Partners Klinik Jalan Templer Sdn. Bhd. Klinik Jauhar Klinik Jaya, Subang Jaya Klinik Jayaraman, Jln. Raja Laut Klinik Jelebu Klinik Jo Klinik Johor, Johor Jaya Klinik Joseph & Surgeri Klinik K.G. Mah Klinik K.I.P. Sdn. Bhd. Klinik K.J. Lim, Prima Setapak Klinik Kanta Klinik Kapar, Jalan Besar Kapar Klinik Karak Klinik Kaulsay Klinik Kayu Ara Klinik Keluarga Klinik Keluarga Aishah Klinik Keluarga Dan Surgeri Klinik Keluarga Dr. Hj. Mohd. Khadzali Klinik Khizan Klinik Koidupan Klinik Kok Klinik Kok Dan Surgeri Klinik Kok Dan Wendy, Klang 250. 251. 252. 253. 254. 255. 256. 257. 258. 259. 260. 261. 262. 263. 264. 265. 266. 267. 268. 269. 270. 271. 272. 273. 274. 275. 276. 277. 278. 279. 280. 281. 282. 283. 284. 285. 286. 287. 288. 289. 290. 291. 292. 293. 294. 295. 296. 172 Klinik Kok Dan Wendy, Subang Jaya Klinik Kok Wah Klinik Kok, Jln. 17/1A Klinik Kok, Jln. USJ 4/1 Klinik Kong Klinik Kuantan Klinik Kucai Klinik Kumpulan Muslimah Klinik Kwok Klinik Lahad Datu (Cawangan) Klinik Langkawi, Pusat Bandar Kuah Klinik Lau Klinik Lee, Petaling Jaya Klinik Leela Klinik Leong, Puchong Klinik Leong, Kuala Terengganu Klinik Leong, Tmn. Maluri Klinik Leow Klinik Liew & Surgeri Klinik Lim, Seremban Klinik Lim, Kuching Klinik Lim & Lau Klinik Lim Chin Chong Sdn Bhd Klinik Lim, Jln. Amarasegara Klinik Lin & Chandran Klinik Ling & Thoo Klinik Lo Klinik Low, Setapak Klinik Ludher, Jln. Kelang Lama Klinik M. Ghana Klinik Maamor Klinik Maharani Klinik Majid Klinik K.S. Tan Klinik K.V. Tan Klinik K.H. Ong Klinik Kalai Klinik Makbul Klinik Malaysia, Sibu Klinik Malaysia, Tampoi Klinik Maniraj Klinik Mansor Klinik Maranatha Klinik Maria, Keningau Klinik Maria, Seremban Klinik Mariam Klinik Masjid Tanah APPENDIX 1 Malaysian Statistics on Medicines 2006 PARTICIPANTS OF THE NATIONAL MEDICINES USE SURVEY Primary Care Clinics participating in NMUS survey # Private Clinics 297. 298. 299. 300. 301. 302. 303. 304. 305. 306. 307. 308. 309. 310. 311. 312. 313. 314. 315. 316. 317. 318. 319. 320. 321. 322. 323. 324. 325. 326. 327. 328. 329. 330. 331. 332. 333. 334. 335. 336. 337. 338. 339. 340. 341. 342. Klinik Medan Jaya Klinik Medic Bestari Klinik Medical Subang HI TEC Klinik Medicare, Jln. Bangsar Klinik Medijaya, Century Garden Klinik Medik 24-7, Bandar Country Homes Klinik Medimetro Klinik Melaka Klinik Melawati Klinik Mersing Klinik Mesra Klinik Mesra, Shah Alam Klinik Metro Medics, HICOM Industrial Estate Klinik Metro, Puchong Klinik Michael Wong Klinik Ming Klinik Mitter dan Rakan-Rakan Klinik Mogan Klinik Moorthy Klinik Muhibbah Klinik Muhibbah, Alor Setar Klinik Mutiara Inanam Klinik Naga Klinik Nagiah Klinik Najihah Klinik Nanda Klinik Nathan, Bgn. Mas Klinik Neoh Klinik Ng & Ng Klinik Ng, Jln. Kangsar Klinik Noh Klinik Noorleza Klinik Nur Aqila Klinik Nuraina Poliklinik & Surgeri Klinik Nuraini Klinik Ong & Surgeri Klinik Oziar Darus Klinik Pakatan Medik, Kuala Lumpur Klinik Pakatan Medik, Banting Klinik Panicker Klinik Pantai, Batu Ferringhi Klinik Pantai, Rantau Klinik Pantai, Tmn. Kota Lukut Klinik Papar Medical Group Klinik Perdana, Kuantan Klinik Perdana - Bgn. PKINK 343. 344. 345. 346. 347. 348. 349. 350. 351. 352. 353. 355. 356. 357. 358. 359. 360. 361. 362. 363. 364. 365. 366. 367. 368. 369. 370. 371. 372. 373. 374. 375. 376. 377. 378. 379. 380. 381. 382. 383. 384. 385. 386. 387. 288. 389. 390. 173 Klinik Perdana - Wisma Suara Muda Klinik Perdana, Islah Klinik Perdana, Jln. Lubok Stol Klinik Perdana, Lumut Klinik Perdana, Pusing Klinik Perkasa Klinik Permata Klinik Pertama, Johor Bahru Klinik Pertama, Georgetown Klinik Pertama, Sg. Besi Klinik Perubatan & Surgeri Dr. Ahmad Klinik Perubatan Chong Klinik Perubatan Lita Alis Klinik Perubatan Ong Klinik Petaling Jaya Klinik Poorni Klinik Prihatin Klinik Primecare, Phileo Corporate Park Klinik Public Klinik Pushpa Klinik Rabiah Klinik Radha, Bentong Klinik Radha Ampang Klinik Rahim Klinik Rahimah Klinik Rahmat Klinik Raj Klinik Raj (Jasin) Sdn. Bhd. Klinik Raj dan Rakan-Rakan, Sentul Klinik Raja, Ipoh Klinik Raju Klinik Rakyat, Gopeng Klinik Rakyat, Jln. Besar Kepong Klinik Rakyat, Jln. Telok Wanjah Klinik Rakyat, Taiping Klinik Rama Klinik Ramabai & Surgeri Sdn.Bhd. Klinik Rawatan Keluarga Klinik Rawatan Utama Klinik Razak Klinik Razana Klinik Reddy PJ Klinik Reddy Pudu Klinik Reddy Setapak Klinik Rembau Klinik Ria Klinik Roberts APPENDIX 1 Malaysian Statistics on Medicines 2006 PARTICIPANTS OF THE NATIONAL MEDICINES USE SURVEY Primary Care Clinics participating in NMUS survey # Private Clinics 391. 392. 393. 394. 395. 396. 397. 398. 399. 400. 401. 402. 403. 404. 405. 406. 407. 408. 409. 410. 411. 412. 413. 414. 415. 416. 417. 418. 419. 420. 421. 422. 423. 424. 425. 426. 427. 428. 429. 430. 431. 432. 433. 434. 435. 436. Klinik Rohana & Seripah Sdn. Bhd. Tmn. Seri Intan Klinik Roslina Klinik S.K. Leong Klinik S.K. Lo Sdn. Bhd. Klinik S.L. Ma Klinik Sabrina Klinik Sada Klinik Sanan Klinik Sandhu Senai Klinik Saujana, Melaka Tengah Klinik Saujana, Selayang Klinik Saujana, Sungai Buloh Klinik Segamat Klinik Segara, Jln. Bangsar Klinik Sekeluarga Ipoh, Fair Park Klinik Sekeluarga Ipoh, Tmn. Bukit Merah Klinik Senan Klinik Sentosa, Johor Bahru Klinik Sentosa, Kuala Berang Klinik Sentosa Sdn. Bhd. Lengkok Dumbar Klinik Sentosa, Penang Street Klinik Seremban, Bdr. Seremban Selatan Klinik Seremban, Senawang Jaya Klinik Seri Pulau, Jln. P. Ramlee Klinik Serijasa Klinik Setapak & Surgeri, Sri Rampai Klinik Setia Klinik Setiajaya Klinik Shafi, Jinjang Utara Klinik Shankar Sdn. Bhd. Klinik Shanraj Klinik Sharani Klinik Shatin Klinik Sibu Klinik Sidhu Klinik Sihat Putrajaya Klinik Sihat, Menggatal Oldtownship Klinik Simee Klinik Sinar Klinik Siti Zariah Klinik Siva & Surgeri Klinik Soo, Chemor Klinik Soon, Sibu Klinik Soon, Puchong Klinik Soong Klinik Sri Puteri 437. 438. 439. 440. 441. 442. 443. 444. 445. 446. 447. 448. 449. 450. 451. 452. 453. 454. 455. 456. 457. 458. 459. 460. 461. 462. 463. 464. 465. 466. 467. 468. 469. 470. 471. 472. 473. 474. 475. 476. 477. 478. 479. 480. 481. 482. 483. 174 Klinik Sri Sulong Klinik Subang Perdana Klinik Subra Sdn. Bhd. Klinik Subramaniam Klinik Suhaini Klinik Sukimi Klinik Sulaiman, Jengka Klinik Sulaiman, Jln. Tahan Klinik Sulaiman, Kompleks Teruntum Klinik Sulaiman, Maran Klinik Sungai Besar Klinik Syed Salleh & Rakan-Rakan Klinik Terengganu Klinik T.A.R. Klinik TA Klinik Taipan Klinik Tampin Klinik Tan, Melaka Klinik Tan Cheng Leng Klinik Tan, Bidor Klinik Tan, Sg. Petani Klinik Tawakal, Parit Sulong Klinik Teck Hoe Klinik Teh, Petaling Jaya Klinik Teh, Port Dickson Klinik Templer Klinik Tenaga Baru Klinik Tengku Amir Klinik Teo, Kota Kinabalu Klinik Teoh & Chan Sdn. Bhd. Klinik Ting Klinik Toh & Lim Klinik Tujuan Klinik Ummu Roihan Klinik Union 16 Jam, Tmn. Tangling Klinik Union 24 Jam Klinik Union, Hunza Complex Klinik Utama, Kepong Klinik Utama, Petaling Jaya Klinik Venka Klinik Vigneshwer Klinik Voon Klinik Wan Suhaimi Klinik Wang Klinik Wawasan 24 Jam Klinik Wawasan, Tmn. Sentosa Klinik Wee APPENDIX 1 Malaysian Statistics on Medicines 2006 PARTICIPANTS OF THE NATIONAL MEDICINES USE SURVEY Primary Care Clinics participating in NMUS survey # Private Clinics 484. 485. 486. 487. 488. 489. 490. 491. 492. 493. 494. 495. 496. 497. 498. 499. 500. 501. 502. 503. 504. 505. 506. 507. 508. 509. 510. 511. 512. 513. 514. 515. 516. 517. 518. 519. 520. 521. 522. 523. 524. 525. 526. 527. 528. 529. Klinik West Jelutong Klinik Wira Klinik Wong, Tawau Klinik Wong, Petaling Jaya Klinik Wong Ching Seh Klinik Y.M. Lo Klinik Yeoh Klinik Yii Klinik Yusof Klinik Zahar Klinik Zain & Zakaria, Batu Caves Klinik Zainab Klinik Zainiati Klinik Zaleha Kumpulan Medic, Shah Alam Kumpulan Medic, Subang Jaya Kumpulan Perubatan SMP Sdn. Bhd. (Klinik Pertama) LKB Clinic Loh & Lim Sdn. Bhd. MAA In House Clinic Maha Klinik Medi-Klinik Shahrol Medic-Klinik Lim Mediklinik Keluarga, Tmn. Ipoh Jaya Timur Mediklinik TTDI Jaya Merican Dispensary Ooi Kwee Lim Polyclinic Ophir Clinic Perak Medical Centre Sdn. Bhd. Kampar Perdana Polyclinics, Selayang Perdana Polyclinics Wilayah Poli Klinik, Jln. P. Ramlee Poliklinik & Surgeri Batu Gajah Poliklinik & Surgeri Chew Poliklinik & Surgeri Gul Poliklinik & Surgeri Seapark Poliklinik Al-Bukhari Poliklinik Al-Haj Poliklinik Aman Poliklinik An-Nisa Poliklinik Bahagia Poliklinik Bukit Mayang Emas Poliklinik Central & Surgeri, Jln. Gombak Poliklinik Chew & Rakan-Rakan Poliklinik & Surgeri Sentosa Poliklinik Damai & Surgeri, Tmn. Desa Jaya 530. 531. 532. 533. 534. 535. 536. 537. 538. 539. 540. 541. 542. 543. 544. 545. 546. 547. 548. 549. 550. 551. 552. 553. 554. 555. 556. 557. 558. 559. 560. 561. 562. 563. 564. 565. 567. 568. 568. 569. 570. 571. 572. 573. 574. 575. 576 175 Poliklinik dan Surgeri Ren-Ai Poliklinik Dinamik, Beranang Poliklinik Dinamik, Kajang Poliklinik Dinamik, Semenyih Poliklinik Dr. Azhar, Jeniang Poliklinik Dr. Norliza Poliklinik Family Poliklinik Fitrah, Bgn. PKNK Poliklinik Harmoni Poliklinik Hidayah, Bagan Serai Poliklinik Hidayah, Jln. Kuala Pilah Poliklinik Ihsan Poliklinik Jaya Poliklinik Kong Poliklinik Kumpulan City - Capital Square Poliklinik Kumpulan City - Dataran Templer Poliklinik Kumpulan City - Jln. Inai Poliklinik Kumpulan City - Jln. Pahang Poliklinik Kumpulan City - Tmn. Connaught Poliklinik Kumpulan City - Tmn. OUG Poliklinik Lai Poliklinik Liew Poliklinik Lim & Leong Poliklinik Lim & Pusat Rawatan Intan Poliklinik Mat Top Poliklinik Medic, Melaka Tengah Poliklinik Meranti Poliklinik Mindaku Poliklinik Murni Poliklinik Mutiara, Shah Alam Poliklinik Mutiara, Tmn. Desa Aman Poliklinik Ng Poliklinik Ong, Bt. Gajah Poliklinik Pan-Medic, Farlim Poliklinik Penawar Poliklinik Perdana Poliklinik Pertama Poliklinik Perubatan Kubang Pasu Poliklinik Putra, Kulim Poliklinik Raj Poliklinik Rajen Poliklinik Rakyat, Masjid Tanah Poliklinik Rakyat, Bahau Poliklinik Rakyat, Jln. Tuanku Munawir Poliklinik Rakyat, Putatan Poliklinik Rakyat, Tmn. Tasik Jaya Poliklinik Rama APPENDIX 1 Malaysian Statistics on Medicines 2006 PARTICIPANTS OF THE NATIONAL MEDICINES USE SURVEY Primary Care Clinics participating in NMUS survey # Private Clinics 577. 578. 579. 580. 581. 582. 583. 584. 585. 586. 587. 588. 589. 590. 591. 592. 593. 594. 595. 596. Poliklinik Raub & Surgeri Poliklinik Ravi Poliklinik S.M. Lee & Rakan-Rakan Poliklinik S. Naga, Tmn. Kluang Jaya Poliklinik Salehudin Poliklinik Samudera, Sitiawan Poliklinik Sandhu Poliklinik Sentosa Poliklinik Seri Mutiara Poliklinik Sg. Besi Poliklinik Simpang Pulai, Tmn. Bersatu Poliklinik Sri Permai Poliklinik Star Puchong Poliklinik Sungai Long Poliklinik Tang Poliklinik Tan, Lee & Cheong Poliklinik Teoh & Ding Poliklinik Zakariya Poliklinik Zul Dan Rakan-Rakan Sdn. Bhd. Poly Klinik dan Surgery Kampung Pandan 597. 598. 599. 600. 601. 602. 603. 604. 605. 606. 607. 608. 609. 610. 611. 612. 613. 614. 615. 616. Polyklinik Rajoo Pusat Rawatan Desa Pandan Pusat Rawatan Islam - Mais Sham Poliklinik Sdn. Bhd. Shri Senthil Clinic Sim’s Medical Clinic, Miri Siva Clinic Somu Kelinik Sushila Clinic Tejani Medical Centre Teow & Teo Medicare Sdn. Bhd. The Key Clinic The People’s Dispensary Sdn. Bhd. Johor Bahru Tiram Medical Centre Uma Klinik Union Clinic, Bau Vaithiyanathan Clinic Victor Medical Practice Yoong Clinic Sdn. Bhd. 17. Farmasi Alychem Sdn. Bhd. - Sg. Long, Kajang Farmasi Apollo Farmasi Bakti Sdn. Bhd. Farmasi Bintang Farmasi Carrie Farmasi Chia Farmasi Gamma Farmasi Kemuning Farmasi Komuniti UKM Farmasi Lim Farmasi Nazifa Farmasi Pendang Farmasi Rantau Farmasi Ruby Farmasi S.J. Sdn. Bhd. Farmasi Teck Hong Farmasi USJ Sdn. Bhd. Farmasi Utara Sdn. Bhd. Pharmacies participating in NMUS survey # Private Pharmacies 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. 14. 15. 16. Alpro Pharmacy Holdings Sdn. Bhd. Damansara Apo’s Pharmacy Bahau Pharmacy Sdn. Bhd. Balik Pulau Health-Care Baling Pharmacy Sdn. Bhd. C.S. Lo Pharmacy Carene Pharmacy CL SU Pharmacy Sdn. Bhd. Daya Pharma Sdn. Bhd. Delima Farmasi Sdn. Bhd. Excelcare Pharmacy Far East Pharmacy Sdn. Bhd. Farmasi Al-Nabilah Farmasi Alychem Sdn. Bhd. - Bdr. Baru Sg. Buloh Farmasi Alychem Sdn. Bhd. - Payar Jaras, Sg. Buloh Farmasi Alychem Sdn. Bhd. - Selayang, Batu Caves 18. 19. 20. 21. 22. 23. 24. 25. 26. 27. 28. 29. 30. 31. 32. 33. 34. 176 APPENDIX 1 Malaysian Statistics on Medicines 2006 PARTICIPANTS OF THE NATIONAL MEDICINES USE SURVEY Pharmacies participating in NMUS survey # Private Pharmacies 35. 36. 37. 38. 39. 40. 41. 42. 43. 44. 45. Farmasi Voon Gaya Pharmacy Supplies GP Pharmacy Health-Care Pharmacy Jitra Pharmacy Sdn. Bhd. Joy Pharmacy K.H. Hoe Pharmacal Sdn. Bhd. Karamunsing Pharmacy Sdn. Bhd. KNL Medicare Kumpulan Farmasi Vitacare Sdn. Bhd. Mico Farmasi Sdn. Bhd. 46. 47. 48. 49. 50. 51. 52. 53. 54. 55. 56. Others 1. Ministry of Foreign Affairs. 177 Nori Care Pharmacy Pahang Pharmacy Sdn. Bhd. - Karak Pharmachem Labuan Sdn. Bhd. Pusat Farmasi USM (Kedai Koop) Remedy Pharmacy Rheco Pharmacy Sentosa Pharmacy Sungai Siput Pharmacy Yin Woh Tong Medical Supply Sdn. Bhd. YW Yong Farmasi Sdn. Bhd. Zuffa Pharmacy Sdn. Bhd. – Jln. Petani






























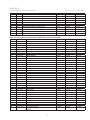

















































































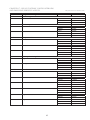





























































![My_Body[1] - Junior2TopicWiki](http://s1.studyres.com/store/data/008060165_1-be31cd2568d5e2c9fee6ce67732b07b4-150x150.png)









